Article Text

Abstract
Background Our 2012 review on therapeutic interventions for acute hamstring injuries found a lack of high-quality studies. The publication of new studies warranted an update.
Objectives To update and reanalyse the efficacy of conservative treatments for hamstring injury.
Data sources PubMed, EMBASE, Web of Science, Cochrane library, CINAHL and SPORTDiscus were searched till mid-February 2015.
Study eligibility criteria Randomised controlled trials (RCTs) on the effect of conservative interventions versus a control group or other intervention for hamstring injuries (HI) were included.
Data analysis The search results were screened independently by two authors. Risk of bias assessment was performed using a modified Downs and Black scale with a maximum score of 28. Meta-analysis was performed, where possible.
Main results 10 RCTs (526 participants), including 6 new RCTs, were identified. Two RCTs were of good/excellent quality, the rest were fair or poor (median Downs and Black score 16 (IQR 9)). Meta-analysis of two studies on rehabilitation (lengthening) exercises showed a significantly reduced time to return to play (HR 3.22 (95% CI 2.17 to 4.77), p<0.0001) but no difference in risk of re-injury. Meta-analysis of three studies investigating platelet-rich plasma (PRP) showed no effect when compared to control (HR 1.03 (95% CI 0.87 to 1.22), p=0.73). Limited evidence was found that progressive agility and trunk stability training may reduce re-injury rates.
Conclusions Meta-analysis showed superior efficacy for rehabilitation exercises. PRP injection had no effect on acute hamstring injury. Limited evidence was found that agility and trunk stabilisation may reduce re-injury rates. The limitations identified in the majority of RCTs should improve the design of new hamstring RCTs.
- Hamstring
- Injuries
- Platelet-Rich Plasma
- Physiotherapy
- Review
Statistics from Altmetric.com
Introduction
In 2012, we systematically reviewed the evidence for conservative interventions in the treatment of acute hamstring injuries (HI).1 We found limited evidence to support the use of agility and trunk stabilisation, (slump) stretching and Actovegin injections.1 Limited evidence was found that sacroiliac manipulations and non-steroidal anti-inflammatory drugs (NSAIDs) were not effective.1 Since the publication of this review, several new randomised controlled trials (RCTs) have been published. After the 2012 Cochrane review of Mason et al2 no new systematic reviews have been published warranting an update.
Given the new evidence, we adjusted the inclusion criteria of our original review1 to include only RCTs. The purpose of this updated systematic review is to reassess the available literature concerning the conservative management of HI, to review their efficacy and perform meta-analysis, where possible.
Materials and methods
Literature search
A literature search was performed in mid-February 2015 in PubMed, EMBASE, Web of Science core collection, Cochrane library, CINAHL and SPORTDiscus. A modified version of the 2012 search was used (see online supplementary appendix 1). Searches were performed by one author (HP) with no limits. The references of the selected articles were manually searched for additional references.
All studies identified by the search were imported in a citation database (EndNote 7.1, Thomson Reuters, New York, USA) and duplicates were removed. Additionally, co-authors of this review, with a specific interest in hamstring injury, were asked about internationally known recently completed and/or submitted RCTs up to February 2015.
Study selection
All titles were screened by two independent assessors (HP and JLT). Full texts of possibly eligible articles were obtained and assessed independently using the inclusion criteria presented in box 1. Both reviewers compared the articles identified and consensus was reached. If no consensus was reached, a third reviewer (MHM) was consulted.
Inclusion criteria
Participants in the study had an acute hamstring injury, diagnosed by physical examination, MRI or ultrasound
The studies included were randomised controlled trials
There was a well-described conservative therapeutic intervention which was compared to another intervention or a control group
Full text of the article was available
The article was written in English, German or Dutch
In the article at least one of the following outcome measures had to be reported:
Time to return to sport or normal function
Re-injury rate
Pain scores
Hamstring force: isometric or isokinetic testing
Hamstring flexibility testing
Patient satisfaction
Adverse effects
Data extraction
Using a standardised data extraction form, study characteristics, patient characteristics and outcome measures were recorded by one author (HP). Point measures and estimations of variance of the selected outcomes were recorded to evaluate therapy efficacy. In the case of multiple measurements, the data of the last measurement were used. If necessary, authors were contacted for additional data.
Quality assessment
Two reviewers (MHM and GR) independently assessed the selected studies for risk of bias using a modified version of the Downs and Black scale (D&B)3 (see online supplementary appendix 2). The original scale consists of 27 questions and allows a maximal score of 32 points. Based on previous literature we modified this scale to a 28-point scale4–7 by converting it to a binary scale and by adding one additional question evaluating therapist blinding. This was identified as an important form of bias based on the studies we identified in our previous review.1 Most studies evaluated physical therapy interventions or complementary therapies, adding a possibly biased party if he/she was not blinded. Especially in return to play (RTP) decision-making, lack of therapist blinding is an important source of bias.8 One point was given if therapist blinding was ensured. Lastly, question 21 was only scored when both time to RTP and re-injury rate were reported in the trial. This was done because we feel that trials reporting both these outcome measures give a more complete and less biased outcome of the therapy success.1
A maximum of 28 points could be scored. We adopted the following quality levels based on previous literature4 ,5 ,7: excellent (26–28); good (20–25); fair (15–19) and poor (≤14).
If there was a difference in opinion on a D&B item score, consensus was reached by consulting a third reviewer (JLT). When at least one of the primary D&B assessors was involved as co-author in the RCT, an independent experienced assessor (AS), scored it as the third assessor.
Data synthesis
One author (HP) calculated weighted means and SDs for demographic information using SPSS V.22.0 (IBM statistics, New York, New York, USA). After assessing normality using the Kolmogorov-Smirnov (p<0.05) test mean or median, D&B scores were calculated.
We considered pooling data when studies were sufficiently statistically and clinically homogeneous (ie, intervention and outcome). Data pooling was carried out with RevMan V.5.3 (The Nordic Cochrane Centre, Copenhagen, Denmark) by two authors (HP and MW). We calculated hazard ratios (HR) with 95% CI for time-to-event data. HRs were calculated such that HR>1 indicated faster RTP in the treatment group as compared to the control group. Risk ratios (RR) with 95% CI were calculated for dichotomous outcomes. RR<1 expressed a smaller risk for re-injury in the treatment group as compared to the control group. A fixed effects model was used to pool data when studies were statistically homogenous. We visually inspected the forest plots for heterogeneity, along with the I2-statistic which was considered to represent substantial heterogeneity for I2>50%.9 Heterogeneity was considered present when the χ2 was significant (p<0.1).9 We planned a metaregression analysis or subgroup analysis when statistical heterogeneity was present and ≥10 studies were available. A random effects model was used when statistical heterogeneity was present. However, when <5 studies were available for data synthesis we used a fixed effects model.
We planned a sensitivity analysis to explore the effect of study quality by excluding studies with low D&B scores (<20) from the meta-analysis.
If meta-analysis was not possible, a qualitative analysis of the data was carried out using the five levels of evidence used in 2012.1 ,10 Meta-analysis was considered superior to qualitative levels of evidence.
Strong evidence: provided by two or more studies with high quality and by generally consistent findings in all studies (≥75% of the studies reported consistent findings).
Moderate evidence: provided by one study with high quality and/or two or more studies with low quality, and by generally consistent findings in all studies (≥75% of the studies reported consistent findings).
Limited evidence: provided by only one study with low quality.
Conflicting evidence: inconsistent findings in multiple studies (<75% of the studies reported consistent findings).
No evidence: when no studies could be found.
We evaluated the possible presence of publication bias in this review by assessing the symmetry of the funnel plot.
Results
Literature search
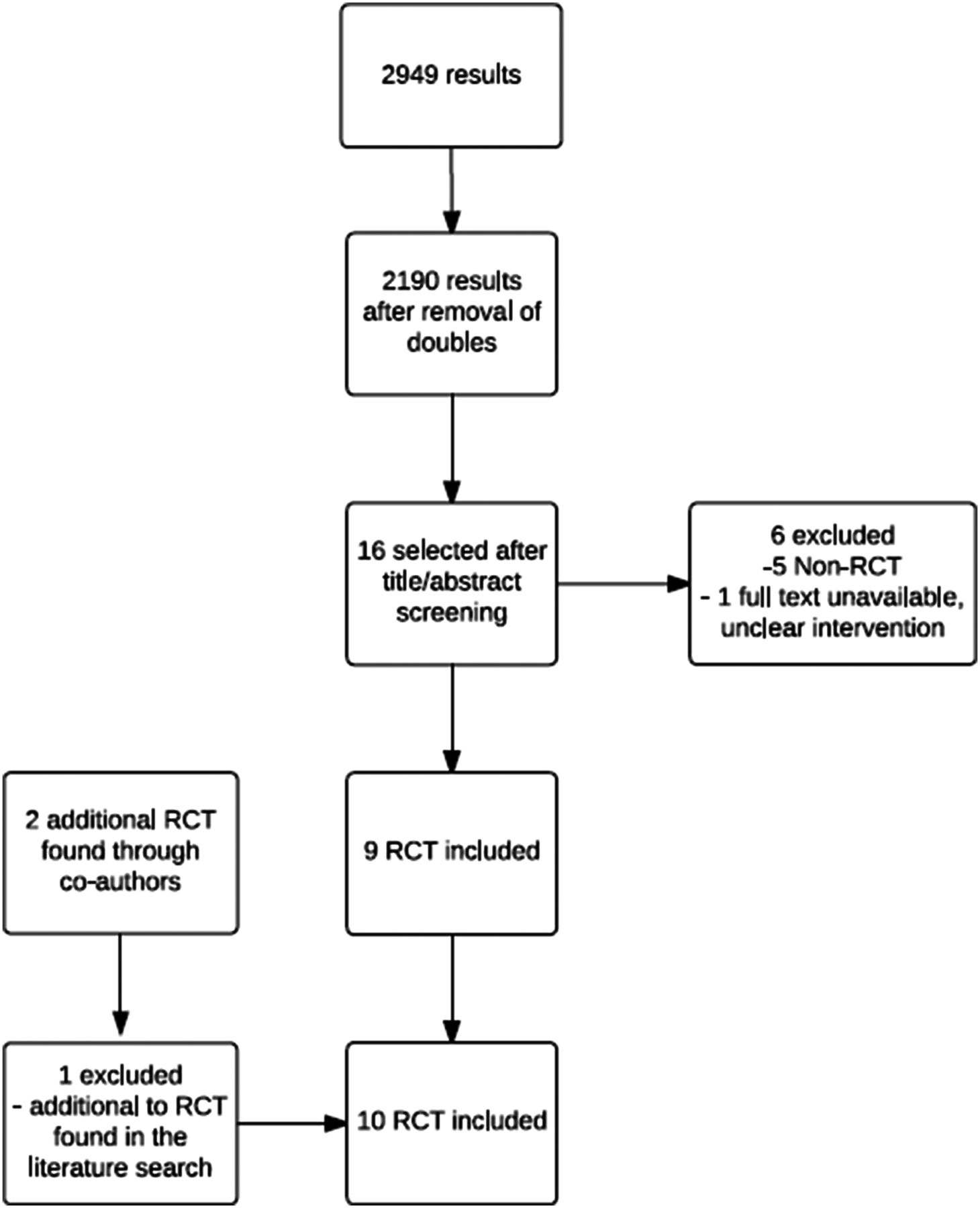
In total 2190 titles and abstracts were screened; 16 studies were selected for full-text assessment. Reference tracking yielded no additional titles. After full-text assessment, six studies were excluded11–15 and nine studies met the inclusion criteria.16–24 Two, at that time unpublished, articles were found through co-authors (JLT and GR).25 ,26 The manuscripts were obtained with permission of the authors. One of these trials26 reported the secondary outcomes of a trial identified in the literature search;24 we did not consider it as a separate trial, but rather as additional information of the first trial.24 Figure 1 illustrates the selection process.

Flow chart of article selection (RCT, randomised controlled trial).
Description of the included studies
The funnel plot showed no evidence of publication bias when taking the symmetrical distribution of the studies in the funnel plot (figure 2) into account.
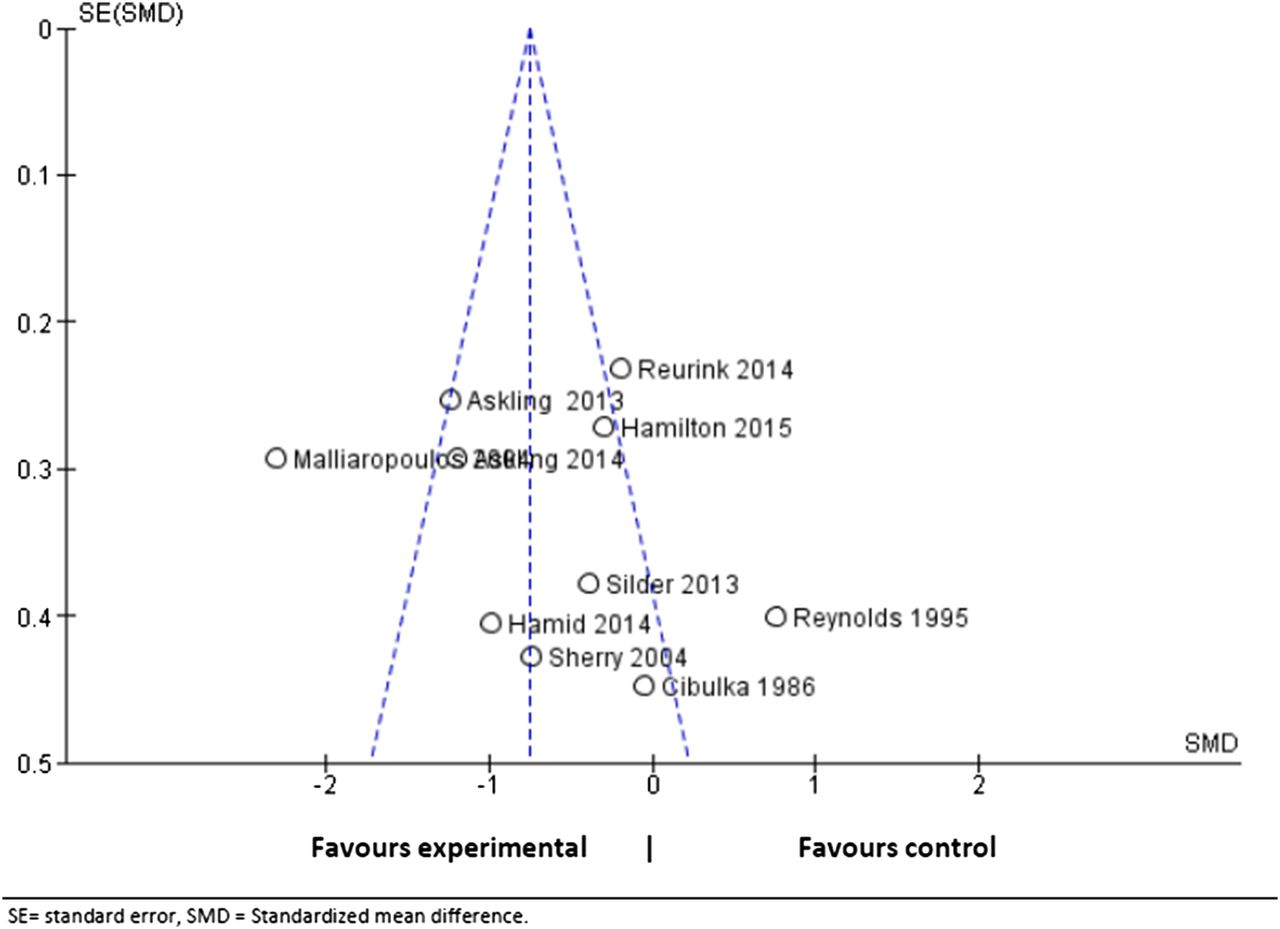
Publication bias funnel plot.
Table 1 summarises the characteristics of the included studies. Compared to 2012,1 two case–control trials were not evaluated13 ,27 and six new RCTs were found.20–26 Five studies21–26 were rated as homogenous and judged to be suitable for meta-analysis. The data of these trials were pooled per intervention.
Article characteristics
Quality assessment
Table 2 shows the overall D&B scores (detailed information in online supplementary appendix 3). Scores ranged from 14 to 27 with a median of 16 (IQR 9). One three-arm RCT was given two separate D&B scores25 as it used two different control interventions which were blinded in different ways. The third assessor was asked to assess all trials concerning questions 11–13 which were found to be highly subjective. An independent assessor (AS) was asked to score one trial,24 ,26 as the primary D&B assessors were involved as co-authors in the trial. The total score of the independent assessor was identical to our consensus assessment though there was a slight variance between individual items (see online supplementary appendix 3).
Total D&B scores (maximal 28)*
Participants
A total of 526 participants were included with a mean of 65 (SD 23) per study. The mean and median ages reported across the studies ranged between 20 and 32 years. The majority of participants were males comprising a weighted mean of 86% (SD 13) of the population (range 65–100). Participants from different sports were used in seven studies,17–20 ,23–26 two studies used a specific sport population,21 ,22 one study did not explicitly mention using a sporting population.16
Table 3 summarises the examinations performed on patients to diagnose hamstring injury.
Clinical examinations used to diagnose hamstring injury
Interventions and outcomes
Table 4 summarises the interventions used in the studies, the outcomes that were measured and their effect. Two studies evaluated the efficacy of exercises aimed at loading and lengthening the muscle during eccentric actions in addition to a physiotherapy programme.21 ,22 Two studies assessed a physical therapy programme focused on agility and trunk stabilisation.19 ,20 Three studies compared platelet-rich plasma (PRP) injections and a standardised physiotherapy programme with placebo injections, platelet-poor plasma injections or no injection.23–26 The remaining studies examined the efficacy of stretching,18 sacroiliac manipulation16 and the use of NSAIDs (meclofenamate and diclofenac).17
Interventions and outcomes of RCTs
Data synthesis
We performed a meta-analysis on five studies.21–25 Two studies evaluated the effect of a partially supervised physiotherapy programme21 ,22 with either a lengthening protocol (L-protocol) or a conventional protocol (C-protocol). Of the three RCTs evaluating the efficacy of PRP injections in addition to physiotherapy, we did not pool the platelet-poor plasma data from Hamilton et al25 due to doubts about the validity and the unknown effects of this product.
Two studies19 ,20 evaluating physical therapy programmes based on agility and trunk stabilisation were not pooled because of differences in the content of the intervention and control programmes.
Meta-analysis: lengthening exercises (also referred to as ‘rehabilitative’ for the general reader)
Askling et al21 ,22 evaluated the effect of adding exercises aimed at progressively loading the injured muscle (L-protocol) to a conventional physiotherapy programme. The hamstrings were lengthened extensively during eccentric muscle actions. This was compared to exercises which had less emphasis on muscle lengthening (C-protocol). Both protocols contained three types of exercises aimed at increasing flexibility, strengthening the muscle, and a combination of strengthening and trunk/pelvic stabilisation, but the exact exercises differed between groups. Both groups received a standard general rehabilitation programme in addition to their exercises (checked with the author). Patients were cleared for return to sport when there were no signs of injury during physical examination and when they could perform the Askling H-test (a rapid straight leg raise in a special knee brace) without hesitation.28 Additional data from the author was requested for meta-analysis.
Fixed effects models were used to estimate the effect of the L-protocol versus the C-protocol for RTP (number of days) and risk of re-injury (figure 3A, B). The pooled effect showed that the L-protocol significantly reduced RTP compared to the C-protocol with an HR of 3.22 ((95% CI 2.17 to 4.77), Z=5.83, p<0.0001) (figure 2). No difference was found between the two protocols for the risk of re-injury ((RR)=0.25, 95% CI 0.03 to 2.20, Z=1.25, p=0.21) (figure 3). No statistical heterogeneity was present (I2=0%).
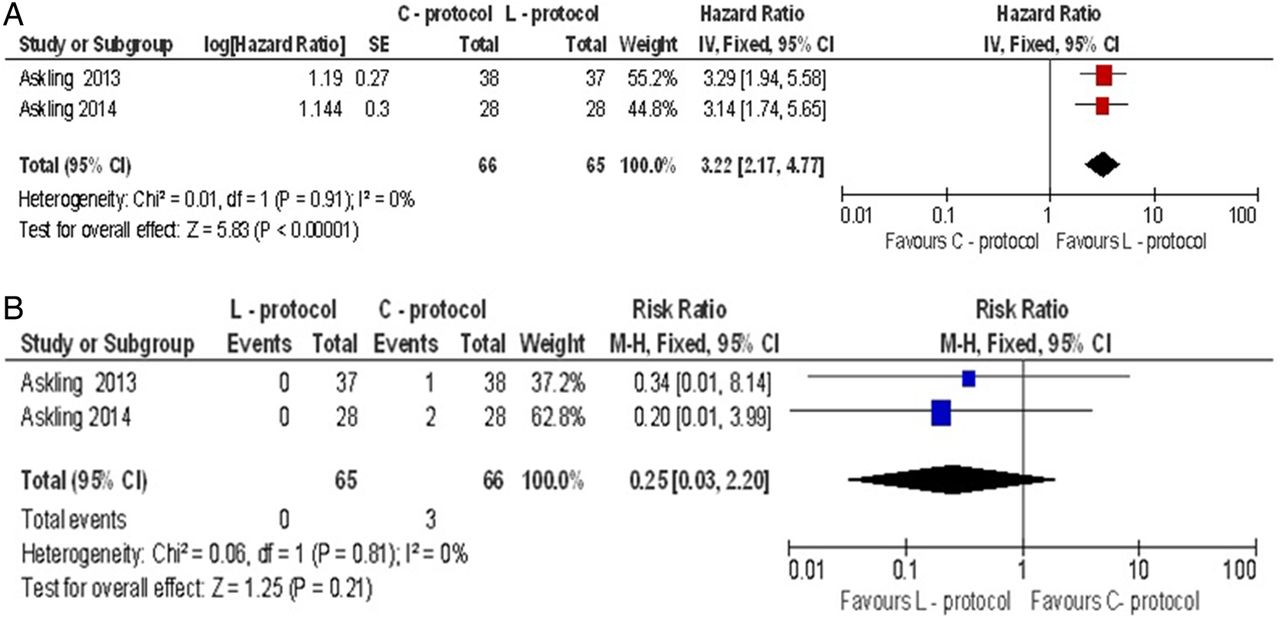
(A) Pooled HRs of return to play for adding lengthening exercises (L-protocol) and conventional exercises (C-protocol) Log natural logarithm; IV, inverse variance;, square size indicates the size of the population investigated in each study; diamond estimated pooled effect: width indicates the 95% CI. (B) Pooled risk ratio for re-injury (<1 year) for adding lengthening exercises (L-protocol) and conventional exercises (C-protocol). square size indicates the size of the population investigated in each study; diamond estimated pooled effect: width indicates the 95% CI.
Meta-analysis: PRP
Three studies evaluated the effect of PRP injections23–25 with standardised rehabilitation. Hamid et al23 performed an assessor-blinded study comparing patients receiving a single 3 mL PRP injection (Biomet, mean 1297×103 platelets/μL, mean 38.3×103 leucocytes/μL) within 7 days after injury, to patients who received no injection. Both groups followed a standardised rehabilitation programme. Hamilton et al25 performed a double-blinded trial comparing one 3 mL injection of PRP (Biomet, mean 765.8±423.6×103 platelets/μL, mean 26.1± 13.7×103 leucocytes/μL) and platelet-poor plasma (mean 30.3± 23.0×103 platelets/μL, mean 0.03±0.03×103 leucocytes/μL) within 5 days after injury and a single-blinded comparison study arm with no injection. All three groups underwent a six-stage criteria-based standardised rehabilitation. All treating physiotherapists were blinded for group allocation and MRI findings. Patients were randomised to receive either 3 mL of PRP or platelet-poor plasma or no injection. Reurink et al24 ,26 undertook a double-blind RCT in which patients were randomised to receive either two injections with 3 mL of PRP, respectively, within 5 days after injury onset and 5–7 days after the first injection (Arthrex mean 433±128×103 platelets/μL, mean 1.9± 2.1×103 leucocytes/μL), or saline placebo injections in addition to a standardised rehabilitation programme.
The D&B scores of the trials differed. Two24–26 were rated as good or excellent (D&B scores 25 and 24/27, respectively) and one23 as fair (D&B 19). We, therefore, performed a sensitivity analysis.
A fixed effects model was used to estimate the HR of RTP in the PRP group compared to the non-injected control group. The pooled effect showed no significant effect of PRP compared to control with an HR of 1.03 ((95% CI 0.87 to 1.22), Z=0.35, p=0.73) (figure 4A). There was substantial heterogeneity (I2=75%), which was significant (p=0.02). Sensitivity analysis revealed that the decision of including high risk of bias studies in the meta-analysis did not affect the effect of PRP when compared to including low risk of bias studies only. When analysing low risk of bias studies only, the HR was 1.00 ((95% CI 0.85 to 1.19), Z=0.04, p=0.97) (figure 4B). The risk of re-injury at 6 months was pooled for two trials24–26 as one trial23 did not report re-injury. This showed no difference between PRP and control (RR=0.88, (95% CI 0.45 to 1.71), Z=0.39, p=0.70) (figure 4C). No heterogeneity was present for re-injury. Owing to the small number of studies investigating the interventions, no meta-regression or subgroup analysis was possible.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Pooled HRs for return to play for platelet-rich protein (PRP) and control interventions. Log natural logarithm; IV, inverse variance; square size indicates the size of the population investigated in each study; diamond estimated pooled effect: width indicates the 95% CI. Data using platelet-poor plasma (PPP) as control were excluded from analysis. (B) Sensitivity analysis, the HR for return to play for PRP and control based on high-quality randomised controlled trials (RCTs) only. Log natural logarithm; IV, inverse variance; square size indicates the size of the population investigated in each study; diamond estimated pooled effect: width indicates the 95% CI. Data using platelet-poor plasma (PPP) as control were excluded from analysis. (C) Pooled risk ratio for re-injury for platelet-rich plasma (PRP) and control. IV, inverse variance; square size indicates the size of the population investigated in each study; diamond estimated pooled effect: width indicates the 95% CI. Data using platelet-poor plasma as control were excluded.
Descriptive synthesis
Progressive agility and trunk stabilisation
Two studies19 ,20 evaluated a rehabilitation programme, which focused on progressive agility and trunk stabilisation (PATS).
Sherry and Best19 compared PATS to a rehabilitation programme focusing on stretching and strengthening (STST). Both programmes consisted of two discrete phases. Compliance was monitored through self-recorded exercise logs. A mean of 22.2 days (SD 8.3) for the PATS group and 37.4 days (SD 27.6) for the STST group was reported, which was not statistically significant (p=0.2455). Re-injury rates between groups were statistically significant in favour of PATS (0/13 re-injuries within 16 days after RTP and 1/13 within 1 year, vs 6/10 and 7/10, respectively in the STST group (p<0.001 in both cases)).
Silder et al20 compared PATS with a progressive running and eccentric strengthening (PRES) programme. Both programmes consisted of three phases. No statistically significant difference in RTP was found (PATS: mean of 25.2 days (SD 6.3), PRES: 28.8 days (SD 11.4), p=0.346). Re-injury rates were 1/16 in the PATS and 3/13 for the PRES group. Significance was not reported. Several other outcome measures based on MRI finding and physical examination were reported in the study. Of these, only the craniocaudal length of injury at RTP on MRI was significantly shorter for the PATS group at RTP (p=0.037).
Stretching
Malliaropoulos et al18 compared two different intensities of static stretching (four times vs once daily) in 80 patient with grade 2 hamstring injury. Full active knee extension was reached earlier in the high-intensity group with a mean of 5.57 (SD 0.71) days vs 7.32 (SD 0.53) days (p<0.001). Time to RTP was shorter in the high-intensity group (mean of 13.27 days (SD 0.71) days compared to 15.05 (SD 0.81) days (p<0.001)).
Sacroiliac manipulation
Cibulka et al16 found no effect of sacroiliac manipulation on peak quadriceps torque and passive knee extension after manipulation compared to non-manipulated controls. A significant difference in peak torque change was reported in favour of manipulation (8.1 (sacroiliac mobilisation group) vs 0.4 ft lbs (control)). It should be noted that significantly lower pre-test peak torques of the experimental group were reported (8.4 ft lbs lower, p<0.005).
Non-steroidal anti-inflammatory drugs
Reynold et al17 evaluated the effect of 50 mg meclofenamate and placebo (group 1) versus 25 mg diclofenac twice daily, and placebo (Group 2) versus placebo only (group 3) for a period of 7 days. No significant effects on pain scores (measured with a visual analogue scale), swelling and isokinetic hamstring tests (peak torque, total work and average power) were found. Adverse events were reported in 5/13 patients in group 1, 6/17 in group 2 and 2/14 in group 3. None of these required alteration or reduction of the medication. Statistical analysis was not performed for adverse events.
PRP injections
Hamid et al23 found that although the PRP group showed significantly lower pain severity scores during the rehabilitation, it had no effect on change in pain scores or pain intensity scores. No adverse events were reported. Re-injury rates were not reported.
Both Hamilton et al25 and Reurink et al24 ,26 found no significant differences between other secondary outcomes. Both reported no significant adverse events.
Hamilton et al25 found that RTP in the platelet-poor plasma group was significantly longer when compared to PRP (−5.7 days ((95% CI −10.1 to −1.4), p=0.01). No difference was found between platelet-poor plasma and no injection (2.8 days (95% CI −1.6 to 7.2), p=0.210).
Discussion
Main findings
We systematically reviewed 10 RCTs that evaluated the effects of different interventions for acute hamstring injuries. These studies were generally of fair quality with one poor quality18 and two good/excellent quality studies.24–26 The poor-quality and fair-quality studies mostly lacked adequate blinding, were underpowered and did not properly adjust for loss to follow-up. Based on the meta-analysis of two studies of fair quality,21 ,22 we found that adding lengthening exercises reduce the time to RTP when compared to conventional exercises. Meta-analysis of the PRP trials23–26 showed no additional effect for PRP injections on RTP or in reducing re-injury. For re-injury reduction, limited evidence from one trial19 was found for agility and trunk stabilisation exercises; however, moderate evidence from two fair quality trials19 ,20 showed no reduction in time to RTP for these exercises.
Limited evidence, through one poor-quality study,18 is available to support high-frequency compared with low-frequency stretching in grade 2 HI. Based on fair-quality studies, limited evidence is available that NSAIDs17 and sacroiliac mobilisation16 have no therapeutic effect in acute hamstring injury rehabilitation.
Physical therapeutic interventions
Meta-analysis showed that adding lengthening exercises to a standard physical therapy programme was more effective than using conventional exercises in reducing time to RTP, but had no effect on re-injury rate. These results should be interpreted with care and require reproduction by other research groups and different athlete populations. It should also be noted that both trials were unblinded and the D&B scores indicate that both trials were of fair quality (D&B scores of 15) making them prone to detection and performance bias. Several differences were found between trials (unequal male/female distributions, age, proportion of stretch type injury, length of injury and sports type) but these did not influence statistical heterogeneity of the data.
We found moderate evidence that PATS does not reduce the time to RTP. Both studies19 ,20 used different control (STST and PRES) interventions and the content of the PATS programmes differed (two vs three phases). It should also be noted that both trials used small sample sizes (n=2419 and n=2920). Sherry and Best19 did prove its superiority over STST with regard to re-injury rate. However, as previously observed,1 the re-injury rate in the STST group was remarkably high (70%), suggesting a possible adverse effect of this programme.
We found limited evidence that static stretching four times a day was superior to once daily stretching.18 No other studies evaluated static stretching or used it as a control making it impossible to state whether stretching itself is efficacious.
Platelet-rich plasma
Our meta-analysis and descriptive synthesis show that there is no superior efficacy for PRP injections. The results from the meta-analysis should be considered carefully as there is substantial heterogeneity in the data. First, two trials23 ,25 used a non-blinded, no injection group as control whereas Reurink et al used a blinded placebo group (saline) as control group,24 ,26 allowing for performance bias in the results. This actually strengthens the results presented because no effect could be found despite the presence of bias. Second, all trials differed slightly in injection techniques and PRP content. Third, we did not pool the platelet-poor plasma data from Hamilton et al25 because there were concerns about its validity as placebo. There is little experience with platelet-poor plasma and due to its content (pH, osmolality, remaining leucocytes and platelets), myotoxic effects cannot be excluded and its enhancing effect remains unclear. Saline was considered a more valid placebo as ample evidence is available that it has no myotoxic effect on muscle tissue.29 Lastly, there were differences in patient characteristics. Thus, no meta-regression or subgroup analysis was possible to investigate the effect of patient characteristics.
The RCTs by Reurink et al24 ,26 and Hamilton et al,25 were of high quality. Please note that members of this review group are co-authors of these studies. The D&B score of the independent assessor (AS) was comparable and did not affect the quality category of Reurink et al24 ,26 (good) and the co-author involved with the Hamilton et al25 trial (JLT) was not involved in the D&B scoring.
Hamid et al23 reported that PRP shortened the time to RTP. The PRP preparation in this study had the highest platelet count (1297×103/μL). However, this study risked bias due to a lack of a placebo or any attempt to mask the lack of injection allowing for a placebo effect among patients. Re-injury rates were not reported, making the assessment of a possible premature RTP and the long-term efficacy impossible.
Several previous reviews30–33 have found a dearth of evidence to support PRP as a treatment for muscle injury. Considering our quantitative and qualitative findings, higher levels of evidence are now available to discourage the use of PRP injections in the rehabilitation of hamstring injuries.
Other interventions
Limited evidence was found that NSAIDs17 and sacroiliac manipulation16 have no effect on outcome. Furthermore, the study by Cibulka et al16 contains several methodical shortcomings (unclear definitions, differences in baseline characteristics) making it prone to bias. Also, its findings with regard to hamstring peak torque can be explained by the difference in pre-test peak torques between groups.
NSAIDs are often proposed as an analgesic in the early phase of muscle injury.34–37 Although the evidence is limited,17 we found no evidence to support the use of NSAIDs for pain management. Furthermore, there is increasing evidence that NSAIDs may be counterproductive for muscle healing.29 Considering the lack of support for their efficacy and the possible detrimental effect on muscle healing, NSAIDs are not recommended in HI.
Limitations
Our review has several limitations. First, we did not perform a grey literature search. We did find one on-going trial through the co-authors. It is possible that other pending trials are available.
Second, we used a modified D&B scale to assess the quality in trials. In 2012, the PEDro scale was used1 making comparison of the trial quality more difficult. However, the association between both scales was previously found to be moderately high (r 0.71, p<0.01)38 and after the modifications to our D&B scale, all questions from the PEDro scale were assessed as part of the D&B. We, therefore, feel that the use of our modified D&B scale was valid. We compared the effect on quality assessment between both scales and found no difference in 50%. In the remaining 50%, the PEDro scale always showed higher quality ratings, suggesting our current review was more critical in assessing the available evidence.
We altered a few keyword combinations because we found that the original search included too many irrelevant articles and that the number of hits using this search had in some cases quadrupled. Each alteration was checked for potentially missed articles. We are confident that no relevant articles were missed.
Lastly, we excluded all clinical controlled trials since enough RCTs were now available to focus specifically on randomised studies, adding to the level of evidence of this review. Owing to this exclusion criterion, two treatment options were not reviewed compared to 2012.1
Updated clinical relevance: what should be implemented in clinical practice
New evidence is available to assist in clinical decision-making for the treatment of hamstring injuries. Askling's et al21 ,22 lengthening protocol enhances RTP compared to conventional therapy (meta-analysis), and PATS might be implemented for reducing the re-injury rate (limited evidence). Statistical evidence suggests that PRP injections have no added effect on RTP or re-injury rate (meta-analysis).
Future directions
The quality of the RCTs included was generally relatively low. The main areas that the studies failed to address in their designs were lack of blinding, sample size and adjustment for loss to follow-up.
Most RCTs had a risk of bias due to lack of blinding of patients and/or therapist. Although it is difficult to blind therapists in physiotherapy studies, every attempt should be made to make this possible. If this is not possible, the use of strict criteria for progression during a rehabilitation programme should be used to minimise performance bias. Blinding of assessors and patients should also be ensured. When evaluating adjuvant treatment, such as PRP, we believe the use of placebo is imperative.
The comparability between trials was poor. Although most trials evaluated a physical therapy intervention, standard control therapies varied between studies making comparison and data pooling difficult. For future research we recommend that ‘standard therapy’ is clearly described and based on a previously described intervention or control therapy.
Lastly, we noticed that the preferred outcome measure, RTP, varied greatly between studies, indicating that RTP criteria lack a universal definition. As it is a highly relevant clinical outcome, we feel authors should report predefined specified criteria (eg, no residual symptoms on physical examination and the unrestricted completion of sport-specific exercises), which need to be met before RTP clearance. Re-injuries should always be reported as this reflects on interventions long-term success and possible pre-mature RTP.1
Conclusion
Of 10 included studies, only two good or excellent quality RCTs with low risk of bias were identified. For enhanced time to RTP, meta-analysis showed superior efficacy for adding lengthening exercises, but not for PRP injections. For reducing re-injury rate, there is limited evidence to include agility and trunk stabilisation exercises. The identified limitations of most RCTs should guide the design of new hamstring RCTs.
For daily practice, adding lengthening exercises and PATS should be considered to reduce the RTP duration and re-injury risk following acute hamstring injuries.
What are the new findings?
Meta-analysis of lengthening and loading rehabilitative exercises in acute hamstring injuries show a positive effect on return to play.
Meta-analysis of platelet-rich plasma injections in acute hamstring injuries shows no effect.
Progressive agility and trunk stabilisation may reduce re-injury rates.
Acknowledgments
The authors would like to thank Andreas Serner from the Aspetar orthopaedics and sports medicine hospital, Doha, Qatar, for his work as our independent assessor. They also thank Carl Askling from the Swedish School of Sport and Health Sciences, Karolinska Institutet, Stockholm, Sweden, for supplying us with additional data to complete our meta-analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Competing interests GR, MHM, JLT and AW report grants outside the submitted work from Arthrex Medizinische Instrumente GmbH and the Royal Netherlands Soccer Association as part of the Dutch HIT study group for conducting a study on PRP in hamstring injuries: the Dutch HIT-study (Reurink et. al, NEJM 2014). In all cases, no personal payments were received.
Provenance and peer review Not commissioned; externally peer reviewed.