Article Text

Abstract
Objectives To conduct a systematic review and meta-analysis investigating effects of exercise for people with alcohol use disorders (AUDs) across multiple health outcomes. We also investigated the prevalence and predictors of dropout from exercise studies in AUDs.
Design Systematic review and random effects meta-analysis with meta-regression analyses.
Data sources 3 major electronic databases were searched from inception until April 2016 for exercise intervention studies in adults with AUDs.
Eligibility criteria Studies of acute exercise in people with AUDs; and randomised and non-randomised trials examining effects of long-term (≥2 weeks) exercise.
Results 21 studies and 1204 unique persons with AUDs (mean age 37.8 years, mean illness duration 4.4 years) were included. Exercise did not reduce daily alcohol consumption (standardised mean difference (SMD) =−0.886, p=0.24), or the Alcohol Use Disorders Identification Test (AUDIT) total scores (SMD=−0.378, p=0.18). For weekly consumption (n=3 studies), a statistically significant difference was observed favouring exercise (SMD=−0.656, p=0.04), but not after adjustment for publication bias (SMD=−0.16, 95% CI −0.88 to 0.55). Exercise significantly reduced depressive symptoms versus control (randomised controlled trials (RCTs) =4; SMD=−0.867, p=0.006, I2=63%) and improved physical fitness (VO2) (RCTs=3; SMD=0.564, p=0.01, I2=46%). The pooled dropout rate was 40.3% (95% CI 23.3% to 60.1%) which was no different to control conditions (OR=0.73, p=0.52). Dropouts were higher among men (β=0.0622, p<0.0001, R2=0.82).
Limitations It was not possible to investigate moderating effects of smoking.
Conclusions Available evidence indicates exercise appears not to reduce alcohol consumption, but has significant improvements in other health outcomes, including depression and physical fitness. Additional long-term controlled studies of exercise for AUDs are required.
- Exercise
- Physical activity
- Depression
- Anxiety
- Fitness
Statistics from Altmetric.com
Introduction
Alcohol use disorders (AUDs) are among the most common of all psychiatric disorders with an estimated global lifetime prevalence of around 16%.1 The societal consequences of hazardous drinking are substantial and include accidents, violence and antisocial behaviours.2 Long-term health consequences can include brain damage, liver cirrhosis and metabolic diseases.2 The estimated annual cost of excessive alcohol consumption in the USA is around US$223 billion.3
While the personal and social impact of AUDs can be immense, only a limited number of those affected receive appropriate treatment.4 ,5 A survey in the UK found that only 1 out of 18 people who met the criteria for alcohol dependence had received formal treatment.6 One potential explanation for poor help-seeking is the perceived stigma associated with traditional treatments for AUDs, which are often administered in specialist clinics.7 ,8 Current treatment options include pharmacological therapy, cognitive–behavioural interventions (CBT), motivational interviewing and 12-step facilitation treatment (ie, a model of alcohol recovery based on group therapy and support).9 Despite advancements in these treatment modalities, relapse remains high and pharmacotherapy has unwanted side effects. Among treated individuals, first year remission rates can vary between 60% and 90%, depending on the severity of the disorder and the criteria for remission.10 ,11 While effective treatment options are available, there is a need for novel adjunctive interventions that may help in alcohol abstinence and the comorbid health problems commonly associated with the disorder, which include depression/anxiety12 ,13 and cardiometabolic risks.14
Exercise is a potentially efficacious alternative treatment for AUDs that is feasible and appeals to a broad spectrum of patients.15 ,16 Meta-analytic reviews have supported the antidepressant effects of exercise among otherwise healthy adults,17 chronically ill patients18 and patients with depressive disorders.19 Evidence supporting the use of exercise in the treatment of substance use disorders is growing.20 In the field of smoking cessation, where most research exists to date, a review of 17 randomised controlled trials (RCTs) exploring the effects of long-term exercise interventions found that exercise generally improved one or more smoking-related outcomes, and abstinence rates were comparable to CBT and/or nicotine replacement therapy.21
Evidence supporting exercise interventions for AUDs has expanded in recent years. Two recent narrative reviews of the literature have summarised the current evidence from studies of exercise for AUDs. A systematic review by Giesen et al22 including 14 RCTs indicated that exercise may have beneficial effects on certain domains of physical functioning, including fitness, basal heart rate, physical activity level and strength. Inconsistent effects with a trend towards a positive effect were observed for anxiety, mood management, alcohol craving and drinking behaviour.22 Exercise interventions in AUDs were considered safe, with no adverse events reported. Manthou et al23 examined studies reporting the use of exercise to treat AUDs published between 1970 and 2015, including the underlying mechanisms. In total, 11 studies were identified, of which six concluded that exercise may have a positive impact on consumption, abstinence rates or the urge to drink.23 While these narrative reviews have clearly advanced the field, to the best of our knowledge, no meta-analysis exists which has pooled data to consider the benefits across the multiple trials and health outcomes.
Another important yet understudied issue concerns dropouts from long-term exercise interventions for AUDs. Available evidence suggests variability in participant dropouts, yet no studies have pooled data to systematically examine dropout rates. Poor treatment adherence is of major concern to policymakers as it is associated with higher risk of relapse, and thus greater resource usage.24 From a research perspective, participants who fail to complete study protocols can affect statistical analyses, research outcomes and interpretation of results. For example, the current research evidence for physical activity interventions in AUDs is mainly based on data from participants completing the interventions. This may skew results, favouring those who fully engage with exercise treatments. Understanding the prevalence and predictors of dropouts in exercise interventions is an important research question. Moreover, an empirically derived estimate of typical frequency of dropout and an exploration of its moderators could inform the design of new studies, in addition to informing clinical practice and policy.
Given the aforementioned, we conducted a systematic review and meta-analysis investigating the benefits of exercise for people with AUDs across multiple health outcomes. The primary outcome of interest was the change in alcohol consumption. A secondary aim was to report the pooled treatment effects of exercise on secondary health-related outcomes including fitness (maximum oxygen uptake, VO2max), depression, anxiety and self-efficacy. Finally, we also sought to clarify the prevalence and predictors of dropout from exercise studies in people with AUDs.
Method
This systematic review was conducted in accordance with the Meta-Analyses and Systematic Reviews of Observational Studies (MOOSE) guidelines25 and in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard.26
Inclusion and exclusion criteria
Included were: (1) studies of acute exercise (a single bout) in people with AUDs; and (2) studies of randomised and non-randomised trials examining the effects of long-term (≥2 weeks) exercise interventions in people with AUDs. We included studies where AUDs were diagnosed using established criteria from the following sources: the Diagnostic and Statistical Manual of Mental Disorders (DSM-I),27 DSM-II,28 DSM-III-R,29 DSM-IV,30 DSM 5,31 the International Classification of Disease (ICD-10),32 the Alcohol Use Disorders Identification Test (AUDIT),33 and guidelines from the National Institute on Alcohol Abuse and Alcoholism (NIAAA).34 All included studies involved ‘exercise’ as the primary intervention, that is, planned, repetitive movement, purposefully engaged in to improve fitness and/or health.35 We excluded cross-sectional and prospective observational studies reporting associations between exercise and AUDs. There were no language restrictions. When required, we contacted the primary or corresponding authors of studies up to two times in a 1-month period to (1) confirm eligibility and (2) obtain the data required for analysis if they were not available in the published paper.
Search strategy, inclusion criteria and critical appraisal
Two independent authors (MH and BS) searched Medline, PsycARTICLES and Embase from database inception to 11 April 2016 without language restrictions. Terms were searched by entering the following key words into the databases: ‘alcoholism’ or ‘alcohol related’ or ‘alcohol dependence’ or ‘alcohol use disorder’ or ‘hazardous drinking’ or ‘harmful drinking’ and ‘exercise’ or ‘physical activity’ or ‘sport’ or ‘aerobic training’ or ‘endurance training’ or ‘resistance training’ and ‘trial’ or ‘randomised controlled trial’ or ‘controlled trial’. Manual searches were also conducted using the reference lists from recovered articles. After the removal of duplicates, two reviewers (MH and BS) independently screened the titles and abstracts of all potentially eligible articles. Both authors applied the eligibility criteria, and a list of full-text articles was developed through consensus. The two reviewers then independently considered the full texts of these articles and the final list of included articles was reached through consensus. A third reviewer (DV) was available for mediation throughout this process. Methodological appraisal was performed according to PRISMA standards,26 including evaluation of bias (confounding, overlapping data, publication bias).
Data extraction
Two authors (MH and ESG) independently reviewed and extracted relevant data using a data extraction form which included the following fields: primary diagnosis, sample size, intervention type, duration and quality (randomisation, blinding, intention-to-treat (ITT), selective reporting), number of sessions offered and completed, level of supervision, participant age, gender, smoking status, body mass index and dropout rate. Alcohol consumption was recorded based on the number of standard drinks consumed per day, per week, the number of heavy drinking days, the AUDIT score and alcohol urges/cravings. Other relevant health outcomes extracted were: physical activity levels, fitness (VO2, heart rate, 3-minute step test, heart rate index, functional aerobic index, walking test), depression, anxiety, self-efficacy, quality of life (QoL) and cortisol levels (if reported).
Risk of bias
One author (MH) assessed studies on the presence of high risk, low risk or unclear risk of bias by considering the following four factors: study design (randomised allocation to treatment vs control group), outcome assessor blinding, ITT analysis and selective reporting of results. Each item was scored as either present, absent or unclear. To be considered a low risk of bias, studies needed to score positively on all four assessment criteria, except selective reporting which was scored in the reverse. The criteria used for risk of bias assessment were based on the Cochrane Handbook36 and Cochrane reviews of exercise for depression.37 ,38
Meta-analysis
Owing to the anticipated heterogeneity across studies, we conducted a random effects meta-analysis with Comprehensive Meta-Analysis software (CMA, V.3). The meta-analysis was conducted in the following sequence. First, for continuous outcome data, we calculated the standardised mean difference (SMD) together with 95% CIs comparing continuous outcome data in exercise participants versus control conditions. We anticipated conducting separate analyses for acute and long-term exercise studies. Second, we calculated the prevalence of dropout from long-term exercise studies together with 95% CI. Where possible, subgroup analyses were performed to identify characteristics which might influence dropout rates. We then did a comparative meta-analysis calculating the OR and 95% CI to establish if dropout rates differ among exercise or control conditions. Third, we conducted meta-regression analyses where possible, when there were four or more studies providing data on each outcome variable. The potential moderators of interest were chosen on the basis of previous work,39 ,40 and included participant characteristics (mean age, % male, illness duration, body mass index) and exercise characteristics (session and intervention length). For all outcomes and meta-analyses, it was our intention to separately pool data from acute and long-term exercise studies. Heterogeneity was assessed with the I2 statistics for each analysis.41 Publication bias was assessed using the Egger's regression method.42 We also adjusted for any potential publication bias with a trim and fill adjusted analysis43 to remove the most extreme small studies from the positive side of the funnel plot, and recalculated the effect size at each iteration, until the funnel plot was symmetric about the (new) effect size. Missing data (SDs) were replaced based on data imputation methods recommended by Cochrane.36
Best evidence synthesis
Using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach,36 we reviewed all relevant papers to determine a summary recommendation for each outcome, taking into account the overall quality of available evidence. This entailed consideration of within-study risk of bias (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias. Based on assessment of these criteria, the GRADE approach specifies four levels of evidence quality: high, moderate, low and very low.
Results
The initial literature search yielded 2938 potential articles, and 2458 after the removal of duplicates. Following removal of papers based on the title and abstract information, we screened 23 full texts and 21 were included in the final sample. Full details of the search results including reasons for exclusion are detailed in figure 1.

PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Included studies, participant and intervention characteristics
The final sample comprised 21 studies and 1202 unique persons with AUDs. A summary of the included studies is provided in online supplementary table S1. Briefly, sample sizes ranged from 2016 ,44 to 46845 participants with a median sample size of 34. Mean age (N=13 studies) was 37.8 years (range=18–70 years), and illness duration (where stated, N=10 studies) ranged from 4.415 to 18 years.46 Participant gender was reported in 13 studies; five involving male participants only,46–50 while another eight studies included men and women. Seventeen studies examined the effects of long-term exercise, ranging in duration from 248 ,51 to 52 weeks,15 and four studies involved acute bouts of exercise.44 ,52–54 The mean exercise session duration was 43 min (SD=19 min). Thirteen studies used aerobic exercise as the intervention, five studies used a combination of aerobic exercise, strength training and/or calisthenics15 ,55–58 and three studies used yoga/stretching.16 ,51 ,58 Most of the included studies (N=17) were supervised, either by a physical therapist or qualified exercise trainer; however, three studies involved a mixture of supervised and unsupervised exercise.16 ,55 ,59 Seventeen studies included an ‘active’ control intervention; for the long-term studies, this generally consisted of CBT, group counselling and/or pharmacotherapy. One study compared exercise with a non-treated control group,58 and three studies did not report details of the control condition. In total, 12 studies involved participants from inpatient/hospital settings, 3 studies included outpatients and 2 studies included student populations. All 21 studies included in the review were rated as either high or unclear risk of bias, based on the four assessment criteria described previously. Complete details of the scoring outcomes are available on request from the corresponding author.
supplementary table
Summary of included studies: exercise interventions in alcohol use disorders
Meta-analysis of exercise versus control conditions
Alcohol consumption
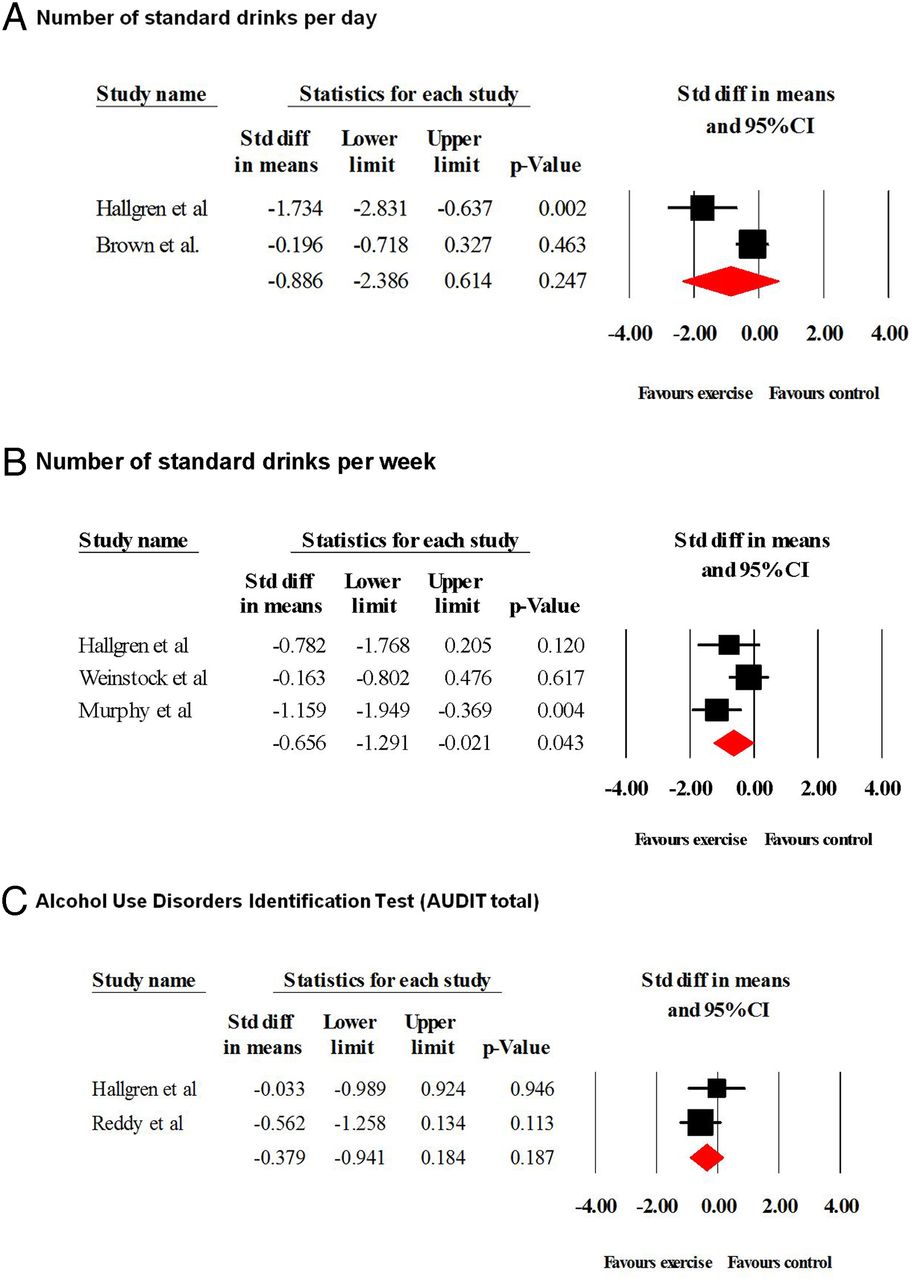
Full details of the meta-analyses results are summarised in table 1, including heterogeneity and publication bias data for each analysis. Figure 2 illustrates the pooled analyses in a forest plot. Briefly, there was no evidence to suggest that exercise reduced self-reported average daily alcohol consumption (SMD=−0.886, p=0.24), or the AUDIT total scores (SMD=−0.378, p=0.18). These analyses were limited to only two RCTs each. For the change in average weekly consumption (n=3 studies), a statistically significant difference was observed favouring exercise (SMD=−0.656, p=0.04), but the difference was no longer significant after adjustment for publication bias (SMD=−0.16, 95% CI −0.88 to 0.55).
Meta-analysis of effects of exercise on outcomes in AUD in long-term studies
{kind=link}
{kind=link}
Effect of exercise on alcohol consumption. (A) Number of standard drinks per day. (B) Number of standard drinks per week. (C) Alcohol Use Disorders Identification Test (AUDIT total).
Other health outcomes
Data from four RCTs15 ,16 ,51 ,60 including 133 people found that exercise significantly reduced depressive symptoms versus control conditions (SMD=−0.867, 95% CI −1.49 to −0.24, p=0.006, I2=63%). While the Egger test did not indicate any publication bias (p=0.23), the Duval and Tweedie trim and fill indicated a potential missing study and the adjusted effect size was slightly increased (SMD=−1.02). Data from 179 people (N studies =3) demonstrated that exercise significantly improved VO2max versus control conditions (SMD=0.564, 95% CI 0.11 to 1.01, p=0.01, I2=46%) with no evidence of publication bias. There was no evidence that exercise improved heart rate, anxiety or self-efficacy (see table 1). Smoking status was indicated in three studies,15 ,44 ,54 but associations between smoking and study outcomes were not reported. Forest plots for the secondary study outcomes are available as online supplementary material.
supplementary data
Dropout from exercise interventions
In total, 10 long-term studies provided data on dropout from exercise interventions. The pooled dropout rate among the 1204 participants was 40.3% (95% CI 23.3% to 60.1%). The Egger test indicated no publication bias (intercept =1.68, p=0.44) and the proportion of dropout remained unchanged after conducting the Duval and Tweedie trim and fill adjusted analysis for missing studies. There were no significant differences in dropout rates according to type of exercise or number of sessions per week. Details of the meta-analysis of dropouts are presented in table 2. The dropout rate in control conditions was 33.6% (95% CI 22.2% to 47.3%). There was no significant difference in dropout from 10 studies between exercise and control conditions (OR 0.73, 95% 0.28 to 1.89, p=0.52).
Meta-analysis and meta-regression of dropouts in long-term exercise studies
Predictors of dropout from exercise in AUDs
Full details of the meta regression analyses including the standardised β, 95% CI and R2 values are summarised in table 2. Only a higher proportion of male participants in the study samples moderated a larger dropout from exercise (β=0.0622, 95% CI 0.0335 to 0.0908, p<0.0001) and explained a large portion of the between-study heterogeneity (R2=0.82). No other moderators influenced the dropout rates.
Adverse events
No adverse events were reported in any of the studies included in this review.
Best evidence synthesis
For the primary study outcome (alcohol consumption) we determined that the current level of evidence supporting exercise interventions for AUDs is ‘low’. The five studies reporting usable alcohol consumption data were randomised trials;16 ,50 ,55 ,58 ,59 however, none of the included studies reported the use of blinded assessments. Moreover, the analyses were limited to only three studies—one with a small number of participants16—resulting in imprecise estimates of treatment effect. We noted that the direction of change favoured exercise interventions (ie, lower consumption in the exercise condition compared with control group at follow-up). For secondary outcomes, four studies reported the effects of exercise on depressive symptoms15 ,16 ,51 ,60 and all studies favoured the exercise intervention with more precise estimates of treatment effect. We rated the level of evidence for this outcome as ‘moderate’. In total, five studies examined the effects of exercise on physical fitness, measured using either VO2 submaximal tests,55 ,59 ,61 or the change in resting heart rate following training.46 ,60 The evidence supporting exercise effects on fitness for these two related outcomes is ‘moderate’ and ‘very low’, respectively. The latter rating reflects the small number of trials (n=2) and outcome heterogeneity. Six studies examined exercise effects on anxiety16 ,47 ,60 and self-efficacy.47 ,48 ,60 Appraisal of these trials resulted in ratings of ‘moderate’ and ‘very low’ levels of evidence, respectively. Finally, on the basis of 10 separate trials, we rated the quality of evidence for the reported dropout rate as ‘high’. A narrative summary of studies reporting alcohol consumption outcomes is available in the journal's online supplementary material.
Discussion
To the best of our knowledge, this is the first study to examine the pooled treatment effects of exercise interventions for AUDs across multiple health outcomes. The results indicate that exercise was associated with significant reductions in depressive symptoms and improved physical fitness. However, after adjustment for publication bias, there were no statistically significant changes in alcohol consumption (the primary outcome), anxiety or self-efficacy. Data from 10 long-term trials indicated a pooled dropout rate of 40.3%, and male gender moderated this outcome. The dropout rate was no different in the exercise versus control conditions. Given that our comprehensive review found no reports of adverse events, a finding reported in previous reviews,15 ,23 it seems evident that exercise is safe and acceptable for people with AUDs.
The current findings are broadly consistent with recent narrative reviews of exercise for AUDs, based on 1154 and 14 studies,15 respectively. Giesen et al15 reported that exercise is a feasible and safe intervention for people with AUDs, which may have beneficial effects on physical functioning, including VO2max. In the present study, improvements in physical fitness were observed for exercise compared with control group participants. This finding has clinical relevance as AUDs are associated with a higher prevalence of metabolic disorders14 and with an increased risk of cardiovascular disease;62 effects that are understood to be mediated by physical fitness. Thus, the prescription of long-term exercise interventions in this population could result in measurable physical fitness benefits, lower cardiometabolic risks, and ultimately a reduced risk of premature mortality.
While adverse health outcomes are rare in studies of exercise for AUDs, heavy drinking is associated with numerous health risks. In addition to an increased risk of cardiovascular disease, stroke and some forms of cancer,63 regular heavy alcohol consumption can cause nerve damage (alcoholic neuropathy), which can produce pain, numbness and muscle weakness in the extremities;64 effects that could limit the type and/or intensity of exercise performed. In some instances, heavy drinking can also cause the number of red blood cells to be abnormally low, triggering symptoms such as fatigue, shortness of breath and light-headedness.63 While most individuals with an AUD do not experience these symptoms, alcohol's negative health effects underscore the importance of a thorough pre-exercise medical assessment, and the prescription of individually tailored exercise programmes. Heavily dependent individuals undergoing withdrawal symptoms (eg, delirium tremens) may require a period of specialised inpatient care lasting days or weeks before starting a light exercise regime under close supervision.
A second finding concerns the improvement in depression seen among exercise participants. Mood disorders frequently coexist with problematic alcohol use and depression has been linked to the aetiology of AUDs.65 US data show that in major depression, the lifetime prevalence rate for any AUD is 40%, and 21% for alcohol dependence.66 ,67 It has been suggested that alcohol exposure may cause metabolic changes that also act to increase the risk of mood disorders. For example, McEachin et al68 found that exposure to ethanol led to reductions in the production of methylenetetrahydrofolate reductase (MTHFR), an enzyme related to folate metabolism. Reduced folate levels have, in turn, been linked to increased risks of major depression, suggesting a possible causal link between AUDs and major depression via reduced MTHFR production. Similarly, Sjöholm et al69 found that individuals with a particular genotype related to circadian rhythms were at greater risk of co-occurring alcohol and mood disorders. The authors suggested that alcohol use alters circadian rhythms and metabolic patterns in individuals with this particular genotype, leading to an increased risk of depression.69 Meta-analytic reviews have supported the antidepressant effects of exercise among otherwise healthy adults,17 chronically ill patients18 and patients with depressive disorders.19 The present study adds the observation that long-term exercise interventions can lead to significant reductions in depressive symptoms in those with AUDs.
Our review included studies exploring the effects of acute exercise in people with AUDs. Of the four studies identified,44 ,52–54 two included assessments of alcohol cravings.44 ,52 In both studies, the ‘urge’ to drink alcohol reduced following bouts of aerobic exercise lasting 10 and 30 min, respectively. In a recently published study, Brown et al70 reported that alcohol cravings diminished pre to post exercise across a 12-week intervention with repeated assessments of moderate intensity exercise lasting 20–40 min. Improvements in mood and reduced anxiety were also reported at each session. These findings are particularly relevant, as mood and the urge to drink have been identified as important predictors of alcohol relapse.71 While promising, findings from these preliminary studies should be interpreted with caution as they are limited by small samples sizes, and in one instance, no comparison group.70
While most physical activity interventions have been shown to improve the health of people with psychiatric disorders, including substance abuse,21 treatment dropout poses an important challenge to the effectiveness of exercise interventions. Moreover, pooled data on dropouts from exercise studies for AUDs have yet to be reported. Ten long-term studies included sufficient data to calculate dropout rates, indicating a pooled dropout of 40.3% across the studies, with low-to-moderate heterogeneity (range=6.3–44.4%). This result should be considered in the context of other exercise studies. A recent meta-analysis of dropouts from physical activity interventions in schizophrenia (N=19 studies, 594 participants) indicated a pooled dropout rate of 26.7%.72 Another meta-analysis exploring dropouts from exercise RCTs among people with depression (N=40 studies, 1720 participants) reported an adjusted dropout prevalence of 18.1%.40 Of relevance, both reviews found that supervision of exercise by a qualified trainer or physical therapist was associated with a significantly lower dropout rate. In the present study, dropout rates were notably higher than those reported in the above-mentioned reviews, indicating that strategies to minimise participant dropout should be carefully considered during the planning of these interventions, and that power calculations should be based on highly anticipated dropout rates. Male gender was the only factor found to moderate participant dropout. As the pooled data included a higher proportion of male than female participants (with five studies including male participants only), this could explain the relatively high dropout rate seen here compared with studies of exercise for depression, where the proportion of female participants is generally much higher.37 Participant age, illness duration, study duration (weeks) and length of exercise session (minutes) had no effect on the pooled dropout rate, which was also equivalent between intervention and control groups.
As noted, our findings also indicate that long-term exercise was not associated with reductions in alcohol consumption, measured by the number of standard drinks consumed per day, per week and by the AUDIT total score. Similarly, there were no improvements in anxiety or self-efficacy. Although the SMD in alcohol consumption was not statistically significant after adjustment for publication bias (exercise vs control), the direction of change favoured the exercise participants, with mean reductions in alcohol consumption seen on all three measures. A similar non-significant trend was observed for the change in anxiety and self-efficacy. A recent narrative review by Giesen et al22 reported ‘inconsistent effects with a slight trend towards a positive effect’ on drinking behaviour, while another narrative review by Manthou et al23 reported that exercise had a positive impact on alcohol consumption, abstinence rates or the urge to drink in six out of 11 studies reviewed. Taken together, the current evidence suggests that exercise is a feasible treatment option for individuals with AUDs, with likely benefits for depression and physical fitness. However, it remains unclear if exercise can reduce drinking behaviour among this group. One should note, that across the multiple alcohol outcomes measured, our analyses were limited to three RCTs, therefore, additional well-designed pragmatic exercise interventions are required before any firm conclusions can be made regarding the potential impact of exercise on drinking behaviour.
Several psychobiological mechanisms have been proposed to explain the positive effects of exercise on mental health and the links with AUDs.20 ,73 Exercise has well-established mood-enhancing effects which have been linked to the monoaminergic system, specifically 5-HT release and metabolism.74 These effects may inhibit the urge to drink alcohol,44 and better mood states are understood to reduce the risk of alcohol use and relapse in dependent individuals.75 Related to these effects, exercise has also been shown to mediate stress-reactivity,76 and acute stress frequently precipitates alcohol consumption and relapse.77 Convergent evidence from human and animal studies suggests that physical activity facilitates neuroplasticity of certain brain structures and as a result, cognitive functions.78 While ‘moderate’ alcohol consumption has been linked in some studies to improvements in cognition, primarily in older adults,79 heavy drinking can have profound negative effects on different aspects of cognition, including attention, memory and executive function.80 Such deficits are postulated to elevate the risk of hazardous drinking by increasing attentional biases towards alcohol (or the salience of alcohol-related cues).81 Recent studies have shown that acute bouts of exercise can reduce cigarette cravings and attenuate smoking-related attentional biases;82 ,83 processes that could also apply to alcohol consumption. In addition to these interrelated neuro-biological mechanisms, a recent review suggests that exercise may also act on other, more distal factors that have a positive influence on AUD outcomes, including social environments.73
While this is the first meta-analysis of exercise interventions for AUDs, we acknowledge several limitations that are largely attributable to factors within the primary data. First, there was considerable methodological heterogeneity across the available studies (ie, sample size, dropout rate, intervention used and outcomes measured), with only five studies adequately reporting data on the primary outcome. Such heterogeneity makes comparison between studies difficult and limits the generalisability of the findings. Second, many studies failed to report relevant secondary health outcomes, such as QoL (one exception15), cognitive assessments, alcohol urges/cravings and effects of exercise on stress reactivity; factors that are related to the aetiology of AUDs, and possibly to alcohol recovery. These omissions limit the current evidence base and the strength of the conclusions that can be drawn from these data. Finally, future studies should seek to investigate the impact of smoking on outcomes and adherence to exercises in AUD.
Conclusion
In sum, our findings add new clinically relevant information about the beneficial effects of exercise interventions on physical fitness (SMD=0.564) and depression (SMD=−0.867) in people with AUDs, and quantify the relatively high dropout rate of 40.3% from these interventions. Another key message is that despite strong evidence supporting exercise in the treatment of myriad mental health disorders, there remains a paucity of studies exploring exercise effects on AUDs. In particular, little is known about the optimal exercise type and the ‘dose’ of exercise needed. Regular exercise may reduce the heightened cardiometabolic risks associated with AUDs, lower depression and improve mood states. To verify these results, additional adequately powered studies are required that include long-term follow-up assessments of multiple health outcomes.
What are the new findings?
This is the first review to assess the pooled treatment effects of exercise interventions for alcohol use disorders (AUDs) across multiple health outcomes.
Exercise was associated with significant reductions in depressive symptoms and improved physical fitness.
There were no statistically significant changes in alcohol consumption; however, the direction of change favoured exercise, and all analyses were limited to three studies.
The pooled dropout rate from exercise interventions in AUDs is 40.3% and is significantly higher among men.
How might it impact on clinical practice in the near future?
As people with AUDs have a double increased risk for cardiovascular disease and associated premature mortality, the findings suggest that supported exercise interventions should be integrated into the clinical management of those with AUDs.
Thorough medical assessment is recommended before exercise interventions are prescribed for people with severe alcohol dependency.
Additional methodologically robust studies are needed to determine the effects of exercise on alcohol consumption.
References
Footnotes
Contributors MH and BS wrote the first draft of the manuscript. BS performed the statistical analyses. DV, ESG and AL provided substantial input into all aspects of the manuscript.
Funding MH is supported by a grant from the Brain Foundation, Sweden (Hjärnfonden).
Disclaimer The funder had no role in the production of this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.