Article Text

Abstract
Background Physical examination tests for hip dysfunction and injury of the strongest diagnostic accuracy were identified in a recent systematic review with meta-analysis in BJSM. These tests are described in this article.
Discussion A detailed description of the various different tests is given, with photographs for each test procedure. Diagnostic interpretation of each test requires careful consideration, with special attention to specific variables such as test performance and patient population.
Statistics from Altmetric.com
Introduction
Diagnosis of non-arthritic hip pathology is challenging. In the last 10 years the understanding of hip pathology and femoroacetabular impingement (FAI) has exploded,1 although in the spectrum of medicine knowledge this area is relatively new.2 As such, expertise is often located in irregular pockets of providers, resulting in variable understanding and recognition in the larger medical community. Patients with intra-articular hip pathology have been reported to see 3.3 providers on average before being correctly diagnosed.3 ,4 Thus, it is not uncommon for a patient to undergo inappropriate imaging and, unfortunately, inappropriate treatments including epidural steroid injections, hernia repairs and even lumbar spine fusion. Furthermore, long-standing hip pain results in surrounding dysfunction of the low back, pelvis and even knee, with poorer outcomes in patients with concomitant conditions.5 These factors converge to make diagnosis of hip pathology one of the greatest challenges currently facing the orthopaedic and sports medicine field.
Disorders of the hip can largely be categorised as intra-articular or extra-articular. Intra-articular disorders are driven by pathology at opposite ends of the morphological spectrum; acetabular dysplasia or FAI.3 ,6 Labral tears are recognised to be the pain generator in these disease states. Extra-articular disorders include psoas tendon disorders such as internal snapping hip and tendinitis, peritrochanteric space disorders such as external snapping hip and abductor tendon tears, and deep gluteal space syndrome, previously known as piriformis syndrome.7
Whereas imaging is clearly important for correct diagnosis, false positives with MRI and MRI with arthrogram (MRA) are common, requiring providers to determine whether a distinct pathology is actually symptomatic, further relying on accurate and efficient physical examination. Solving this problem requires two primary approaches: (1) identify the most accurate-specific hip physical examination (HPE) tests and (2) provide detailed descriptions and instructions to providers to allow reproduction and application of these tests. The first was recently addressed by Reiman et al8 in a systematic review and meta-analysis. This article encompassed a detailed execution of the HPE tests with the greatest clinical utility as outlined by that group. In addition, the publication discussed the discrepancy in test description and reason for caution in test interpretation when appropriate.
Physical examination tests of the hip
Hip osteoarthritis
Trendelenburg's sign9
Patient position: Standing in front of the examiner, with both feet on ground.
Clinician position: Observing the patient from the front.
Movement: The patient is instructed to lift one leg up by flexing their hip and knee, standing on only one leg (figure 1A).
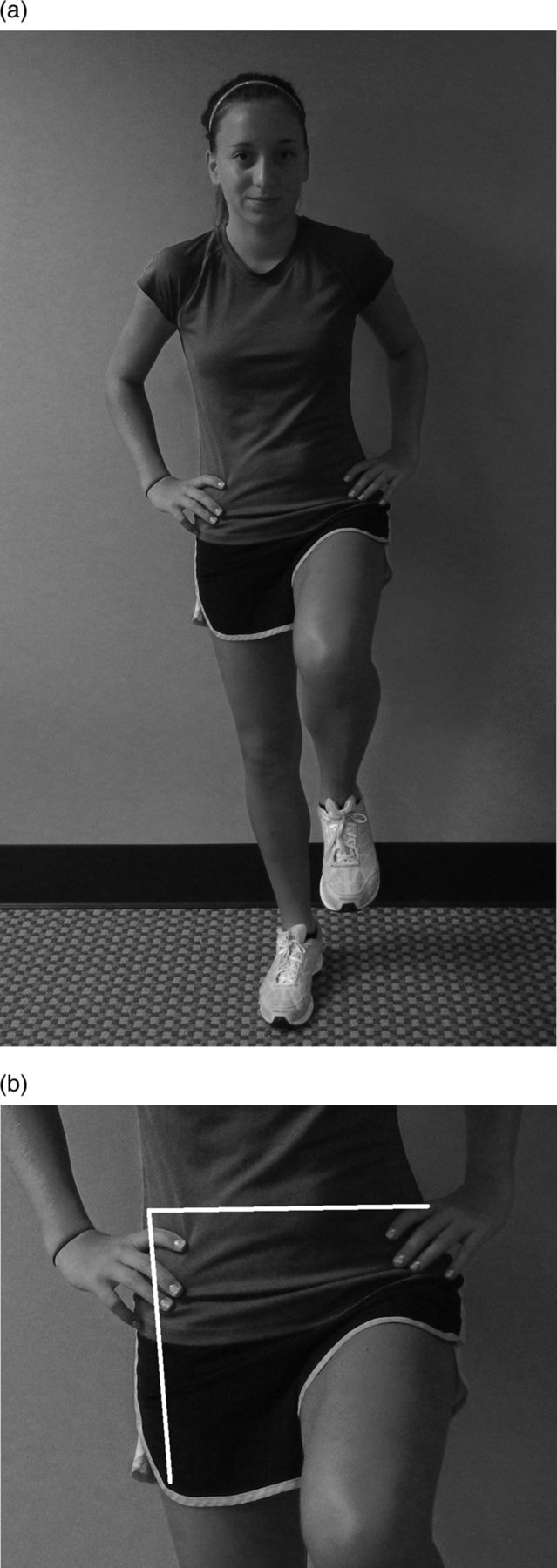
(A) Trendelenburg's sign. (B) Angle of measurement for Trendelenburg's sign.
Assessment: The clinician assesses the weight-bearing leg by evaluating the degree of drop of the contralateral pelvis once the leg is lifted. A pelvic on femoral angle with ≤83° angle criteria with specified time duration of 30 s was used as a positive sign. Figure 1B shows the pelvic on femoral angle (angle between the two lines).
Diagnostic accuracy: Sensitivity (SN) 55%, specificity (SP) 70%, positive likelihood ratio (+LR) 1.83 and negative likelihood ratio (−LR) 0.82.
Special note: Monitor for patient compensating by leaning their trunk to avoid having pelvis drop. Leaning compensation constitutes a positive test as well.
Background: Generally considered a physical performance test of hip strength, this test has also been utilised for assessment of gluteal tendinopathy with a positive test being reproduction of spontaneous pain within 30 s on involved leg compared with the contralateral leg during single leg stance.10
The use of a supporting stick was suggested in the hand only on the side of the weight-bearing hip. Alternatively, both shoulders could be supported by the examiner so as to maintain balance without a stick.11
Commentary on hip osteoarthritis tests
The Trendelenburg's sign alters post-test probability of a diagnosis to a very small degree.8 The clinician should carefully incorporate functional assessment (gait, stairs, etc) as part of the examination continuum even though they have not been specifically investigated for this cohort. In addition, consideration of additional components such as (1) more than one plane of motion restriction, (2) age >50 and (3) stiffness ≤60 min, are a necessity for clinical assessment of hip osteoarthritis.12 ,13
Gluteal tendinopathy
Resisted external derotation test
Patient position: Supine, hip flexed 90°, and in external rotation.10
Clinician position: Clinician, standing just to the side of leg being tested, slightly decreases external rotation just enough to relieve pain (if any was present).
Movement: Patient then actively returns the leg to neutral position (placing leg along the axis of the bed) against resistance (figure 2).

Resisted external derotation test.
If test result is negative, the test is repeated with patient lying prone, hip extended and knee flexed to 90°.
Assessment: A positive test is spontaneous reproduction of patient's concordant pain.
Diagnostic accuracy: SN 88%, SP 97.3%, +LR 32.6 and −LR 0.12.
Special note: Monitor for patient compensation of grabbing onto table for stabilisation during test.
Background: The combination of passive stretch, followed by active contraction is likely to provide the tensile load across the involved structure(s).
Commentary on gluteal tendinopathy tests
Only the resisted external derotation test demonstrated the ability to modify the post-test probability of a gluteal tendinopathy diagnosis.8 The sole study examining this test only had a sample size of 17 participants, with an average age of 68.1±10.8 years, thus limiting the external generalisability. The Trendelenburg's sign (as described above in the Hip osteoarthritis section) demonstrated a pooled SN of 61%, SP 92%, +LR 6.83 and −LR of 0.25;8 across three studies with 78 patients.10 ,14 ,15
Impingement/labral tear/intra-articular pathology
Impingement (flexion-adduction-internal rotation) (FADDIR) test
Patient position: Supine, bilateral legs extended.16–20
Clinician position: Standing at the side of the leg to be tested.
Movement: Clinician passively moves the patient's leg to 90° of hip and knee flexion. The leg is then passively adducted and internally rotated with overpressure to both motions at end-range (figure 3).

Flexion-adduction-internal rotation test.
Assessment: A positive test is reproduction of concordant pain, locking, clicking and catching.
Pooled diagnostic accuracy:
-
(MRA criterion reference) SN 94%, SP 8%, +LR 1.02, −LR 0.48;8 across four studies with 128 patients.16 ,17 ,19 ,20
-
(Arthroscopy criterion reference) SN 99%, SP 7%, +LR 1.06, −LR 0.15;8 across two studies with 157 patients.18 ,19
Special note: Monitor for patient compensation of rolling trunk toward non-involved leg to avoid pain. Discordant lateral hip pain is a negative test.
Background: The combination motions of flexion, adduction and internal rotation cause an abutment between the femoral head and anterior acetabulum.
Flexion-internal rotation test
Patient position: Supine, bilateral legs extended.21–23
Clinician position: Standing at the side of the leg to be tested.
Movement: Clinician passively performs the combined movements of flexion to 90° and internal rotation (figure 4).

Flexion-internal rotation test.
Assessment: A positive test is reproduction of concordant pain, locking, clicking or catching.
Pooled diagnostic accuracy: SN 96%, SP 17%, +LR 1.12, −LR 0.27;8 across three studies with 42 patients.21–23
Special note: Monitor for patient compensation of rolling trunk toward non-involved leg to avoid pain.
Background: This test produces a likely similar abutment described for the FADDIR test without the end-range adduction. In addition, moving from neutral adduction to end-range internal rotation could impinge an anterior labral tear.
Thomas test
Patient position: Sitting at the end of the table, feet on floor.24
Clinician position: Standing at end of table, directly facing patient.
Movement: Clinician passively lays the patient onto their back, bringing bilateral knees up to patient's chest. Patient holds non-tested leg toward their chest with bilateral arms as the clinician passively lowers the tested leg into extension. The clinician stabilises the ipsilateral side of the pelvis with their other arm (figure 5).

Thomas test.
Assessment: A positive test is reproduction of painful click or concordant groin pain.
Diagnostic accuracy: SN 89%, SP 92%, +LR 11.1 and −LR 0.12.24
Special note: Monitor for tightness/compensation of the lumbar spine arching, tested leg abducting and externally rotating.
Background: Although this test does not reproduce the mechanical abutment between the femoral head and acetabulum similar to the FADDIR or flexion internal rotation test, it does recreate hip extension, which has been shown to recreate the greatest forces on the hip joint.25
Commentary on impingement/labral tear/intra-articular pathology tests
In general, these tests demonstrate better screening than diagnostic ability.8 The one study with the least risk of bias demonstrated that the Thomas test has value as both a screen and diagnostic test.24 Caution should be used though as this was only one study.24
Femoral fracture/stress fracture
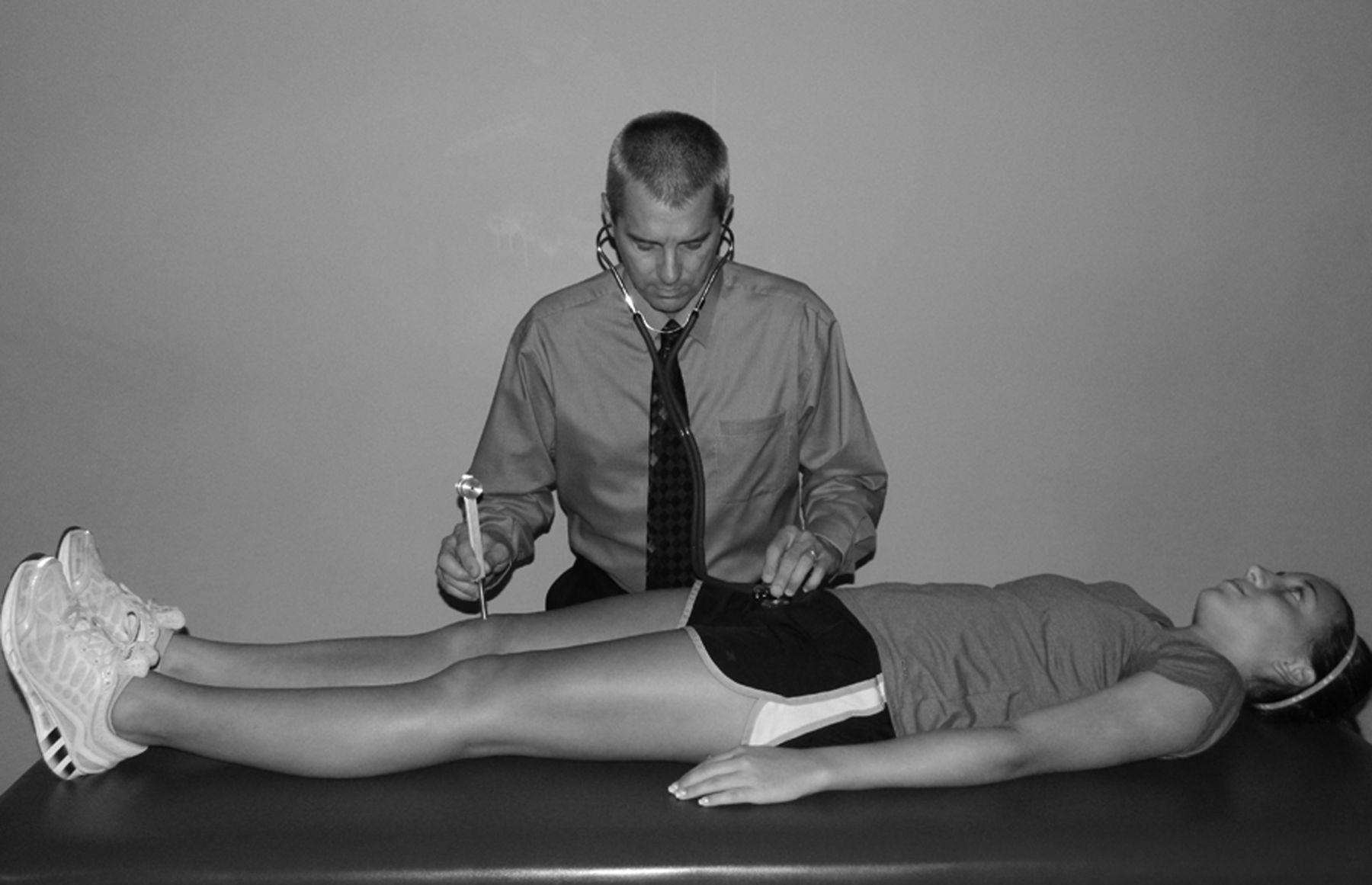
Patellar-pubic percussion test
Patient position: Supine, bilateral legs extended.26–28
Clinician position: Standing at the side of the leg to be tested.
Movement: Clinician places a stethoscope over the pubic tubercle of the patient. Clinician taps the patella of patient's leg being assessed and qualitatively reports the sound. A tuning fork has also been used in place of tapping (figure 6).

Patellar-pubic percussion test.
Assessment: A positive test is diminished percussion noted compared with contralateral side.
Pooled diagnostic accuracy: SN 95%, SP 86%, +LR 6.11, −LR 0.07;8 across three studies with 782 patients.26–28
Special note: Clinician must ensure that stethoscope is placed firmly over pubic tubercle and lateral to the pubic symphysis joint (on the side ipsilateral to side being tested).
Background: The sound produced with either tapping or the tuning fork is dampened with the fracture/stress fracture.
Fulcrum test
Patient position: Sitting on side of table with bilateral distal portion of legs off the edge of the table.29 ,30 Patient is instructed to lean back on bilateral hands.
Clinician position: Standing or kneeling to the side of the leg to be tested.
Movement: Clinician places one forearm under patient's thigh to be tested. Clinician arm is used as a fulcrum under the thigh and is moved from the distal to the proximal thigh as gentle pressure is applied to the dorsum of the knee with the opposite arm (figure 7).

Fulcrum test.
Assessment: A positive test is reproduction of patient's concordant discomfort/sharp pain, usually accompanied by apprehension.
Diagnostic accuracy: SN 93%, SP 75%, +LR 3.7, −LR 0.09;29 SN 88%, SP 13%, +LR 1.0, −LR 0.92.30
Special note: The length of the femur assessed is limited due to the ability to place the arm under the assessed femur.
Background: Fulcrum and pressure applied in the direction opposite creates stress force to the area of suspected stress fracture.
Commentary on fracture/stress fracture tests
The patellar-pubic percussion test has strong diagnostic value as both a screen and diagnostic test.8 The use of stethoscope and tuning fork has previously been demonstrated as a valid measure for this diagnosis.31 Caution is suggested with the use of the stress fracture test (despite demonstrated ability to function as a screening test) due to high risk bias and small subject sizes in studies investigating this test.
Sports related chronic groin pain
Single adductor test
Patient position: Patient is supine with bilateral legs extended.32
Clinician position: Standing at patient's foot to be assessed.
Movement: Clinician passively flexes leg to be assessed to 30° with slight abduction and internal rotation. Patient resists the clinicians attempt to abduct the leg to be tested, effectively contracting their adductor muscles on that side (figure 8).

Single adductor test.
Assessment: A positive test involves reproduction of patient's concordant pain.
Diagnostic accuracy: SN 30%, SP 91%, +LR 3.3 and −LR 0.66.32
Special note: Force is applied at the ankle with the knee straight.
Background: As with the other sports related chronic groin tests, adduction contraction elicits stress across the common origin of the adductor muscles on the pubic symphysis region.
Squeeze test
Patient position: Supine with bilateral hips flexed 45° and knees flexed 90° so that bilateral feet are flat on table.32
Clinician position: Standing at patient's bilateral knees, placing fist between knees.
Movement: Patient is asked to contract maximally both adductor muscles simultaneously to ‘squeeze the fist’ effectively (figure 9).

Squeeze test.
Assessment: Reproduction of patient's concordant pain is considered a positive test.
Diagnostic accuracy: SN 43%, SP 91%, +LR 4.8 and −LR 0.63.32
Special note: Monitor for patient compensation of lower trunk rotation.
Background: As with the other sports-related chronic groin tests, adduction contraction elicits stress across the common origin of the adductor muscles on the pubic symphysis region.
Bilateral adductor test
Patient position: Patient is supine with bilateral legs extended.32
Clinician position: Standing at patient's bilateral feet, directly facing patient.
Movement: Patient is asked to contract maximally both adductor muscles simultaneously, thereby attempting to bring bilateral legs together (figure 10).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bilateral adductor test.
Assessment: Reproduction of patient's concordant pain is considered a positive test.
Diagnostic accuracy: SN 54%, SP 93%, +LR 7.7 and −LR 0.49.32
Special note: Monitor for compensations of patient grabbing onto table and/or bending knees.
Background: As with the other sports related chronic groin tests, adduction contraction elicits stress across the common origin of the adductor muscles on the pubic symphysis region.
Commentary on sports related chronic groin pain tests
The bilateral adductor test was the most diagnostic of these tests, with the potential to alter post-test probability to a moderate degree.8 The other two tests, single adductor test and the squeeze test, also have greater capability as a diagnostic versus screening test. Both of these tests can alter posttest probability to a small degree.
Discussion
Clinical testing of the hip is not nearly as comprehensively investigated as other body part regions such as the shoulder and the knee. As such the collection of clinical tests available to diagnostic clinicians is somewhat underwhelming in context. This may be one of the reasons patients with hip problems frequently undergo inappropriate imaging and inappropriate treatments, and have a delayed proper diagnosis.3 ,4
This manuscript focuses on the detailed execution of 10 index tests for the hip joint. Each is described in sufficient detail using the sentinel reference when available. The tests were selected from the recent systematic review and meta-analysis from Reiman et al,8 because to our knowledge, this study is the most comprehensive investigation of the diagnostic accuracy of the hip joint.
And added benefit of a description paper is that the execution of the tests can be standardised across future studies. When possible, we used the sentinel references for the description of each index test. Variation in test performance is a form of bias that has been recognised in the original QUADAS33 and QUADAS II34 quality assessment instruments. Consistent use of these tests in future well designed studies should more efficiently determine the true value of these tests during examination of the hip joint.
What is already known on this topic
-
Hip joint examination is becoming increasingly popular with improving technology regarding examination and treatment.
-
Multiple studies have been describing various hip physical examination (HPE) tests. Currently, reviews have only focused on labral pathology. Reiman et al8 in the British Journal of Sports Medicine is the only systematic review to examine the clinical utility of HPE tests for all hip pathology.
-
Description of the various HPE tests is quite variable dependent on the study.
What this study adds
-
This study describes the correct performance of the best HPE tests as described by Reiman et al8 The variable description in multiple studies for similar tests requires a detailed description (and photograph) of the test procedure for each relevant hip pathology.
Acknowledgments
The authors would like to thank Carly Reiman for participating in the photographs.
References
Footnotes
-
Contributors MPR provided idea, design, writing, review of manuscript and overall content of material; Mather and Cook provided writing, review and overall content of manuscript.
-
Competing interests None.
Provenance and peer review