Article Text

Abstract
Objective To review and compare treatments (1) after primary traumatic shoulder dislocation aimed at minimising the risk of chronic shoulder instability and (2) for chronic post-traumatic shoulder instability.
Design Intervention systematic review with random effects network meta-analysis and direct comparison meta-analyses.
Data sources Electronic databases (Ovid MEDLINE, Cochrane Clinical Trials Register, Cochrane Database of Systematic Reviews, Embase, Scopus, CINAHL, Ovid MEDLINE Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE Daily, DARE, HTA, NHSEED, Web of Science) and reference lists were searched from inception to 15 January 2018.
Eligibility criteria for selecting studies Randomised trials comparing any interventions either after a first-time, traumatic shoulder dislocation or chronic post-traumatic shoulder instability, with a shoulder instability, function or quality of life outcome.
Results Twenty-two randomised controlled trials were included. There was moderate quality evidence suggesting that labrum repair reduced the risk of future shoulder dislocation (relative risk 0.15; 95% CI 0.03 to 0.8, p=0.026), and that with non-surgical management 47% of patients did not experience shoulder redislocation. Very low to low-quality evidence suggested no benefit of immobilisation in external rotation versus internal rotation. There was low-quality evidence that an open procedure was superior to arthroscopic surgery for preventing shoulder redislocations.
Conclusions There was moderate-quality evidence that half of the patients managed with physiotherapy after a first-time traumatic shoulder dislocation did not experience recurrent shoulder dislocations. If chronic instability develops, surgery could be considered. There was no evidence regarding the effectiveness of surgical management for post-traumatic chronic shoulder instability.
- shoulder
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The shoulder is the most commonly dislocated large joint.1 A traumatic shoulder dislocation is often accompanied by a labral lesion,2–7 which predisposes the patient to developing chronic shoulder instability.8–11 The incidence of primary shoulder dislocation varies between 15.31 and 56.312 per 100 000 person-years. Most patients are men aged under 40 years and most dislocations are sports injuries. Both these facts make shoulder dislocation and possible subsequent chronic instability an important health issue for young, active patients and their treating clinicians.13
Acute treatment of a dislocated shoulder is closed reduction, which should be performed as soon as possible, either on the field or in an emergency department.14 Some patients develop recurrent dislocations or symptomatic subluxations even in daily activities. This has prompted suggestions that surgical stabilisation may be indicated after the first dislocation—a treatment strategy that has been investigated in several randomised controlled trials (RCT), with mixed results.3 4 6 7 15 16
There is considerable variation in the management of patients after a primary traumatic shoulder dislocation (both between surgeons and disciplines).17 18 Most patients with chronic post-traumatic shoulder instability are offered stabilisation surgery, while the surgical methods vary widely.17–20 Some evidence suggests that in the management of musculoskeletal conditions patients are more likely to undergo surgical treatment if the treating physician is a surgeon versus a non-surgical specialty (eg, physiotherapy),21 and that surgeons more easily recommend surgical treatment if the evidence regarding the effectiveness of surgery is inconclusive.19 Thus, to provide the best care, physiotherapists, physical medicine specialists, sports medicine specialists and orthopaedic surgeons should know what is the best quality evidence for treatment of shoulder instability.
Therefore, we aimed to assess the current evidence regarding the effectiveness of interventions after primary traumatic shoulder dislocation and in chronic post-traumatic shoulder instability. Our systematic review focused on two clinical effectiveness questions regarding post-traumatic shoulder instability: (1) What are the best treatments to reduce the incidence of chronic shoulder instability after a first-time traumatic shoulder dislocation? and (2) How can the clinician best treat a patient with chronic post-traumatic shoulder instability?
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement22 when conducting and reporting this prospectively registered systematic review (PROSPERO registration ID: CRD42015020303). We use dislocation to refer to a true dislocation of the joint and instability to refer to dislocations, subluxations or other symptoms of instability either alone or together. By recurrent dislocation(s) and redislocation(s) we mean one or more dislocations after the primary episode, and by chronic post-traumatic instability we mean recurrent dislocation(s), subluxations or other symptoms of instability occurring after a first-time traumatic shoulder dislocation.
Data sources and searches
We searched Ovid MEDLINE, Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews, Embase, Scopus, CINAHL, Ovid MEDLINE Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Ovid MEDLINE Daily, Database of Abstracts of Reviews of Effect (DARE), Health Technology Assessment Database, NHS Economic Evaluation Database and Web of Science on 15 January 2018. There were no restrictions on language or publication date. We adjusted the search strategies to meet the specifications of the individual databases (online supplementary appendix 1). We reviewed the reference lists of included publications and earlier reviews to identify any additional studies that were missed in the electronic database search. We also searched the WHO International Clinical Trials Registry Platform (WHO ICTRP) (www.who.int/ictrp) on 23 January 2018 for registrations of the included RCTs, possible completed but unpublished RCTs and ongoing RCTs.
Supplemental material
Study selection
We included RCTs that compared any interventions after a first-time, traumatic shoulder dislocation or chronic post-traumatic shoulder instability with a follow-up of at least 1 year. We required an outcome measure related to shoulder instability, shoulder function or quality of life. We excluded studies of treatment of non-traumatic shoulder instability, cadaveric or biomechanical studies and studies on secondary shoulder instability (such as neurological conditions, syndromes or congenital conditions). Two investigators (LK and TL) independently assessed all identified publications for eligibility and resolved any disagreements by consensus.
Data extraction and risk of bias assessment
We categorised the included publications according to the two clinical scenarios under review (first-time traumatic shoulder dislocation and chronic post-traumatic shoulder instability). We extracted the outcome data for all available follow-up assessments. For primary shoulder dislocation, we used redislocation data from 1-year and 2-year follow-ups as defined in the individual studies. If numeric outcome data were unavailable, we extracted the data from figures and graphs.
In addition to the outcome measures, we extracted the following information regarding the trial characteristics and participants: study objectives, inclusion and exclusion criteria, number of patients allocated to intervention and control groups, follow-up time, sex distribution, mean age, proportion of sports injuries, indications for surgery, treatments for the intervention and control groups, associated soft-tissue and bony injuries, prespecified and reported harms, sample size estimations, study sponsorships and conflict of interest statements and trial registry identifiers. We extracted the method of randomisation and randomisation sequence generation, allocation concealment, degrees of blinding, loss to follow-up, intention-to-treat analysis, selective reporting, similarity of patient groups, cointerventions, compliance and timing of the outcome assessment. All data were extracted to a customised worksheet independently by two reviewers (LK and TL). We sent emails to authors of potentially eligible conference abstracts, publications with no available source data and unpublished trials and inquired about the status of the trial and requested data to be included in the meta-analyses.
Two reviewers (LK and TL) independently assessed the study-level risk of bias according to the guidelines of the Cochrane Back Review Group.23 The risk of bias assessment has 12 independent criteria; with a judgement of ‘yes’, ‘unclear’ or ‘no’. If at least six of the 12 criteria were judged to be at low risk of bias (‘yes’), the risk of bias in the publication was considered low.23
To assess possible selective reporting of results, we compared the outcome measures specified in the methods section of the publication and in the trial registry (if available) to what was reported in the results section of the publication. For the analysis of the timing of the outcome assessment, we deemed a deviation of 3 months (in a 2-year follow-up) to be an acceptable range. Disagreements between the two reviewers on the retrieved data were resolved by consensus. If any item was unclear, we contacted the authors by email to clarify the issue.
Researcher conflict of interest and industry sponsorship have been identified as potential sources of bias.24–26 We evaluated and noted the existence of these potential sources of bias in the studies.
Data synthesis and analysis
We performed meta-analyses of clinically homogenous studies (patient populations, indications of treatment, intervention pairs and outcomes). If studies with same intervention-control pairs were not sufficiently homogenous, we performed multiple pairwise meta-analyses of the trials with poolable patients and data. In the analysis of surgical treatment after first-time shoulder dislocation, we performed a frequentist network meta-analysis to assess the effectiveness of surgical treatment alternatives at matching time points available in the source data. We prioritised outcomes at 2 years since the majority of shoulder redislocations take place within that time.27–33 If a trial had reported outcomes at multiple time points, we used data from one time point only in a single analysis. We calculated the number needed to treat (NNT) and number needed to harm (NNH)34 for interventions with dichotomous outcomes and statistically significant between-group comparisons. For shoulder redislocations, the NNT is the number of patients who need to receive a treatment to prevent one patient having a shoulder redislocation. The NNH is the number of patients who need to be treated in a certain way to cause a redislocation. For NNT estimates we used the point estimate of the relevant risk ratio, base redislocation risk from a systematic review (21%–47%, minimum follow-up of 2 years)35 and the redislocation rates in the relevant included trials.
We based all analyses on random effects models due to expected variation among patients and outcome measurements. Statistical heterogeneity was quantified with the I2 statistic. Sensitivity analyses or metaregression was not performed to explore heterogeneity or the effect of bias. In the network meta-analysis (NMA), the assumption of exchangeability was evaluated qualitatively. Inconsistency was evaluated using tau2 and Cochran Q statistic and corresponding p values, and the Netheat plot.36 Use of quantitative methods to assess exchangeability or the use of p score to estimate the best treatment was not possible due to the low number of trials in the network. We did not plan subgroup analyses.
We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to rate the quality of evidence and present a summary of findings table.37 We downgraded for inconsistency if the magnitude or direction of effects were dissimilar, the CIs had minimal overlap, the test of heterogeneity was significant or if the I2 was >50%. For imprecision, we downgraded if the CIs were very wide or if the Optimal Information Size criteria were not met. We used Review Manager (RevMan) (V.5.3.5)38 for the meta-analyses, the netmeta package36 in R (V.3.2.1)39 for the network meta-analysis and GRADEpro GDT40 for the GRADE judgements and summary of findings tables.
Patient involvement
The study did not involve patients.
Results
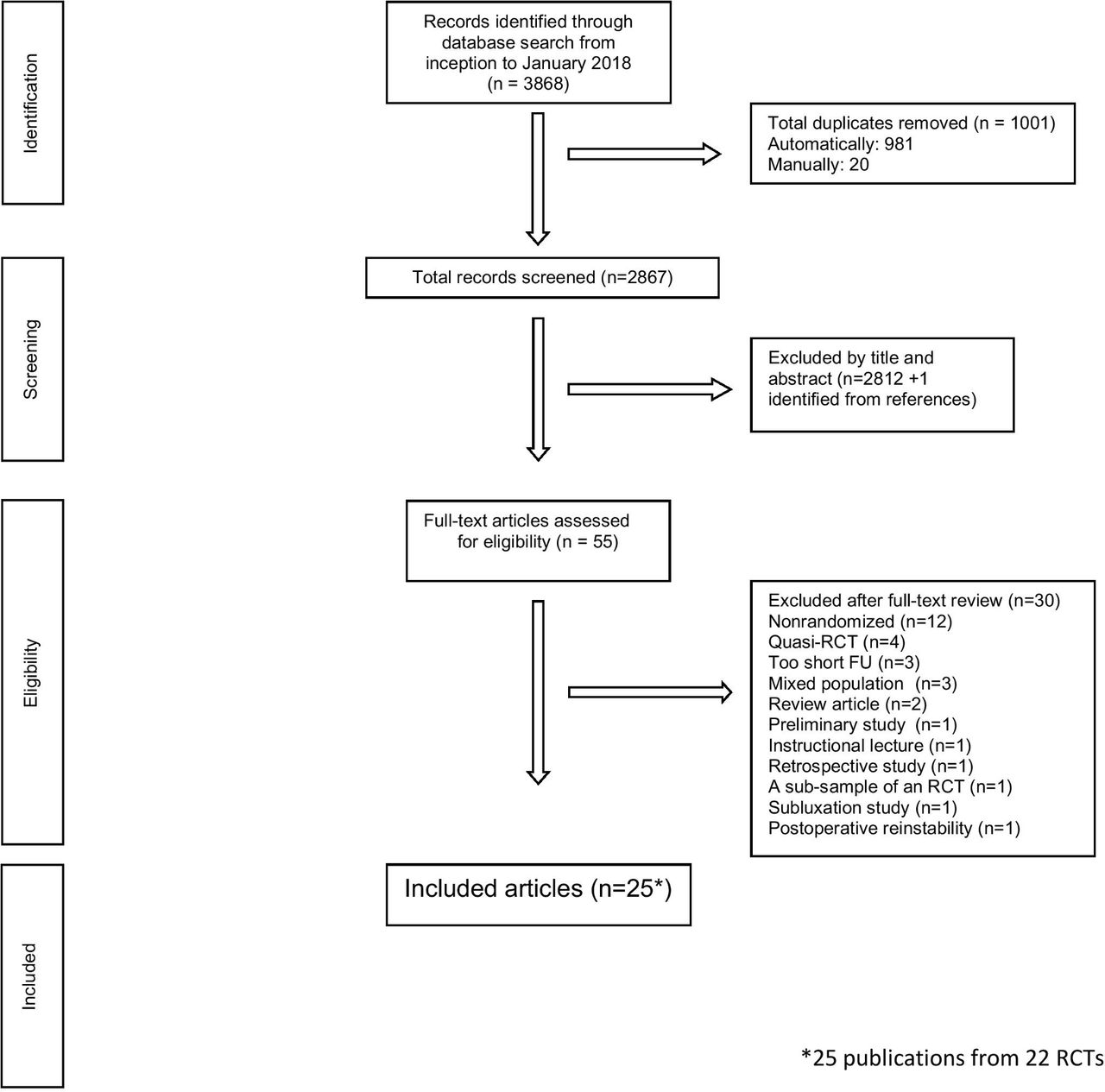
The literature search yielded 2867 reports after exclusion of duplicates. Of these reports, 55 were considered for inclusion after review of titles and abstracts (figure 1). After full-text review, 25 publications (22 RCTs) were included (figure 1). Studies excluded at the full-text screening stage are presented in online supplementary appendix table 1. We identified six unpublished RCTs (online supplementary appendix table 2). Five of these explored external rotation (ER) versus internal rotation (IR) as a treatment for a first-time traumatic shoulder dislocation. We did not receive data of any trial. We identified 20 ongoing RCTs (online supplementary appendix table 3).
Supplemental material
Supplemental material
Supplemental material

Study accrual flow chart.
Of the 22 included RCTs, 10 investigated treatment after a first-time traumatic shoulder dislocation. Four studied whether early surgery was beneficial after a first-time traumatic shoulder dislocation,3 4 6 7 15 16 and five compared the effect of upper limb immobilisation in ER versus IR in preventing further instability.41–45 Twelve RCTs focused on chronic post-traumatic shoulder instability, of which four RCTs compared open labral repair with arthroscopic labral repair2 5 46 47 and three compared absorbable with non-absorbable suture anchors.48–50
Mean participant age ranged from 20.3 to 36 years. The mean follow-up ranged from 12 to 143 months. In 15 RCTs, 67% of the primary dislocations were sports injuries; seven RCTs did not report injury mechanism.2 5 45 46 50–52 One study included patients with large bony defects of the glenoid.52 The trials are summarised in table 1; online supplementary appendix tables 4 and 5 present all extracted data.
Summary of included studies
Risk of bias assessment
All trials were of parallel-group, prospective design. Twenty-one were classical RCTs; one used a minimisation algorithm.6 Two trials were double blind,6 49 seven were single blind4 15 45 48 51 53–56 and 13 were not blinded.2 3 5 7 16 41–44 46 47 50 52 57 Loss to follow-up ranged from 0% to 20%. Intention-to-treat analysis was reported in all publications. The sample sizes ranged from 30 to 198 participants. Sample size estimation was described by 14 trials4–6 15 41–45 47 48 52–54 56 57; one of these met the prespecified assumptions of the sample size estimation.42 Levels of evidence of the included trials are presented in online supplementary appendix table 6.
Supplemental material
Risk of bias was high in two RCTs.41 50 There was a high risk of detection bias due to variation in the timing of the follow-up assessments; three43 44 48 (14%) of the 22 trials met the minimum criterion of less than 3-month discrepancy between scheduled and actual follow-up visit (online supplementary appendix table 7).
Supplemental material
Two trials disclosed a potential conflict of interest and industry sponsorship,54 57 three disclosed industry sponsorship43 50 55 and five disclosed either conflict of interest or industry sponsorship.3–5 52 53 Six trials made an explicit statement of no conflicts of interest or industry sponsorship,6 41 42 44 45 47 and nine did not mention conflict of interest or industry sponsorship (online supplementary appendix table 7).2 7 15 16 46 48 49 51 56
GRADE analysis and summary of findings
The quality of evidence varied from very low to moderate. The most common reasons for downgrading were absence of blinding and imprecision. Summary of findings tables are presented below within the subsections of synthesis of results.
Synthesis of results
First-time traumatic shoulder dislocation
Early surgery
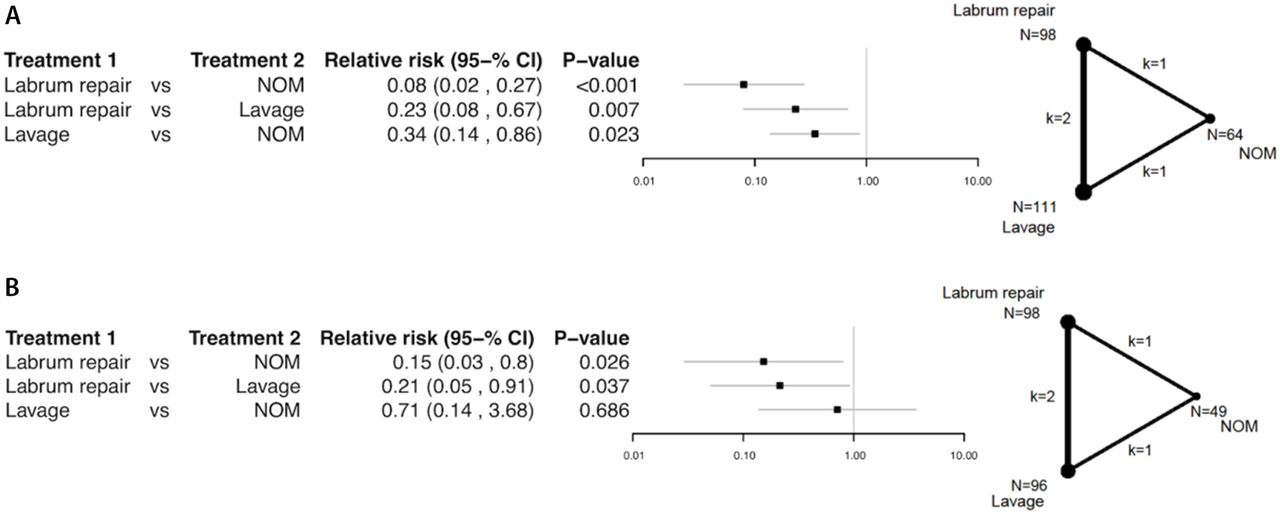
Patients who underwent surgery to repair a labral injury (ie, Bankart repair) had fewer redislocations than patients who received non-surgical management or arthroscopic lavage of the glenohumeral joint at 1 year (four studies, 273 patients)3 4 6 7 (relative risk (RR) labrum repair vs non-surgical management 0.08; 95% CI 0.02 to 0.27, p<0.001 and labrum repair vs arthroscopic lavage 0.23; 95% CI 0.08 to 0.67, p=0.007, I2=0%, p=0.46) and 2 years (four studies, 243 patients)3 4 6 16 (RR labrum repair vs non-surgical management 0.15; 95% CI 0.03 to 0.8, p=0.026 and labrum repair vs arthroscopic lavage RR 0.21; 95% CI 0.05 to 0.91, p=0.037, I2=63.6%, p=0.064) (figure 2A,B; table 2). There was a benefit of arthroscopic lavage at 1 year over non-surgical management (RR 0.34; 95% CI 0.14 to 0.86, p=0.023) (figure 2A); this effect was not evident at 2 years of follow-up (RR 0.71; 95% CI 0.14 to 3.68, p=0.686) (figure 2B). Tests for inconsistency were insignificant at both time points. Direct meta-analysis was possible between studies comparing labrum repair and arthroscopic lavage (two studies, 160 patients).3 6 There was a treatment effect in favour of labrum repair (RR 0.13; 95% CI 0.03 to 0.69, p=0.02, I2=54%, p=0.14) (online supplementary appendix figure 1). The NNT to prevent a redislocation at 2 years ranged from 2.5 to 5.6 based on external data35 and 2.0 and 4.73 4 6 using the redislocation rates in the included RCTs.
Supplemental material

{kind=link}
{kind=link}
Relative risk (RR) of a redislocation after treatment of a first-time traumatic shoulder dislocation at (A) 1 year and at (B) 2 years derived from the network meta-analysis.
Summary of findings for labrum repair after a first-time traumatic shoulder dislocation
Arm position
Immobilisation in ER (vs IR) had no effect on the redislocations or chronic instability (table 3). Due to heterogeneity of the trials, three separate direct comparison meta-analyses comparing immobilisation in ER versus IR were performed: one of trials with young patients and narrow age range reporting redislocations, second of a subset of the former reporting instability and a third of older patients with a wide age range reporting instability. In none did the arm position affect the outcome. Three trials (287 patients)41 44 45 had a narrow age range with an average age of approximately 25 years reporting redislocations (RR 1.07; 95% CI 0.76 to 1.50; p=0.70; I2=0%; p=0.65) (online supplementary appendix figure 2a); two of these trials (236 patients)44 45 also reported recurrent instability (RR 1.01; 95% CI 0.82 to 1.24; p=0.90; I2=0%; p=0.78) (online supplementary appendix figure 2b). Two trials (261 patients)42 43 had a wide age range with an average age of approximately 35 years and reported recurrent instability (RR 0.31; 95% CI 0.06 to 1.68; p=0.17; I2=82%; p=0.02) (online supplementary appendix figure 2c).
Supplemental material
![[SP4.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC8/embed/inline-supplementary-material-8.jpg?download=true){kind=link}
Supplemental material
![[SP5.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC9/embed/inline-supplementary-material-9.jpg?download=true){kind=link}
Supplemental material
![[SP6.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC10/embed/inline-supplementary-material-10.jpg?download=true){kind=link}
Summary of findings for immobilisation in external versus internal rotation after a first-time traumatic shoulder dislocation
Restriction band usage
There was one trial investigating the use of a shoulder motion restriction band after immobilisation in ER (vs immobilisation in ER only). The restriction band had no effect on shoulder redislocation rates.57
Chronic post-traumatic shoulder instability
Open versus arthroscopic surgery
There was a statistically significant difference in favour of open labrum repair for preventing redislocations (three studies, 269 patients) (RR 0.43; 95% CI 0.19 to 0.97; p=0.04; I2=0%; p=0.43) and instability (two studies, 223 patients) (RR 0.49; 95% CI 0.26 to 0.92; p=0.03; I2=0%; p=0.99) (online supplementary appendix figure 3a,b; table 4). The NNH was approximately 12, defined here as a redislocation that would not have occurred if open instead of arthroscopic technique had been used.
Summary of findings for open compared with arthroscopic labrum surgery in treatment of chronic post-traumatic shoulder instability
Absorbable versus non-absorbable suture anchors, tacks or suture materials
There were no differences in recurrent instability rates between absorbable and non-absorbable suture anchors (three studies, 232 patients)48–50 (RR 0.62; 95% CI 0.21 to 1.86; p=0.40; I2=0%; p=0.95) (online supplementary appendix figure 4; table 5). The absorbability of tacks or suture material had no effect on recurrent instability rate.48–50 53–55
Supplemental material
![[SP10.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC11/embed/inline-supplementary-material-11.jpg?download=true){kind=link}
Summary of findings for use of absorbable compared with non-absorbable implant materials in labrum surgery in treatment of chronic post-traumatic shoulder instability
Accelerated versus traditional postsurgical rehabilitation and different surgical procedures
There was one trial investigating each of these topics. Neither the pace of rehabilitation after surgical intervention nor the surgical method had any effect on the redislocations or chronic instability.51 52 56
Harms
Three publications specified and reported harms as a study outcome a priori.5 6 44 Thirteen publications reported harms occurrence but did not list harms as a prespecified outcome.2–4 7 41–43 46 47 49 51 53 54 Nine publications did not mention harms.15 16 45 48 50 52 55–57 There were 19 patients (1.5%) with temporary pain, rigidity or stiffness in the treated shoulder, 17 patients (1.3%) with transient nerve injuries, 5 patients (0.39%) with superficial wound infections, 3 patients (0.24%) with cases of adhesive capsulitis and 1 patient (0.08%) with septic arthritis in the shoulder (online supplementary appendix table 5).
Supplemental material
Discussion
Our review aimed to answer two patient-oriented questions relevant to clinical practice: (1) What are the best treatments to reduce the incidence of chronic shoulder instability after a first-time traumatic shoulder dislocation? and (2) How should the clinician best treat a patient with chronic post-traumatic shoulder instability? Evidence regarding the comparative effectiveness of surgery versus non-surgical treatment is currently available only for a first-time traumatic shoulder dislocation: early surgery led to fewer shoulder redislocations. However, approximately half of the patients primarily treated non-surgically do not experience a shoulder redislocation or develop shoulder instability within 2 years of the primary injury. Immobilisation in ER was not beneficial after a first-time traumatic shoulder dislocation compared with immobilisation in IR.
For the treatment of chronic post-traumatic shoulder instability, we did not identify any RCTs that assessed the effectiveness or efficacy of surgery versus non-surgical measures or sham surgery. Open Bankart repair produced more reliable results than the arthroscopic method for prevention of shoulder redislocations. There were no differences between other technical aspects of surgery.
Treatment after a first-time traumatic shoulder dislocation
Labrum repair was more effective than non-surgical treatment for first-time dislocation in terms of fewer redislocations. Arthroscopic lavage was no more effective at 2 years compared with non-surgical treatment, making arthroscopic lavage a candidate placebo surgical treatment in this context. Our NMA indicated a beneficial effect of labrum repair on the incidence of shoulder redislocation when compared with non-surgical treatment. The NNT—in this context the number of patients who needed to undergo surgery to prevent one patient having a shoulder redislocation—was 2.5–5.6 based on external data35 and 2.0–4.7 based on the data in the included trials.3 4 6
Regarding disease-specific quality of life, no meaningful meta-analysis was possible. There were some differences between the treatment alternatives in favour of labrum repair (online supplementary appendix table 5).4 6 Even though the differences were small, they were consistent with and explained by the reduced risk of shoulder redislocations and chronic instability in the groups treated with labrum repair.
The study populations in the included RCTs consisted mostly of young men and the majority of dislocations were sports related, making the results applicable to the typical patient, but the generalisability to women, non-athletes and older patients is uncertain. Our results are less favourable towards surgery than those presented by previous systematic reviews and meta-analyses.58 59 This difference might be attributed to a strict inclusion of RCTs only, the handling of labrum repair, arthroscopic lavage and non-surgical treatment as separate entities and the use of NMA. Overall, since only about half of the patients in the included studies and in a large long-term prospective cohort60 suffered shoulder redislocations and the NNTs are relatively high, the prevailing practice17 of low-threshold surgery after a first-time shoulder dislocation can be questioned. Previous studies have suggested that delaying surgery and waiting to see whether the patient developed chronic instability after a first-time traumatic shoulder dislocation did not lead to a less favourable prognosis of instability, quality of life or glenohumeral joint osteoarthritis.61 62 Compared with routine surgery after a first-time traumatic shoulder dislocation, waiting to see if a patient develops chronic instability despite rehabilitation might direct resources more efficiently and may save half of patients from unnecessary surgery.
Arm position after primary traumatic shoulder dislocation (immobilisation in ER vs IR) had no effect on the risk of redislocations or chronic shoulder instability. This finding is consistent with other meta-analyses.63–66 The number of unpublished trials investigating immobilisation in ER identified was equal to the number of RCTs included in this review, which raises concerns of publication bias. Immobilisation in an ordinary arm sling for comfort appears to be preferable to the use of an ER brace.
Chronic post-traumatic shoulder instability
There were no RCTs exploring the effectiveness of surgery versus non-surgical treatment, which is an important evidence gap. Open labrum repair appears to be more effective than arthroscopic labrum repair in successfully stabilising an unstable shoulder, while there was no difference in other outcomes or harms. The point estimate for the RR was 0.43; this means that arthroscopic technique was more than twice as likely to fail as open technique, and the NNH was approximately 12, defined here as a shoulder redislocation that would not have occurred if open technique had been used instead of arthroscopy. Previous meta-analyses, which have also included non-randomised studies, have suggested no difference between open and arthroscopic techniques67–73 or a difference in favour of the open method.74–76 Although we have witnessed a rapid increase in the popularity of arthroscopy within the past two decades to the point of it being considered the accepted standard,77–81 our findings might justify a tempering of enthusiasm for the arthroscopic method. On the other hand, even though the perceived effectiveness of surgery might be overestimated since the natural course of chronic post-traumatic shoulder instability is largely unknown, the results of surgery for chronic instability are encouraging in terms of the low redislocation rates after surgery in the included trials.
Study bias
The risk of bias among the included RCTs was relatively low. However, concern for confounding still exists, as there was considerable heterogeneity in the follow-up time and less than half (41%) of the studies used any kind of blinding. In most trials, the primary outcome was recurrent dislocation, a relatively ‘hard’ endpoint. However, in the included RCTs, the definition of redislocation varied from a solely symptoms-based diagnosis to one that was confirmed radiographically or alternatively, an event that required a manual reduction. Analysis on the effect of conflicts of interest or industry sponsorship on trial results was not possible due to heterogeneity.
Limitations
The use of shoulder instability-validated outcome instruments was rare4 6 15 42 44 45 47 52 and baseline values were seldom reported.45 47 The publications also generally did not meet the assumptions of the power calculations, making a type II error possible. Another limitation is publication bias in the field, as studies with ‘negative results’ for the intervention are more likely to remain unpublished,82 risking overestimation of the true effect in meta-analyses. A methodological limitation is that no sensitivity analyses or meta-regression were performed. Finally, our findings apply only to patients with almost intact bony glenoids, as in all but one trial no marked bony defects of the glenoid were present among the patients.52 This has direct clinical relevance as shoulder dislocation occasionally causes a sizeable glenoid fracture, or the glenoid bone may erode with numerous redislocations.83
A limitation to the clinical relevance of our findings is that the effect of a shoulder redislocation on patient quality of life remains unclear. An occasional shoulder dislocation may result in mild discomfort while the shoulder functions otherwise normally. In contrast, a subjectively unstable shoulder may be associated with constant fear of dislocations, kinesiophobia and poor function even in the absence of redislocations.4 84 If the primary treatment aim was to prevent redislocations only, shoulder arthrodesis would be very effective. However, such a treatment would also likely be associated with poor functional outcomes, and we might reasonably expect this treatment and outcome is not desired by patients.85
Future research
The most important evidence gaps regarding clinical practice are the effectiveness of surgery for chronic post-traumatic shoulder instability and what is the ideal physiotherapy regime for non-surgical management after a primary traumatic dislocation or for chronic post-traumatic instability. The impact of surgery to patient quality of life should also be investigated. Future trials should be adequately designed,86 87 powered and reported,88 and use validated measures of disability or function in addition to the shoulder redislocation rate. Due to the placebo effects associated with surgery, further trials should be double blinded and placebo controlled whenever possible.6 89 90
Conclusions
There was an RR of 0.15 (95% CI 0.03 to 0.8) for a recurrent dislocation after first-time traumatic shoulder dislocation in favour of labrum repair compared with physiotherapy. The certainty in the evidence was moderate. Forty-seven per cent of patients with a first-time traumatic shoulder dislocation treated non-surgically did not experience a redislocation within 2 years.
What is already known on this subject?
After a first-time traumatic shoulder dislocation, approximately half of patients developed recurrent shoulder dislocation within 2 years.
Some studies have shown promising results with surgery after a first-time traumatic shoulder dislocation. Primary surgery has been advocated to prevent chronic shoulder instability.
Many patients with chronic post-traumatic shoulder instability are offered stabilising surgery. Current practice favours arthroscopic labral repair over open surgery.
What this study adds?
There was moderate-quality evidence that patients who had labrum repair surgery after a first-time traumatic shoulder dislocation had lower recurrent dislocation rates than patients treated with physiotherapy. However, surgical treatment has a relatively high number needed to treat (2.5–5.6) to prevent redislocation.
In the treatment of chronic post-traumatic shoulder instability, effectiveness of surgery compared with non-surgical treatment is not known. Low-quality evidence supported open labrum repair over arthroscopic labrum repair.
Supplemental material
Supplemental material
![[SP7.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC14/embed/inline-supplementary-material-14.jpg?download=true){kind=link}
Supplemental material
![[SP8.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC15/embed/inline-supplementary-material-15.jpg?download=true){kind=link}
Supplemental material
![[SP9.jpg]](https://bjsm.bmj.com/content/bjsports/52/23/1498/DC16/embed/inline-supplementary-material-16.jpg?download=true){kind=link}
Supplemental material
Acknowledgments
We thank Professor Teppo Järvinen for his insightful comments and critical review of the manuscript, information specialist Ritva Miikki for the database searches and Teppo Huttunen and Joni Keto-Tokoi of 4Pharma for assistance with the NMA.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.
Footnotes
LK and TL contributed equally.
Contributors LK, TL, AM and MP all participated in the conception and design of the study. LK and TL acquired the data. LK performed the analyses and TL, AM and MP participated in interpreting the analyses. TL and LK drafted the manuscript. All authors critically revised and approved the final version of the manuscript.
Funding LK has received a research grant from Finnish Research Foundation for Orthopaedics and Traumatology (FRFOT) and from the Helsinki Academic Medical Centre. TL has received a research grant from the FRFOT.
Disclaimer The funders had no role in any part of the study or in any decision about publication.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The study protocol is available from the PROSPERO registry, https://www.crd.york.ac.uk/prospero/ with the identifier CRD42015020303. Statistical codes are available for the Netmeta package in program R (online supplementary appendix 2) and RevMan (online supplementary appendix 3). Full data are presented in online supplementary appendix tables 2–7.