Article Text

Abstract
Objective Resistance training (RT) improves walking ability in persons with peripheral artery disease. We conducted a meta-analysis of randomised controlled trials (RCTs) investigating the effect of RT on peripheral artery disease (as measured by walking ability).
Design We included RCTs that investigated the effect of RT on treadmill and/or 6 min walk (6-MWT) distances. RT intensity was assessed according to the American College of Sports Medicine guidelines by 1 repetition maximum or rating of perceived exertion. Standardised mean (SMD) and mean differences (MD) were calculated using a random-effects inverse variance model. Heterogeneity and bias were assessed using RevMan V.5.3. Meta-regression and meta-analysis of variance were performed as moderator analyses.
Data sources Databases (Medline, Embase, Web of Science, Cinahl and Google Scholar) were searched until July 2018.
Results Fifteen trials isolated RT; 7 trials compared RT with aerobic exercise. We analysed 826 patients (n=363 completing RT), with a mean age of 67.1±3.8 years. Training ranged from low-high intensity, 2–7 times per week for 17±7 weeks, with a mix of upper, lower or whole body training. Overall RT significantly improved constant load treadmill claudication onset (COD) (SMD 0.66 [0.40, 0.93], p<0.00001) and total walking distance (WD) (SMD 0.51 [0.23, 0.79], p=0.0003), progressive treadmill COD (SMD 0.56 [0.00, 1.13], p=0.05) and total WD (SMD 0.45 [0.08, 0.83], p=0.02), and 6-MWT COD (MD 82.23 m [40.91, 123.54], p<0.0001). Intensity played a role in improvement, with high-intensity training yielding the greatest improvement (p=0.02).
Conclusions RT clinically improved treadmill and flat ground walking ability in persons with peripheral artery disease. Higher intensity training was associated with better outcomes. Our study makes a case for clinicians to include high-intensity lower body RT in the treatment of peripheral artery disease.
Trial registration number CRD42017081184.
- cardiovascular
- strength
- meta-analysis
- artery
Statistics from Altmetric.com
Introduction
Peripheral artery disease (PAD) is an atherosclerotic disease affecting the arteries of the periphery, most commonly the aorta and iliac arteries, and the arteries of the lower limbs, and it affects over 200 million people worldwide.1 Although some people may be asymptomatic, others may present with intermittent claudication symptoms. Claudication, a fatigue, cramp, discomfort or pain in the lower limb, is a symptom of reduced muscle blood supply.2 PAD eventually denervates the lower limb muscle fibres,3 which causes muscle weakness,4 5 atrophy6 7 and altered lower limb biomechanics.8–10 This limits walking ability and impairs quality of life in this population.
Current treatment guidelines for PAD recommend interval walking as the first-line therapy, along with other modes of aerobic exercise and resistance training (RT) as an adjunct treatment for the condition.2 11 In addition, some guidelines omit the mode of exercise and only provide prescriptive elements of supervision, frequency, duration and length of programme.12 While intermittent walking is an effective exercise prescription for people who can complete it, people with severe intermittent claudication may struggle to take part due to chronic diseases and conditions that limit the ability to walk or be physically active (e.g., chronic obstructive pulmonary disease, obesity, arthritis, amputation or cerebrovascular disease with stroke13). Furthermore, people with intermittent claudication have intense pain with walking.14 15 Some people have low confidence in their walking ability, and believe the pain induced by it can be harmful.14 16 These factors might lead to increased sedentary behaviour,17 accelerated functional decline,18 reduced aerobic capacity or cardiorespiratory fitness, and reduced muscle strength and endurance,4 19–21 all impairing walking ability further and ultimately reducing quality of life.22
Resistance Training does not typically cause claudication pain,23–27 and improves cardiovascular disease risk factors28–34 and aerobic capacity and attenuates functional decline, yet is typically recommended only as an adjunct to aerobic exercise for the treatment of PAD.2 35 Therefore, we conducted a systematic review and meta-analysis on randomised controlled trials (RCTs) using RT as an intervention for persons with PAD, with walking ability as an outcome. We aimed to identify whether or not RT is effective at improving walking ability in this population by analysing the effect of RT compared with usual care or aerobic exercise training on 6 min walk (6-MWT) distance and treadmill walking. Primary outcomes included claudication onset distance (COD) and total walking distance (WD) for all walking tests. We also aimed to identify whether there were any moderators associated with changes in walking ability. For the purpose of this review, RT included any structured body weight, machine and/or free weight-based RT where muscles contracted against some form of external resistance or immovable object/surface.
Methods
This review was registered with The International Prospective Register of Systematic Reviews (PROSPERO) on 8 December 2017.
Five electronic databases (Ovid Medline/PubMed, Scopus/Web of Science, Physiotherapy Evidence Database, Embase and Cochrane Library) were searched from the earliest record until July 2018. Search terms used include the following: (peripheral vascular or claudica* or peripheral arter*) AND (exer* or resist* or weightlifting or strength or musc* exercise or circuit or endurance) AND (random* or control*). One study author (BJP) ran the search and uploaded the search results into one EndNote database. After excluding duplicates one author (BJP) reviewed all titles and abstracts for possible inclusion. Any full papers that were retrieved for evaluation were then screened by two authors for inclusion (BJP and YM). Any disputes were settled by a third author (MFS). The reference lists of eligible papers were reviewed to identify other relevant studies, and recent related systematic reviews were consulted to identify any additional studies that may have been missed.
Studies were included if they were an RCT on any persons with diagnosed PAD who took part in an RT intervention for ≥4 weeks, with walking ability measured via treadmill protocols and/or the 6-MWT distance as an outcome. For the purpose of this review, muscular fitness was defined according to the American College of Sports Medicine (ACSM), where it is used as a collective term for muscular strength, power and endurance.36 Muscular fitness can be improved by a strength exercise training programme, where a movement is performed that causes the muscles to contract against an external resistance with the expectation of increases in strength, tone, mass and/or endurance.37 Equipment used can include free weights, machines with stacked weights, pneumatic resistance, resistance bands, springs or body weight. To be included in this review, RT must have included multijoint or compound exercises (e.g., chest press, shoulder press, pulldowns, rows, leg press, squats, deadlifts), or single joint exercises targeting major muscle groups (e.g., bicep curls, triceps extensions, quadriceps extensions, leg curls, calf raises). Studies that included exercises targeting the core muscles (e.g., planks, bridges) were also included. Training programmes could be circuit type in nature, where clear exercise:rest intervals were defined, or a more traditional form of RT, where reps and sets were completed without specified set time and recovery between sets was 2–3 min. To be labelled progressive, the resistance exercise must have been progressive by design, in that the absolute workload prescribed increased over time.37 The workload increase may have been achieved by greater forces used, number of exercises, volumes (sets/reps), frequencies of training, or relative intensities of the loads or maximal effort prescribed.
As there is a dose–response association between the volume of exercise and some outcomes,37 RT volume was defined using sets × repetitions × number of days per week.36 Intensity was also defined according to ACSM36 where:
≥85% of 1 repetition maximum (1RM) or rate of perceived exertion38 (RPE) ≥18 is very high, near maximal or maximal.
70%–84% of 1RM or RPE 14–17 is high.
50%–69% of 1RM or RPE 12–13 is moderate.
30%–49% 1RM or RPE 9–11 is light.
<30% 1RM or RPE <9 is very light.
To be included studies must have compared the intervention with the current unsupervised walking guidelines (usual medical care), or a supervised aerobic exercise training programme. Outcomes to be assessed included COD, defined as the moment in which claudication pain starts, and total WD, defined as the maximal WD obtained from a constant load and/or graded treadmill test and/or 6-MWT. A secondary outcome of muscle strength was assessed for trials that included this measure. Trials were excluded if they combined an RT intervention with an aerobic exercise intervention and the effects of RT could not be isolated; or if they were completed on animals; or not published in English in a peer-reviewed journal or thesis. Trials were also excluded if asymptomatic patients were grouped with symptomatic patients with PAD and the symptomatic patients were unable to be isolated. Data were extracted by one author (BJP) onto prepiloted data forms. Authors were contacted for missing data.
Risk of bias
Risk of bias of the included studies was assessed using the Cochrane Collaboration’s tool for assessing risk of bias. Eight domains of potential bias were assessed (online supplementary table 1): sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, complete outcome data, free of selective outcome reporting, baseline similarity, and intention to treat data analyses. Scores were summed across all eight domains to give a total score of risk bias for each study, with a possible range of 1–8. Studies with a higher score were deemed to be of higher quality and therefore lower risk of bias. However, rather than focusing on just the scores, the quality of each study was assessed by whether or not points were given for individual quality criterion. With randomisation already being a necessary criterion, studies that have points allocated for randomised sequence generation, allocation concealment, blinding of participants, blinding of outcome assessors and intention-to-treat analysis, and were free of any other bias were deemed higher quality and therefore lower risk of bias.
Supplemental material
Data extraction
WDs analysed were the mean difference (MD) between pregroup and postgroup data, if not reported MD was calculated by subtracting baseline from post values for both the control and intervention groups. Data required were the individual group sample size, mean change and SD or 95% CI of the change score, and/or within-group p value. When the CI or SD was not available, actual p values for preintervention/postintervention change were used. If only the level of significance was available, we used default p values where p<0.05 becomes p=0.049, p<0.001 becomes p=0.0099, and p=not significant becomes p=0.051. Values were taken from baseline measures, and then at the time-point closest to the end of the intervention period. For studies that contributed multiple comparisons (e.g., one control group and two interventions groups39), the control group data were evenly divided into two smaller groups.
Data synthesis
A narrative synthesis regarding participant characteristics and study interventions was completed. Aggregate data were used in the analyses to calculate the standardised mean response. However, RevMan V.5.3 (Nordic Cochrane Centre, Denmark) reports this as MD and 95% CI, which were calculated for the 6-MWT measures (reported in metres), and to account for any differences in testing protocols standardised mean (SMD) and 95% CI were calculated for the treadmill WD using the Cochrane RevMan calculator40 in RevMan V.5.3. MD was unable to be calculated for constant and progressive load treadmill protocols due to the difference in protocols used across trials (i.e., some constant load protocols ran at different speeds and/or grades to other constant load protocols, and vice versa for progressive grade protocols). If enough data were provided, then a quantitative synthesis was completed on each of the outcomes using an inverse variance, random-effects analysis. Both statistical and clinical meaningfulness of outcomes were characterised. Statistical significance of SMDs was inferred if the CIs did not cross zero. Clinical meaningfulness of the MDs were interpreted such that a 50 m improvement in 6-MWT distance was considered to be the lower threshold of a clinically important difference in this cohort,41 as this improvement is associated with a reduction in cardiovascular mortality.
Moderator analysis
The significance of any heterogeneity identified was examined using the Cochran’s Q (χ²) test with p<0.05 indicating significant heterogeneity. Interpretation of heterogeneity was based on Cochrane recommendations39 using Higgins I², with scores ranging from 0% to 100%. A cut-off of 40% was used to proceed to moderator analysis if three or more studies were present to help identify sources of heterogeneity in the overall meta-analysis. Potential moderators assessed included age, ankle brachial index, frequency, intensity, RT method, number and area of exercises, total repetitions, programme length, progression and study quality. Univariate meta-regression analyses were used to assess the influence of continuous variables such as frequency, length of intervention and duration of session on walking ability. Meta-analysis of variance was completed on categorical variables such as intensity or location of training. Meta-regression and meta-analysis of variance were completed with a random intercept, fixed slopes model using ‘Wilson’s SPSS macro42’ and SPSS Statistics for Windows V.24.0. For studies where both a graded treadmill protocol and constant grade protocol and below-knee and above-knee strength were completed and reported, effect sizes (ES) and study weighting were averaged, so both outcomes were represented in the meta-regression analysis. If inconsistency remained, it was decided that the random-effects model used accounted for any other differences between studies.
Reporting bias
If as according to Cochrane more than 10 studies were included in an outcome analysis, funnel plot symmetry was used to detect reporting bias.39 Funnel plots are provided in online supplementary file.
Results
Included studies
Overall, 18 studies met the inclusion criteria for this analysis.21 23–27 43–54 Fourteen studies compared RT with a control group of usual medical care. Seven studies compared RT with an aerobic exercise group,21 23 24 26 45 46 53 three of these also had a control group.23 24 26 Seventeen studies published or provided enough data to be included in the quantitative analysis (figure 1). Study quality and risk of bias are outlined in online supplementary table 1. On average, study quality was moderate, with most trials failing to blind outcome assessors in the trials, potentially leading to a detection bias, where there could be a difference between groups in how outcomes are determined.

PRISMA flow chart for study identification. PAD, peripheral artery disease; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomised controlled trial; RT, resistance training.
Participant characteristics
In total 826 participants were studied, with 363 completing an RT intervention. The mean age was 67.1±3.8 years (range 61–74), and on average 68% of participants studied were male. The mean ankle brachial index was 0.66±0.23 (range 0.54–0.75), indicating mild to moderate PAD. Cardiovascular risk factors such as body mass index, waist circumference and blood pressure were poorly reported across studies.
Intervention characteristics
The characteristics of the RT interventions are outlined in table 1. Programme length varied from 6 to 24 weeks (18±7 weeks). The average training frequency was three times per week. Six trials trained participants twice a week,21 45 47 48 52 53 one trial four times a week43 and one trial daily.51 Intensity ranged from light at 30% 1RM25 to high at 80% 1RM,25 55 and the number of different exercises performed ranged from 1 to 14 (7±4 exercises), while the number of sets for each type of exercises ranged from 1 to 3, when reported, with the most common number being 3. The number of repetitions per set when reported ranged from 6 to 15 (10±5 reps). Exercises involved the use of arms, legs and trunk in six studies,21 25 27 46–48 the upper limb only in one study26 and the lower limb in the remainder of the studies.23 24 43–45 49–54 One study focused only on the calf muscles, using plantar flexion as the chosen exercise.54 Nine trials reported using a circuit training protocol,43 44 47–52 54 while the remaining studies21 23–27 45 46 53 had participants complete 1–3 sets of 3–14 reps of dynamic exercise, with 2–3 min rest intervals between sets. Duration of exercise sessions ranged from 20 through to 60 min. Ten trials21 23–27 45 46 51 53 reported that the RT was progressed weekly during the exercise sessions; in the remaining trials progression was not reported. Out of the 18 trials, 822 24–28 47 54 reported that RT did not produce claudication pain, 8 trials25 44 45 49–51 reported mild pain, and 2 trials47 48 reported moderate pain.
Intervention characteristics
Effect of RT versus control/usual care condition
Claudication onset distance
In the eight studies25 44 47 48 50–52 54 measuring this outcome, RT led to a significant improvement in COD on a constant grade treadmill protocol: SMD 0.64 (0.38, 0.90), p<0.00001, with zero heterogeneity (I2=0%, p=0.57) (figure 2A).
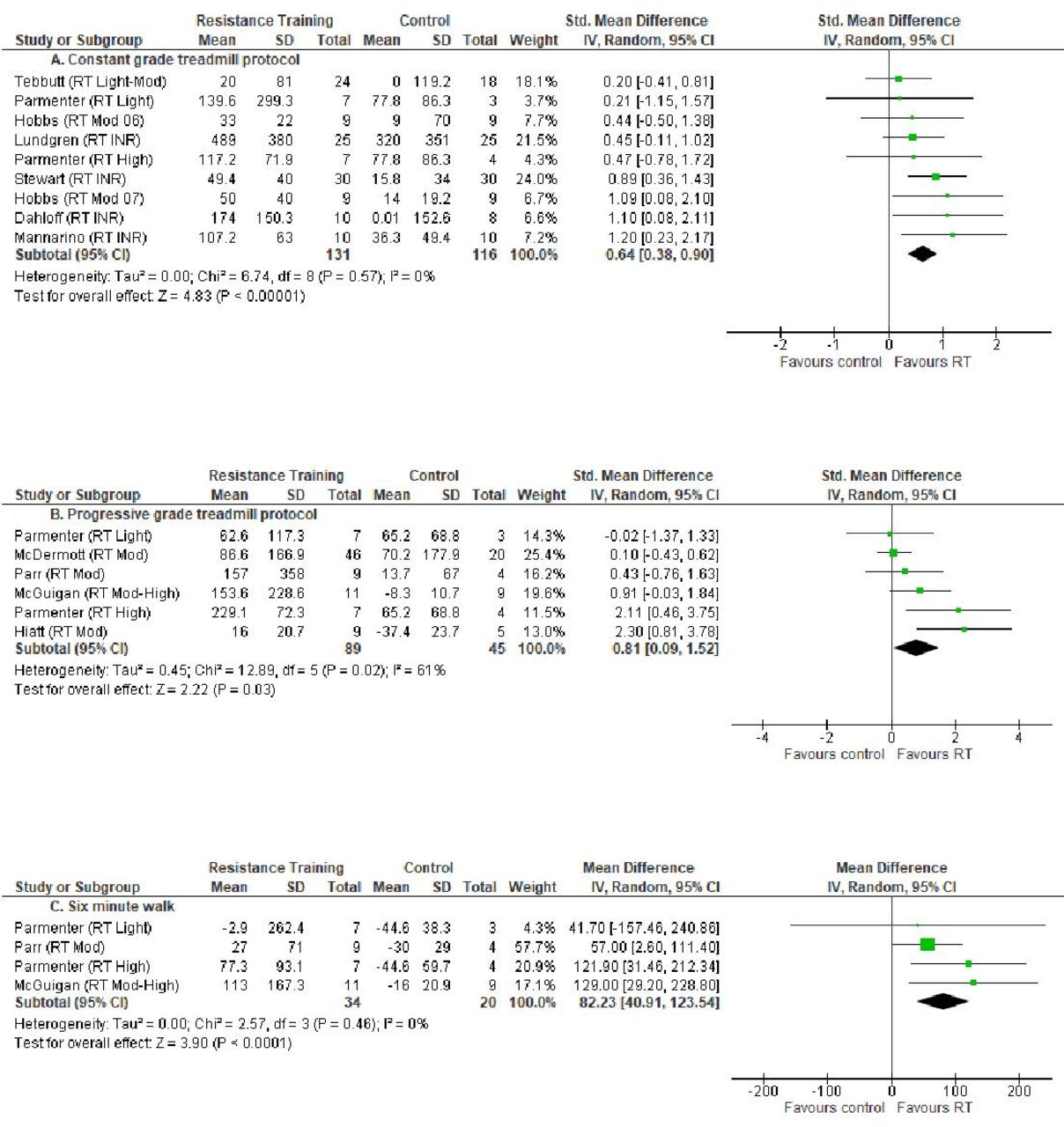
Claudication onset distance for (A) constant grade treadmill protocol; (B) progressive grade treadmill protocol; and (C) 6 min walk. CI, confidence interval; INR, intensity not reported; IV, inverse variance; Mod, moderate; RT, resistance training; SD, standard deviation of change.
In the five studies23–27 44 measuring this outcome (across six interventions), RT led to a significant improvement in COD on a progressive grade treadmill protocol: SMD 0.81 (0.09, 1.52), p=0.03; however, heterogeneity was substantial at I2=61% (p=0.02) (figure 2B). When only machine-based training studies (free weights excluded) were analysed, heterogeneity was reduced (I2=42%, p=0.14); however, the pooled effect was no longer significant: SMD 0.53 (−0.07, 1.13), p=0.08.
In the three studies25–27 44 that measured it (across four interventions), RT led to a clinically meaningful improvement in COD during the 6-MWT: MD 82.23 m (40.91, 123.54), p<0.0001, with zero heterogeneity (I2=0%, p=0.46) (figure 2C).
Total WD
Nine studies completed a constant grade treadmill protocol25 43 44 47 48 50–52 54 (across 10 interventions). In the studies that measured it, RT led to a significant improvement in WD in this protocol: SMD 0.48 (0.18, 0.78), p=0.002, with minimal heterogeneity (I2=33%, p=0.14) (figure 3A).

Total walking distance for (A) constant grade treadmill protocol; (B) progressive grade treadmill protocol; and (C) 6 min walk. CI, confidence interval; INR, intensity not reported; IV, inverse variance; Mod, moderate; RT, resistance training; SD, standard deviation of change.
Five studies23–27 used a progressive grade treadmill protocol. In these studies, RT led to a significant improvement in total WD: SMD 0.46 (0.09, 0.83), p=0.01, with zero heterogeneity (I2=0%, p=0.66) (figure 3B).
In the four studies that measured 6-MWT (across five interventions),24–27 RT did not significantly improve WD: MD 25.56 m (−3.12, 54.24), p=0.08, and there was minimal heterogeneity across studies (I2=34%, p=0.19) (figure 3C).
Effect of RT compared with walking training
Five studies21 23 24 46 53 compared RT with supervised treadmill walking training. There were only two studies45 53 that reported claudication onset during the 6-MWT; therefore, these data were unable to be combined and analysed. For 6-MWT distance, four studies reported enough data to be included in the analysis. Treadmill walking training was significantly better than RT; however, this difference was not clinically meaningful: MD −16.04 m (−27.48, –4.60), p=0.006 (I2=0%, p=0.68) (figure 4A).
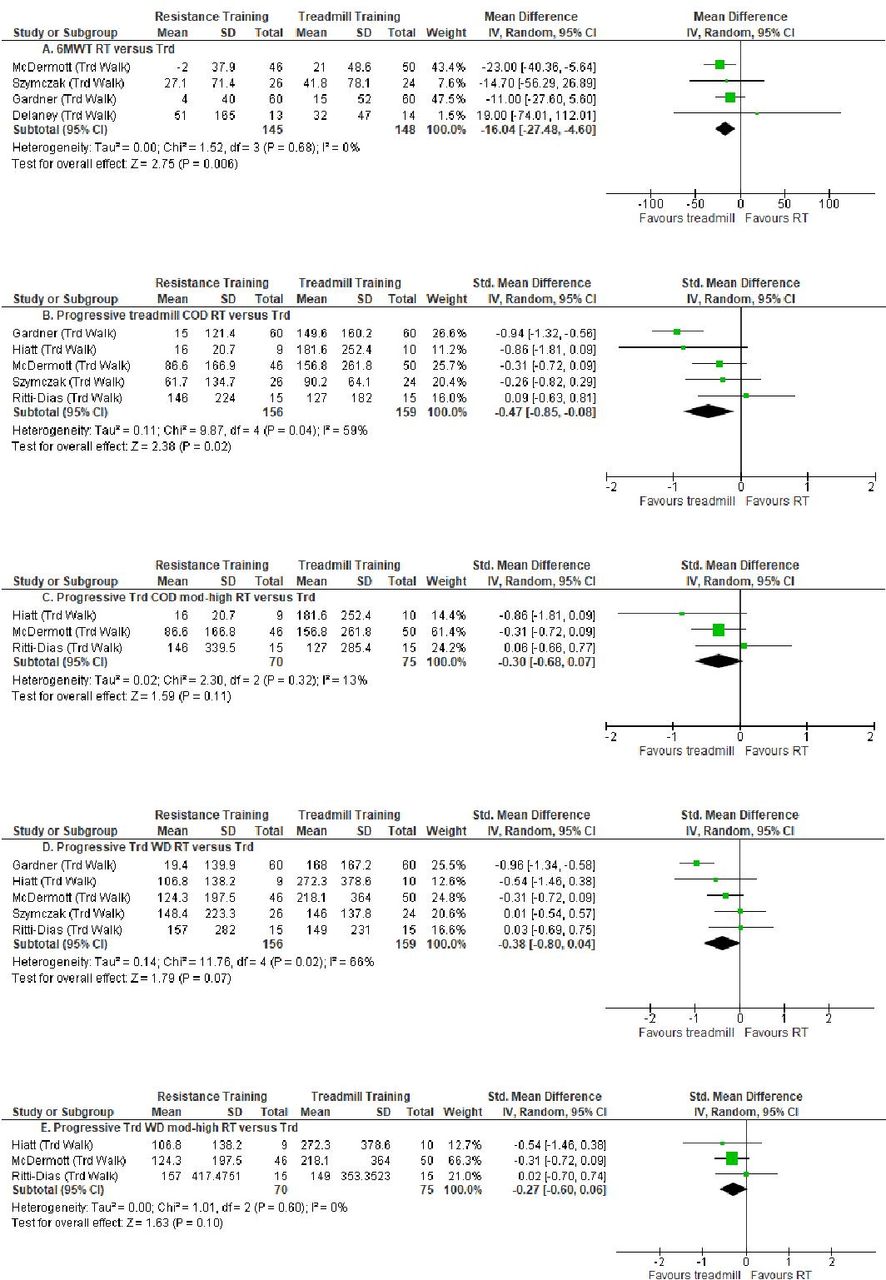
(A) 6-MWT distance for RT versus Trd training trials; (B) progressive treadmill COD RT versus Trd training; (C) progressive treadmill COD mod-high intensity RT versus Trd training; (D) progressive treadmill total WD RT versus Trd training; and (E) progressive treadmill total WD mod-high intensity RT versus Trd training. 6-MWT, 6 min walk; CI, confidence interval; COD, claudication onset distance; IV, inverse variance; Mod, moderate; RT, resistance training; SD, standard deviation of change; Trd, treadmill; WD, walking distance.
Five studies reported enough data to analyse progressive treadmill COD. Treadmill walking training was significantly better than RT: SMD −0.47 (−0.85, –0.08), p=0.02 (figure 4B). Notably, heterogeneity was moderate and significant at I2=59% (p=0.04). However, when high-intensity studies alone were analysed, the difference between WDs for treadmill COD was no longer significant and heterogeneity reduced substantially: progressive treadmill COD, SMD −0.30 (−0.68, 0.07), p=0.11 (I2=13%, p=0.32) (figure 4C).
Five studies reported enough data to analyse progressive treadmill total WD. Treadmill walking training was not significantly better than RT: SMD −0.38 (−0.80, 0.04), p=0.07 (figure 4D). However, heterogeneity was again moderate at I2=66% (p=0.02). When moderate-to-high intensity studies only were analysed, there was still no significant difference between treadmill training and RT, but heterogeneity was eliminated: SMD −0.27 (−0.60, 0.06), p=0.10 (I2=0%, p=0.60) (figure 4E). As there were only three studies, this result warrants further exploration.
Moderator analysis for identifying optimal exercise prescriptive elements
Effect of intensity of RT
Random-effects meta-analysis of variance results indicate that higher intensity RT leads to greater improvements in total WD (ẞ=0.53, p=0.03; high intensity (n=2) mean ES=0.66 (0.24, 1.07); moderate intensity (n=6) ES=0.46 (−0.25, 0.67); and low intensity (n=5) ES=−0.21 (−0.74, 0.29), with between-group p=0.02).
Effect of muscle groups trained
Random-effects meta-analysis of variance results indicate that lower body RT leads to a greater improvement in total WD (lower body mean ES=0.67 (0.39, 0.95); whole body mean ES=0.25 (-0.15, 0.65)). However, the between-group difference was not significant (p=0.09).
No statistically significant relationships with any other prescriptive elements or participant characteristics were identified.
Muscle strength testing
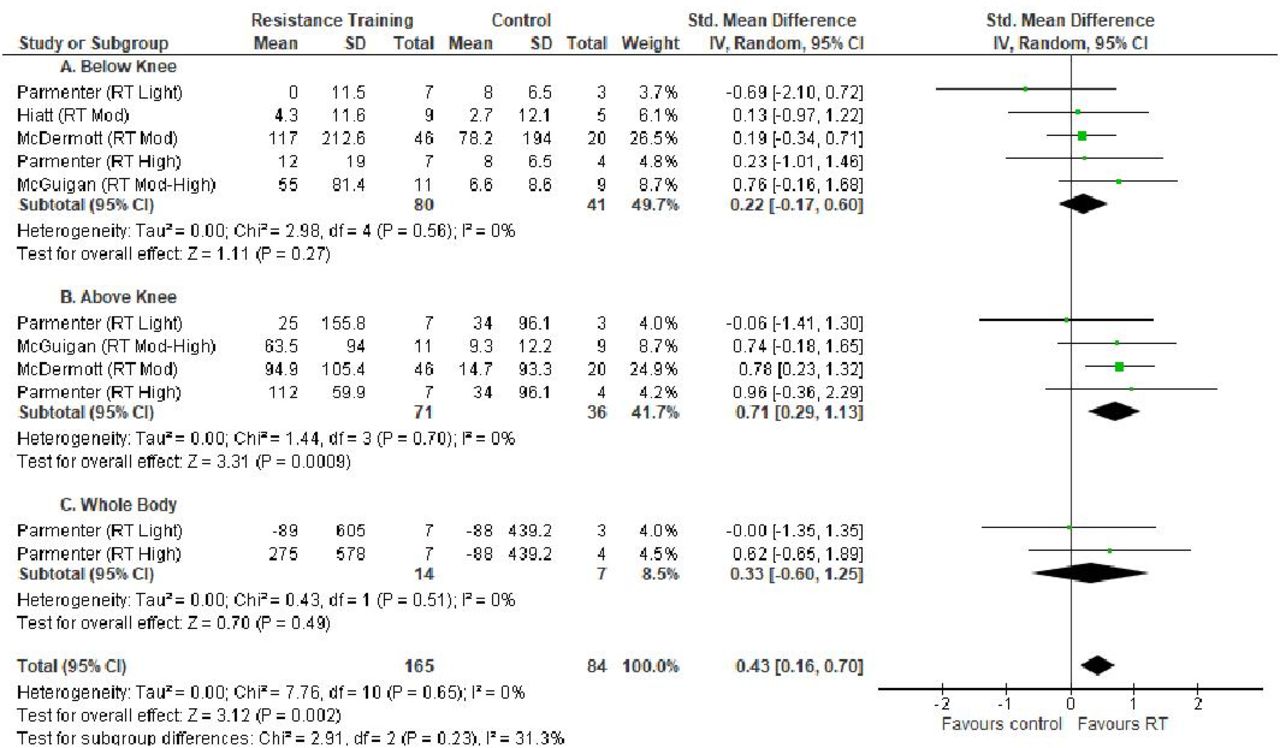
Although ten studies23–27 45 46 53 55 reported muscle strength as an outcome, only four23–25 27 reported enough information to be included in the analysis. All four studies used a version of RM testing. Two studies24 25 completed a 1RM with no adverse events, one study23 completed a 5RM on the calf muscles only, and the last study completed a 10RM. Overall RT improved muscle strength ES: SMD 0.43 (0.16, 0.70), p=0.002, with zero heterogeneity (I2=0%, p=0.65) (figure 5). Strength improved more robustly in the upper-leg/above-knee muscles of the claudicants, SMD 0.71 (0.29, 1.13), p=0.0009, and results were similar across trials (I2=0%, p=0.70).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in muscle strength across studies measuring (A) below-knee muscle strength; (B) above-knee muscle strength; and (C) whole body muscle strength. CI, confidence interval; IV, inverse variance; Mod, moderate; RT, resistance training; SD, standard deviation of change.
Risk of publication bias
The number of trials reaching 10 only occurred in two outcomes: constant grade treadmill total WD and change in overall muscle strength. Funnel plots for each of the analyses are presented in figures 1 and 2 of the online supplementary material. Funnel plots are symmetrical and do not indicate publication bias for either outcome.
Discussion
Patients with PAD have reduced leg strength and function.21 25 This study has shown that RT improves leg strength and both flat ground and graded WDs in persons with PAD. Furthermore, supervised RT programmes can also improve each of the individual risk factors for cardiovascular disease in older healthy adults.56 Trials of RT in persons with PAD therefore warrant further research to identify whether different prescriptions (ie, adjusting frequency and intensity) may be more effective in individual patients with PAD with varied cardiovascular risk profiles.
Effects of RT on walking capacity
This analysis has shown that RT alone improves walking ability for persons with PAD. The mechanisms underlying these effects have been explored in few studies. RT increases muscle mass27 and muscle strength,21 25 measures that are already reduced in patients with PAD.20 This meta-analysis included studies showing a strong association between changes in strength levels and changes in walking capacity after RT,21 25 suggesting that strength gains lead to greater muscle fibre recruitment during walking, thereby reducing the energy cost of walking. However, as only four studies included in this analysis reported strength testing results, it was difficult to explore this relationship.
Walking exercise has been recommended as the primary mode of exercise for patients with PAD. Therefore, the comparison of walking exercise against RT is useful to understand the effects of RT compared with this gold-standard mode of exercise for patients with PAD. This meta-analysis indicated superior effects of walking exercises compared with RT. However, when subgroup analyses were conducted, high-intensity RT produced similar increases in walking capacity assessed during a maximal graded treadmill test compared with walking training. Although we could not compare the effects of RT against walking training during the 6-MWT because there were too few studies, the similar effects of high-intensity RT compared with walking training assessed during graded treadmill tests suggest that high-intensity RT may be a feasible alternative therapy to walking for patients with PAD. This could help improve adherence of exercise programmes, given that patients have reported RT as being less painful than walking training.21
Elements of the most effective RT interventions and recommendations for future research
When we examined which elements of interventions were associated with large, significant improvements in walking ability, high-intensity RT of the lower body was the most effective element. Exercises focusing on the lower body—calf muscles, quadriceps, hamstrings and gluteals—were included in the interventions with the larger effects. Further comparisons of RT intensity would be better verified with direct comparisons (i.e., moderate 60% 1RM vs high-intensity [80% 1RM]) within trials. Only one study has done this to date,25 the results of which showed the ineffectiveness of low-intensity (30% 1RM) training against the efficacy of high-intensity (80% 1RM). Other elements of exercise prescription such as frequency of training sessions, length of programme, and whether whole body exercises are more beneficial than lower limb only remain unclear and need to be tested explicitly.
Limitations
Although poorly reported, some studies showed that the changes in WD were associated with changes in above-knee leg strength.21 25 The lack of strength testing of participants and/or lack of reporting testing results in the included trials is a major limitation of this literature. Future trials should ensure baseline strength measures are completed prior to commencement of strength training in order to ensure appropriate overload and progression is consistently applied to the training muscles. Furthermore, trials should report both the baseline and follow-up strength test results for individual muscle groups, along with changes in WDs so the relationship between leg strength and WDs can be explored further in future meta-analyses.
As cardiovascular risk is increased in this cohort, future trials should also report the effect of the exercise training on cardiovascular risk factors such as body mass index, waist circumference, arterial stiffness, inflammation and blood pressure. Research should also include more women and culturally and linguistically diverse cohorts. Outcomes should include measures of quality of life and physical function, such as balance, chair stand, gait speed and stair climb power, in order to identify RT prescriptions that are most efficacious at improving performance of activities of daily living. Finally, studies need to report and investigate more prescriptive elements of strength training, including the number of exercises, intensity and frequency of exercise training, and conduct longer follow-up testing in an effort to identify how long the effects of RT are maintained.
What is already known
Interval walking is the current gold standard treatment for peripheral artery disease (PAD).
Resistance training can improve walking ability in persons with PAD; there has been no previous synthesis of the literature.
What are the new findings
Resistance training improves both flat ground and graded treadmill walking ability in persons with PAD, by a clinically meaningful extent.
Better results were related to higher intensity training.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.