Article Text

Abstract
Objectives The effect of shoe-worn insoles on biomechanical variables in people with medial knee osteoarthritis has been studied extensively. The majority of research has focused specifically on the effect of lateral wedge insoles at the knee. The aim of this systematic review and meta-analysis was to summarise the known effects of different shoe-worn insoles on all biomechanical variables during level walking in this patient population to date.
Methods Four electronic databases were searched to identify studies containing biomechanical data using shoe-worn insole devices in the knee osteoarthritis population. Methodological quality was assessed and a random effects meta-analysis was performed on biomechanical variables reported in three or more studies for each insole.
Results Twenty-seven studies of moderate-to-high methodological quality were included in this review. The primary findings were consistent reductions in the knee adduction moment with lateral wedge insoles, although increases in ankle eversion with these insoles were also found.
Conclusion Lateral wedge insoles produce small reductions in knee adduction angles and external moments, and moderate increases in ankle eversion. The addition of an arch support to a lateral wedge minimises ankle eversion change, and also minimises adduction moment reductions. The paucity of available data on other insole types and other biomechanical outcomes presents an opportunity for future research.
- orthotics
- knee
- osteoarthritis
- systematic review
- biomechanics
Statistics from Altmetric.com
Introduction
Knee osteoarthritis (OA) is a chronic degenerative joint disease and leading cause of long-term physical disability. There is a growing body of literature reporting the effects of non-surgical treatments on biomechanical outcomes. Biomechanical outcomes, such as the external knee adduction moment (KAM), are important to monitor as abnormal joint loading patterns are associated with OA disease progression.1 2
Shoe-worn foot orthotic devices (insoles) are an inexpensive intervention for potentially altering knee joint biomechanics. While off-the-shelf shock absorbing insoles are frequently used by members of the general public with knee OA, lateral wedge insoles (LWIs—insoles with a raised lateral border) have received the majority of research attention. Importantly, LWIs reduce certain biomechanical risk factors of OA progression such as the KAM.3 However, despite shoe-worn insoles such as LWIs reducing KAM values, a recent systematic review reported that lateral wedges provide no additional clinical improvements in pain when compared with a neutrally aligned insole.4
One limitation of most biomechanics studies examining shoe-worn insoles has been the focus on changes in knee biomechanics (predominantly the KAM)—data are generally lacking on the effect of the insoles at other joints or on other biomechanical outcomes.5 6 Now, a growing number of studies have examined the effects of shoe-worn insoles on other joints such as the hip7 and ankle.8 Given that shoe-worn insoles evoke changes directly at the foot/shoe interface9 —with anticipated changes experienced more proximally at the knee joint—a thorough understanding of their effects on joints other than the knee is needed to best guide their use in the clinical management of knee OA. Therefore, the purpose of this review was to conduct a systematic search of the existing literature to identify kinematic and kinetic changes in walking gait biomechanics in this patient population with the use of shoe-worn insoles.
Methods
Literature search strategy
A comprehensive search was performed using the following electronic databases: Medline, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase and SPORTDiscus. The final search was conducted on 22 June 2016. Two researchers (CP and CDV) conducted the search and determined the final eligibility based on full-text screening. Eligibility was determined independently by these two reviewers, with differences rectified via consensus discussion. The search strategy was as follows (identical for all databases): (1) osteoarthritis, knee/ (2) ((osteoarthritis or osteoarthritides or osteoarthros*) adj3 knee*).mp (3) 1 OR 2 (4) orthotic devices/ or foot orthoses/ (5) ((insole or foot or shoe*) adj3 (device* or orthotic* or insert* or orthos*)).mp (6) 4 OR 5 (7) 3 AND 6 (8) gait.mp or exp gait/ (9)walk*.mp (10) walking/ (11) or/8–10 (12) foot joints/ or knee joint/ or ankle joint/ (13) ((foot or knee or ankle) adj3 joint*).mp (14) biomechanical phenomena/ (15) (biomech* or kinematic* or kinetic*).mp (16) or/12–15 (17) 11 OR 16 (18) 7 AND 17. No limits were placed on publication date or language for the initial search. Recursive hand searching was completed on relevant systematic reviews and based on the reference lists of all publications considered for inclusion. The abstracts of all returned papers were reviewed by two reviewers (CP and CDV); papers that met all inclusion criteria received full-text review by the same two reviewers.
Study selection
Included studies met the following inclusion criteria: human participants with diagnosed knee OA; use of an insertable shoe-worn device; analysis of level walking gait in a motion analysis laboratory and reporting of at least one biomechanical outcome measure. No restrictions were placed on the severity of knee OA, compartmental involvement or the sex of the participants. Within-subject and within-session data during walking conditions with and without the shoe-worn insole was required. Prospective studies were included only if they measured baseline data as well as the immediate effects of the intervention at the same testing session; thus, studies that examined the latent effects following a period of treatment were excluded as they did not examine the immediate effects of the shoe-worn device. Studies were excluded if the study sample had predominantly additional lower extremity conditions that affected gait; were predominantly composed of comorbidities (eg,rheumatoid arthritis); were comprised solely of patients who had undergone total knee arthroplasty or permitted the use of ambulation aids. Non-experimental and non-English language papers were excluded during the abstract screen.
Publications with similar author names and dates of publication were compared at the data extraction stage to identify any duplication of data. In instances where it was clear that the same data were presented (eg, same mean values for an outcome measure from the same sample size and same sample demographics), duplicate data were only included from the paper with the highest methodological quality index score (see below). Finally, in papers where more than one iteration of the same intervention was tested (eg, different angulations or lengths of the same type of insole), only data from the condition with the largest change (eg, highest degree of wedging or longest length insole) was included.
Methodological quality assessment and data extraction
Methodological quality was assessed independently by two reviewers (MR and JW) using 26 items of the Downs and Black quality index.10 The quality index assessed reporting (items 1–10), external validity (items 11–13) and internal validity (bias and confounding) (items 13–26). As discussed in the literature, item 27 was removed due to item ambiguity.11 The scale was scored out of 27, as item 5 is rated out of a maximum of two points. An a priori threshold of 50% (14/27) on the quality assessment was chosen for inclusion in the data synthesis. Consensus on disagreements was achieved through face-to-face meeting, and in the event that consensus was not reached, a third reviewer (MH) provided input. Agreement between reviewers was assessed using a kappa statistic.
Two reviewers (KS and JC) independently extracted all biomechanical data from the included articles and reached consensus on any discrepancies. Data consisted of publication details; demographic data (sex, height, body mass index (BMI)); OA severity as measured using the Kellegren and Lawrence (K/L) grading system (based on the presence and severity of osteophytes and joint space narrowing12); OA characteristics and relevant study inclusion criteria; intervention details and outcome data (mean and SD, and between-group p values where available). Authors of articles missing data, or data in graphical format only, were contacted, and studies were subsequently excluded if authors did not respond to requests for discrete data.
Data synthesis and analysis
Effect sizes (mean difference/pooled SD) were calculated for all biomechanical outcomes. Data were grouped for synthesis based on 1) the type of intervention; 2) the biomechanical variable; 3) the plane of movement and 4) the particular aspect of given biomechanical variable (if applicable).
A meta-analysis of data was performed on biomechanical variables in three or more studies for the same intervention. The standardised mean difference (SMD) with 95% CI was calculated in a random-effects model within Cochrane Review Manager (RevMan V.5.3), with individual data point contributions weighted by sample size. Aspects of the same biomechanical variable that produce different values (eg, early stance peak KAM and late stance peak KAM) were analysed separately for the purposes of the meta-analysis. However, for outcomes that have a relatively constant magnitude and a single value can be obtained at different time points (eg, the overall peak knee adduction angle vs the knee adduction angle at the early stance peak KAM), data were grouped for the purposes of meta-analysis. Given that many studies required participants to walk at a similar speed between conditions, meta-analyses were not performed on variables that would be influenced by this methodological design including: ground reaction force magnitude, gait speed, step length and cadence. The I2 Index was used to assess heterogeneity between pooled results across the included articles and values were interpreted as: low≤50%; moderate=51%–74% and large≥75%. The calculated SMDs from the meta-analysis were used to examine the magnitude of overall effect sizes, and SMD point estimates were interpreted as: minimal≤0.2; small=0.2–0.49; medium=0.50–0.79 and large≥0.8.13
Results
Literature search and study sample characteristics
The search strategy initially yielded 340 unique papers; 31 passed through the full-text screening and went on to quality assessment screening, and 27 papers were included in the final data analysis (figure 1). Participant demographics were generally well described with respect to mean age, BMI or height and mass and frequency of each sex (table 1). Most studies included both males and females, although five studies only reported data for one sex. The K/L grade of OA severity was reported in 20/27 studies for a total of 580 knees (9% grade 1; 39% grade 2; 40% grade 3; 12% grade 4). Finally, sample sizes ranged from a minimum of 10 to a maximum of 73 participants.

Flow chart for study screening and inclusion. OA, osteoarthritis.
Characteristics of included studies
Methodological quality
Quality assessment scores of the 27 included articles ranged from 19 to 22, with a median and mode score of 20 out of 27, indicating a moderate methodological quality. Based on the initial assessments, overall interobserver agreement was high, with a Cohen’s kappa of 0.91. Agreement of single items ranged from moderate (item 8, κ=0.35) to perfect (items 2, 7, 12, 17, 18, 20, 22 and 26, K=1.0). Consensus was reached on the 63 individual items of disagreement (representing 9.0% of all 702 assessment scores) by the two reviewers at a face-to-face consensus meeting. Single items not met in more than 50% of articles included: item 8—adverse effects (6/27, 22%); item 11—participants representative of the entire population (12/27, 44%); item 12—proportion of invited participants reported (2/27, 7%); item 13—treatment environment representative of standard clinical care (4/27, 15%); item 14—participant blinding (1/27, 4%); item 15—assessor blinding (4/27, 15%) and item 24—concealment of randomisation (0/27, 0%). Blinding participants to the intervention was difficult because of the sensory impact of a shoe-worn insole and visual differences in the design of the active and control insole conditions.
Interventions and outcome measures
The most commonly examined intervention in this review was a lateral wedge insole (23 studies), followed by a lateral wedge with arch support (five studies), medial arch support (one study) and a shock absorbing insole (one study). Three studies examined both lateral wedges and lateral wedges with arch support. A total of 42 different biomechanical variables were identified in this review. Biomechanical variables that were reported in more than 10 studies included the KAM (26/27 studies), gait speed (17/27 studies) and the frontal plane ankle moment (11/27 studies), while 21 different variables appeared in only one study. The number of different variables from a given study ranged from 114 to 30.15 Data are summarised in table 2 and Appendix 1, and summaries by intervention are listed below. Control/comparison conditions are listed for each study in table 2—unless noted, the only difference was the presence or absence of the shoe-worn insole in the same pair of footwear.
Study outcome data—kinematic and joint moments. Positive values indicate: flexion, adduction/varus/inversion, internal rotation at the hip, knee and ankle; varus for segmental angles; ground reaction force medial to the joint centre of interest for moment arm values
Lateral wedge insoles
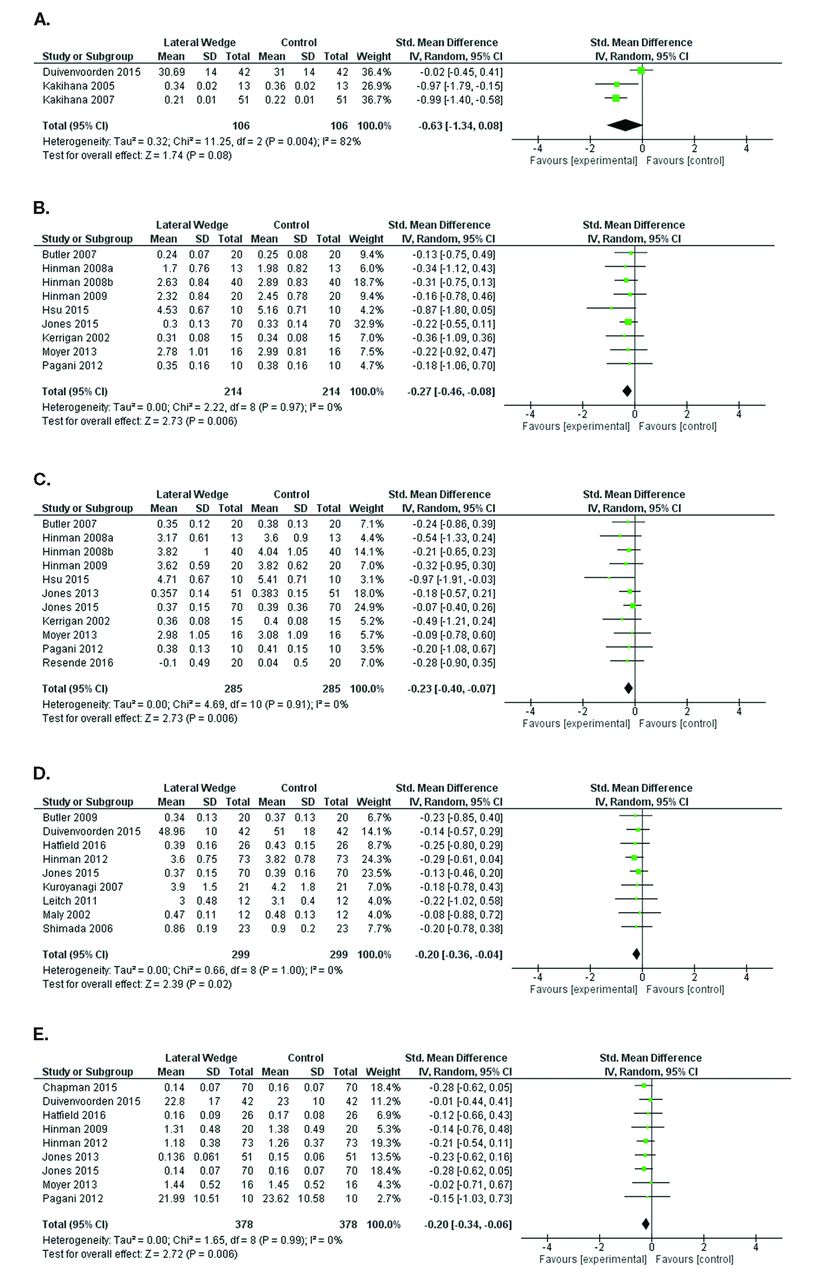
The vast majority of research identified in this review examined LWIs. Overall, LWIs provide a significant reduction in the frontal plane knee moment (KAM). Five separate aspects of the KAM were reported, and data pooling was possible for each (figure 2). The mean KAM throughout stance was shown to be reduced the most with the use of LWIs across three studies (SMD=−0.63), although large heterogeneity (I2=82%) and a 95% CI that crossed zero (95% CI: −1.34 to 0.08, p=0.08) does not provide strong enough evidence for firm conclusions. In contrast, significant reductions in the late stance peak KAM across 9 studies (SMD=−0.27, 95% CI: −0.46 to –0.08, I2=0%, p=0.006), the early stance peak KAM across 11 studies (SMD=−0.23, 95% CI: −0.40 to –0.07, I2=0%, p=0.006), the overall peak KAM magnitude across 9 studies (SMD=−0.20, 95% CI: −0.36 to –0.04, I2=0%, p=0.02) and the KAM impulse across 9 studies (SMD=−0.20, 95% CI: −0.34 to –0.06, I2=0%, p=0.006) provided more conclusive evidence of a small-to-medium effect of LWIs on the KAM.

Forest plots (standard mean differences and 95% CIs) for the effects of lateral wedge insoles on the external knee adduction moment (KAM). (A) Mean KAM; (B) late stance peak KAM; (C) early stance peak KAM; (D) overall peak KAM; (E) KAM impulse.
Six studies reported changes in the frontal plane knee angle with the use of LWIs, and showed some reduction in knee adduction/varus (Appendix 2). However, a minimal and statistically non-significant change was observed, thereby questioning the strength of the effect (SMD=−0.12, 95% CI: −0.32 to 0.08, I2=0%, p=0.24). Similar findings were found with respect to the frontal plane moment arm of the ground reaction force at the knee across five studies (figure 3). Although a small reduction in the varus moment arm was seen, there was large heterogeneity in the data, resulting in a statistically non-significant finding (SMD=−0.39, 95% CI: −0.87 to 0.08, I2=64%, p=0.11).

Forest plots (standard mean differences and 95% confidence intervals) for the effects of lateral wedge insoles on ankle/subtalar joint biomechanics. (A) ankle/subtalar eversion angle; (B) external ankle/subtalar eversion moment; (C) frontal plane ground reaction force moment arm at the knee.
Eight studies examined the effects of LWIs on ankle biomechanics. For the purposes of the meta-analysis, unlike the KAM, the magnitudes of the ankle/subtalar eversion angle and moment were deemed to be relatively consistent between 20% and 80% of stance,16 and data were pooled from studies reporting overall peaks, mean values and values at the time of early and late stance KAM peaks (figure 3). In general, LWIs produce small-to-medium increases in ankle/subtalar eversion angles (SMD=−0.48, 95% CI: −0.91 to –0.06, I2=77%, p=0.03) and subsequently large increases in external ankle eversion moments (SMD=−0.84, 95% CI: −1.41 to –0.27, I2=77%, p=0.0003), however, large heterogeneity in each variable reduces the strength of the evidence. Finally, three studies reported the frontal plane moment arm of the ground reaction force at the ankle (figure 3) and found a large, but statistically non-significant, increase of the valgus moment arm (SMD=−2.00, 95% CI: −4.30 to 0.29, I2=96%, p=0.09), which had high heterogeneity among the studies.
A number of other biomechanical variables were reported with lateral wedge insole use across all three lower limb joints and all three planes of motion, as well as segmental angles. However, most were only reported in a single study and therefore data pooling was not possible and firm conclusions cannot be reached for any variable except peak hip adduction angle. Three studies reported the early stance peak hip adduction and found minimal effect of LWIs (SMD=0.01, 95% CI: −0.25 to 0.27, I2=0%, p=0.96) (Appendix 2).
Spatiotemporal and global kinetic variables that were included in the meta-analysis included step width and the mediolateral position of the centre of pressure (Appendix 2). Use of LWIs result in a small increase in step width based on three studies (SMD=0.28, 95% CI: 0.01 to 0.55, I2=0%, p=0.05), while the centre of pressure had a large lateral shift (SMD=−0.83, 95% CI: −1.37 to –0.29, I2=75%, p=0.003), although there was high heterogeneity among the four studies.
Lateral wedge insoles with arch support
Minimal effect was found for either the early stance peak KAM across four studies (SMD=−0.16, 95% CI: −0.38 to 0.06, I2=0%, p=0.16) or KAM impulse across three studies (SMD=−0.14, 95% CI: −0.37 to 0.08, I2=0%, p=0.22) when using LWIs with arch support. Similarly, although a large effect was found on the frontal plane ankle/subtalar moment (SMD=−0.96, 95% CI: −2.20 to 0.28, I2=90%, p=0.13), this was statistically non-significant due to large interstudy heterogeneity (figure 4). Other biomechanical variables were only reported in one or two studies, and therefore a meta-analysis was not performed.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots (standard mean differences and 95% CIs) for the effects of lateral wedge insoles with arch support on joint moments. (A) Early stance peak external knee adduction moment (KAM); (B): KAM impulse; (C) external ankle/subtalar eversion moment.
Medial arch supports and shock absorbing insoles
Only one study each was identified that examined the use of medial arch supports17 or shock absorbing insoles,18 and therefore data pooling was not possible. However, Hinman et al 17 found no statistically significant changes with medial arch supports in any aspect of the KAM or external hip adduction moment, while Turpin et al 18 found no changes with shock absorbing insoles in any aspect of the KAM.
Discussion
In our systematic review of the biomechanical effects of shoe-worn insoles throughout the body during level walking in individuals with knee OA, we identified four different insole interventions: LWIs with and without arch support, medial arch supports alone and shock absorbing insoles. Pooled data indicate that LWIs produce small-to-medium reductions in the KAM, while the addition of arch supports to wedges produced non-significant reductions in this biomechanical outcome. A limited amount of literature indicates that LWIs increase the amount of eversion at the ankle/subtalar joint and subsequent external eversion moments, while the addition of arch supports do not change ankle eversion. As discussed below, the interplay between foot and knee biomechanics must be considered when determining the clinical appropriateness of these devices for patients.
Taken together, this review extends the findings of previous systematic reviews and meta-analyses by examining the larger kinetic chain, not the knee alone. Importantly, this approach has shown that use of shoe-worn insoles—LWIs in particular—has implications on the biomechanics of all joints of the lower limb. Given the potential for adverse effects multiple joints with changing biomechanics—regardless of any beneficial loading outcome at the knee joint —clinicians must complete a thorough lower limb assessment when prescribing shoe-worn insoles to people with knee OA to minimise the potential for patient harm.
Dynamic joint loading with shoe-worn insoles
The KAM was the most commonly reported biomechanical outcome identified in this study, with all but one study19 reporting its changes with insoles use. This extends to recent systematic reviews of KAM calculation in gait studies in people with knee OA.20 The KAM may influence OA progression in a variety of ways; disease progression has been linked to (i) the overall peak magnitude (usually the early stance peak),1 (ii) the KAM impulse2 and (iii) external foot rotation—which is only affected by the late stance peak KAM.21 We found that LWIs produce similar, although small, reductions in the KAM, regardless of the discrete measure reported (SMDs ranging from −0.20 to −0.27; in addition to an SMD of −0.63 for the mean KAM, but with high heterogeneity). Given that Miyazaki et al found a 6.46 times increase in OA progression risk with an approximate 20% increase in overall peak KAM magnitudes,1 the 5%–10% reduction in KAM magnitudes typically observed with LWIs may be clinically important and aid in maintaining cartilage integrity. Even small reductions in the KAM may be beneficial over the long-term given that patients are encouraged to increase physical activity (eg, greater step counts) as part of guideline care.22 However, these potential biomechanical benefits have not yet been shown to translate to consistent clinical improvements in longitudinal studies of up to 2 years duration.4
What role does the foot and ankle play?
Recent studies have shifted focus to the changes at the ankle/subtalar joint. Although the available data on ankle/subtalar joint are still sparse compared with knee data, the findings are consistent. Specifically, while LWIs increase the amount of eversion as well as the subsequent external eversion moment, the addition of arch support to the medial aspect of the insole reduces the change in eversion and KAM. The design of LWIs promote more eversion throughout stance, and thus inclusion of material on the medial aspect likely dampens the mechanical effect of the lateral wedge.
The effect of increasing eversion on the ankle/subtalar joint is unclear, and caution must therefore be advocated when prescribing a device such as a lateral wedge, despite the positive effects on KAM magnitudes. For example, recent evidence has pointed to important links between foot biomechanics and knee OA characteristics. Individuals with knee OA exhibited more pronated feet than those without knee OA,23 and presence of foot and ankle pain increases the odds of developing symptoms and radiographic findings of knee OA.24 In the clinical setting, the maximum amount of ankle eversion that is tolerable to achieve meaningful KAM reductions should be determined. There is no research available to definitively answer this question; thus, determination should be considered on a case-by-case basis and will likely involve a number of small individual modifications to assess changes and optimise outcome.
Recent papers also suggest that foot type should be accounted for when studying and prescribing shoe-worn insoles.25 Furthermore, a recent study points to a potential role for increased eversion in the reduction of KAM magnitudes with LWIs. Chapman et al found that the amount of ankle/subtalar eversion was a significant predictor in who would achieve reductions in KAM values with the use of LWIs.8 While smaller KAM reductions may be achieved with lateral wedges plus arch support,16 26 preservation of normalised ankle biomechanics may be advantageous to prevent adverse effects at the ankle and/or foot. Given the obvious link between foot, ankle and knee biomechanics, it is suggested that future studies examining shoe-worn devices for the purposes of altering knee joint loads in people with knee OA measure and report foot and ankle biomechanical outcomes.
While changes at joints other than the knee, such as the ankle/subtalar joint, may be associated with changes in knee joint loading, there is potential for negative and unintended consequences at other joints. This is especially important given the small number of studies included in this review that included participant-reported adverse effects of the insoles. Only six studies reported measures of immediate comfort or adverse effects, and reports were generally of mild foot discomfort. However, some studies that incorporated a longitudinal design15 18 did report adverse effects or comfort throughout the intervention. As a result, it is suggested that future studies examining shoe-worn insoles in people with knee OA—both immediate and long-term—provide clinical measures of comfort and pain throughout the lower limb and back. These data are necessary to provide an indication of treatment safety before large-scale clinical implementation is undertaken.
Limitations
This review has limitations. First, we placed stringent inclusion and exclusion criteria on selected studies that reduced the total number of studies, which may have prevented data pooling for some variables. For example, we were only interested in studies that examined biomechanical changes in people with knee OA. There exists a number of studies that examine the effect of shoe-worn insoles on healthy individuals, and although the biomechanical responses may be similar, our aim was to summarise the biomechanical data in the target population (ie, knee OA) only. Second, we limited the analysis to studies that examined removable insole devices. This was done to increase generalisability and ecological validity to a wider potential target population. As a result, studies that examined specialised changes in shoe design such as variable stiffness insoles,27 or devices that attach to the bottom of specially made shoes (eg, Apos therapy28) were excluded. Third, there were inconsistencies in the design of the insoles between studies, and factors such as angulation of the lateral wedge, length of insoles and material properties may have increased variability in findings. In addition, no between-insole comparisons could be drawn due to the limited number of studies examining interventions other than LWIs. Finally, we placed no restrictions on compartmental involvement or disease severity. Thus, our findings may not be generalisable to all individuals with knee OA. Importantly, recent findings have shown that links between biomechanical outcomes such as the KAM and clinical outcomes such as pain may only exist in those with more severe disease.29 Unfortunately, the nature of our review and the available data did not permit a comparison of biomechanical changes among disease severities.
With the exception of a small reduction in KAM magnitudes with the use of LWIs, the available research regarding the effect of shoe-worn insoles on the majority of reported biomechanical variables shows negligible, conflicting or no evidence. Importantly, this review further highlights the lack of available data for the use of different types of shoe-worn insoles other than LWIs, and that few studies have considered biomechanical changes at areas other than the knee. Future research should further investigate how different types of shoe-worn insoles result in alterations throughout the kinematic chain, either in isolation or when combined into a single insole, as well as identifying subgroups who respond to different insole configurations. Importantly, research identifying clinically meaningful changes in biomechanical variables following interventions including shoe-worn insoles that are relevant to OA is needed.
What is already known and what are the new findings
Lateral wedge insoles reduce the external knee adduction moment—an important biomechanical outcome associated with knee osteoarthritis progression.
Lateral wedges also produce changes at the ankle and foot, such as increasing ankle eversion.
Addition of arch support to a lateral wedge normalises ankle and foot motion, but limits reductions in the knee adduction moment.
The consequences of increasing ankle eversion to maximise knee adduction moment reductions are presently unknown.
Research to better guide the prescription of shoe-worn insoles to optimise biomechanics throughout the entire kinematicchain should improve clinical outcomes.
References
Footnotes
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.