Article Text

Abstract
Objective Minority student-athletes have a lower survival rate from sudden cardiac arrest (SCA) than non-minority student-athletes. This study examined the relationship between high school indicators of socioeconomic status (SES) and survival in student-athletes with exercise-related SCA.
Methods High school student-athletes in the USA with exercise-related SCA on school campuses were prospectively identified from 1 July 2014 to 30 June 2018 by the National Center for Catastrophic Sports Injury Research. High school indicators of SES included the following: median household and family income, proportion of students on free/reduced lunch and percent minority students. Resuscitation details included witnessed arrest, presence of an athletic trainer, bystander cardiopulmonary resuscitation and use of an on-site automated external defibrillator (AED). The primary outcome was survival to hospital discharge. Differences in survival were analysed using risk ratios (RR) and univariate general log-binomial regression models.
Results Of 111 cases identified (mean age 15.8 years, 88% male, 49% white non-Hispanic), 75 (68%) survived. Minority student-athletes had a lower survival rate compared with white non-Hispanic student-athletes (51.1% vs 75.9%; RR 0.67, 95% CI 0.49 to 0.92). A non-significant monotonic increase in survival was observed with increasing median household or family income and with decreasing percent minority students or proportion on free/reduced lunch. The survival rate was 83% if an athletic trainer was on-site at the time of SCA and 85% if an on-site AED was used.
Conclusions Minority student-athletes with exercise-related SCA on high school campuses have lower survival rates than white non-Hispanic athletes, but this difference is not fully explained by SES markers of the school.
- resuscitation
- sports
- cardiovascular diseases
- defibrillators
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sudden cardiac arrest (SCA) in a child or adolescent is a tragic event with devastating impact to the family and local community. SCA affects >7000 youth in the USA annually and is the leading cause of exercise-related sudden death in young competitive athletes.1–4 A proportion of SCA in the young occurs on a school campus, with one systematic review reporting a SCA event in one per 24 –294 primary and secondary schools per year.5 SCA events in schools present a unique opportunity for targeted interventions through medical emergency response plans that improve outcomes and reduce the occurrence of sudden cardiac death (SCD). Guidelines from the American Heart Association and consensus recommendations on emergency preparedness and management of SCA in high school athletic programmes exist to guide proper emergency responses in schools.6 7 Current best practice recommendations for high schools recommend access to an automated external defibrillator (AED) within 3 min of collapse.8 SCA in schools is also more likely to be witnessed and receive bystander intervention.9 Indeed, recent studies indicate improved outcomes from SCA in middle schools and high schools largely due to wider training in cardiopulmonary resuscitation (CPR) and greater access to publicly available AEDs.10 11
In a 2018 study, we reported the overall survival from exercise-related SCA in young athletes was 48% across the USA.12 Importantly, 83% of athletes survived if an athletic trainer (AT) was on-site and involved in the resucitation, and 89% of athletes survived if an AED was on-site and used.12 However, racial differences in survival rates were found with 60% of white non-Hispanic athletes surviving SCA compared with 31% survival in minority athletes.12 We hypothesised that socioeconomic disparities, including reduced access to an AED or AT in schools, may contribute to lower survival rates in low-income communities with a greater proportion of minority students.12
The purpose of this study was to (1) define survival outcomes from exercise-related SCA in high school student-athletes, and (2) examine the relationship between SES indicators in high schools and survival from exercise-related SCA occurring in student-athletes on campus. Factors affecting SCA survival such as witnessed arrest, the presence of an AT, bystander CPR and use of an on-site AED were also analysed.
Methods
This study was conducted in collaboration with the National Center for Catastrophic Sports Injury Research (NCCSIR) and the UW Medicine Center for Sports Cardiology. The study was approved by the institutional review board at the University of North Carolina at Chapel Hill.
Case collection
Cases of SCA and SCD in young athletes participating in organised competitive sports in the USA were prospectively identified from 1 July 2014 to 30 June 2018 through an active surveillance programme led by the NCSSIR. This is an ongoing surveillance programme from which 2 years of survival data were previously reported.12 This study includes a 4-year dataset which allows a more robust survival analysis and the additional investigation of the relationship of school socioeconomic factors and survival.
Case identification methods included a systematic search of traditional and social media sources; reporting directly to the NCCSIR or UW Medicine Center for Sports Cardiology; direct communication with the National Federation of State High School Associations, state high school associations and National Athletic Trainers’ Association; and regular review of cases collected in the Parent Heart Watch database.
Attempts were made to collect additional information via phone interviews with family members, school representatives, ATs and coaches involved in the resuscitation and review of medical records and coroners and medical examiner reports in the event of autopsy. Outreach to family members and school representatives included 4–6 contact attempts by postal mail, email and/or phone over an 8-week period. Autopsy and medical records were gathered from public resources or through next-of-kin consent. All records were examined by a multidisciplinary panel, including experts in cardiovascular pathology, sports medicine and sports cardiology, to determine the underlying cause based on published criteria.4 12–15 All sources of information were used to classify race and ethnicity. If medical examiner or medical records or a surveillance report from the family or school staff were not available (n=57), media reports and athlete photos were used to determine race and ethnicity.
Inclusion and exclusion criteria
SCA was defined as an unexpected collapse due to a cardiac cause in which CPR and/or defibrillation was provided regardless of survival outcome.16 Cases occurring during exercise in which autopsy or medical records could not be obtained were included as cardiac in nature if the event details supported an abrupt collapse requiring cardiac resuscitation. Only exercise-related SCA cases in high school student-athletes that occurred on campus during school hours or during an organised athletic event (ie, practice or competition) were included. Cases of SCA occurring in a non-student or during a non-school-related activity outside of normal school hours were excluded.
School socioeconomic indicators
Demographic statistics and socioeconomic indicators were obtained for each high school with an SCA event. In cases during competition between two schools, the home high school’s demographic statistics and SES indicators were used. The school zip codes, school districts and public/private status of the schools were obtained from each school’s website. Median household and family incomes for the zip codes of the schools were obtained from the US Census Bureau’s American Community Survey 5-Year Estimates (available at census.gov).17 The years of the median household and family incomes were matched to the calendar year of incident in cases that occurred from 2014 to 2018. For cases that occurred in calendar year 2018, the 2017 incomes were used as this was the most up-to-date data available. Demographic information about the schools, including population, number of students on free/reduced lunch, enrollment by race/ethnicity and locale was acquired through the National Center for Education Statistics’ Elementary/Secondary Information System.18 The demographic and SES information of the schools was matched to the academic year (1 July–30 June) of the incident up to the 2016–2017 academic year. For cases that occurred during the 2017–2018 academic year, the 2016–2017 demographic information was used as this was the most up-to-date data available. The proportion of students on free/reduced lunch was only available for public schools. Details regarding schools’ employment of full-time or part-time ATs and the presence of AEDs on school campus were provided by the Korey Stringer Institute and the National Athletic Trainers’ Association Athletic Training Locations and Services (ATLAS) project.19 School AT employment was determined by the data available in ATLAS at the time of inquiry but did not allow matching to the precise year of the event.
Resuscitation details
Resuscitation details including witnessed arrest, presence of an AT, provision of bystander CPR, use of an on-site AED (AED on school campus or brought directly by AT) and use of a defibrillator provided by responding emergency medical services (EMS) were obtained by review of available media reports and phone interviews with school staff, families or survivors.9 14
Data analysis and statistics
The primary outcome was survival to hospital discharge following exercise-related SCA. Differences in survival based on minority status and SES indicator percentiles (lower 10th, middle 80th and upper 90th) were analysed using χ2 tests for the 2×3 tables. For statistically different 2×3 comparisons, post hoc pair-wise comparisons were performed with χ2 tests with Bonferroni adjustments. In all comparisons where expected cell counts were <1 or when >20% of cell counts were <5, a Fisher’s exact test was used instead. Descriptive analyses were used for resuscitation details. A Cochran-Armitage test for trend was performed to analyse the survival proportion over the four academic years included in the study period using a two-sided p value 0.05. The study period was also divided into the initial two academic years (2014/15 and 2015/16) vs the latter 2 years (2016/17 and 2017/18) to assess differences in overall survival and survival by minority status. A p value of<0.05 was considered statistically significant for all analyses.
Survival risk ratios (RR) and 95% CIs for exercise-related SCA survival (yes vs no) were calculated with univariate and multivariate modified Poisson regression with robust standard errors.19 Independent variables included the following: sex (female vs male), minority status (minority vs white non-Hispanic), academic year (indicator variable: 2015, 2016 and 2017 vs 2014), AT employment (binary variable: part-time or full-time AT vs none), and the four school-based SES indicator variables divided into percentiles (indicator variable: 10th and 90th vs the middle 80th percentiles for median household income, median family income, proportion free/reduced lunch and proportion student minority status). There were missing values for minority status (n=10), AT employment (n=4), proportion of students on free/reduced lunch (n=23), and proportion of student minority status (n=3) and univariate and multivariate models for those variables included only cases with non-missing values. 95% CIs that did not include 1.00 were considered statistically significant. Statistical analyses were performed using RStudio20 and SAS software.
Patient and public involvement
Patient and public involvement was not sought for design of this study, choice of outcome measures or dissemination of the results. The public could report an incident of catastrophic injury in an athlete through a public portal to the NCCSIR. Patient survivors and/or next-of-kin could provide additional information about a case via phone interview.
Results
Case demographics
A total of 215 SCA cases among high school student-athletes were captured over the 4-year study period. Of the 215 total cases, 168 were exercise-related, and of the exercise-related cases, 111 (66%) occurred on a school campus during normal school hours or during practice or competition (table 1). The mean student-athlete age was 15.8 years (range 13–18) with 88% of cases occurring in males. Fifty-four (49%) athletes were white non-Hispanic, 34 (31%) black/African American, 11 (10%) white Hispanic and 2 (2%) Asian. Race could not be determined in 10 athletes.
Demographic information for student-athletes with exercise-related sudden cardiac
Sixty-two (56%) cases occurred during practice and 33 (30%) occurred during competition. Cases occurring during a competition were more likely to survive (28/33; 85%) than cases occurring at practice (36/62; 58%) (χ2 7.03, p=0.008). Additional cases in student-athletes included eight (7%) cases during physical education class, three (3%) cases during recreational activities on campus during school hours, two (2%) cases during team-sanctioned strength and conditioning, two (2%) cases during a pick-up game and one (1%) case during an exercise/conditioning activity not sanctioned by the team.
Survival outcomes and school demographics
The overall survival was 68% (75 survivors, 36 deaths). Higher survival was observed in the latter two academic years of the study period compared with the earlier 2 years but the trend was not statistically significant (figure 1). Across the 4-year study period, minority athletes had a lower likelihood of surviving exercise-related SCA than white non-Hispanic athletes (24/47 (51%) vs 41/54 (76%); χ2 6.77, p=0.009; RR 0.67, 95% CI 0.49 to 0.92) (figure 2). When adjusting for covariates, while not statistically significant the effect size still suggests a meaningful difference (RR 0.76, 95% CI 0.52 to 1.13) (online supplemental table 1).
Supplemental material

Survival for exercise-related sudden cardiac arrest in student-athletes on high school campuses by academic year: 1 July 2014 to 30 June 2018 (n=111).
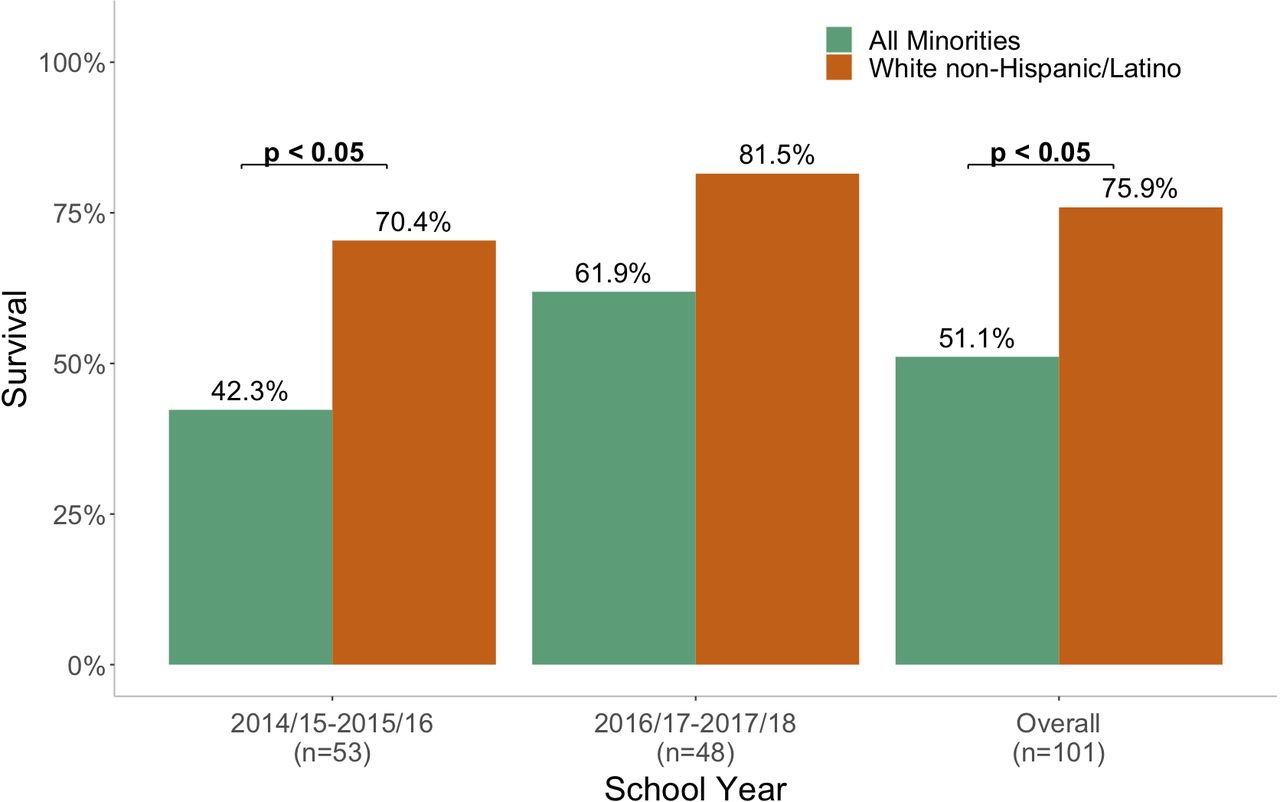
Survival for exercise-related sudden cardiac arrest in student-athletes on high school campuses by race: 1 July 2014 to 30 June 2018 (n=101). All comparisons not shown were non-significant.
The demographics of high schools where exercise-related SCA events occurred are shown in table 2. Eighty-nine (80%) cases occurred at public schools and 22 (20%) occurred at private schools. Survival was similar between cases that occurred at public (67%; 60/89) versus private (68%; 15/22) schools. Twenty-nine (26%) of the cases occurred in a city, 48 (43%) in a suburb, 15 (13%) in a town and 18 (16%) in a rural locale. There was no difference in survival based on the location of the school: city (69%), suburb (68.8%), town (66.7%) and rural (66.7%). Sixty-eight (61%) schools employed a full-time AT, 27 (24%) employed a part-time AT and 12 (11%) did not employ an AT. Cases occurring in schools that employed an AT (full-time or part-time) had a higher survival rate (71%; 67/95) than at schools that did not employ an AT (50%; 6/12), but the difference was not statistically significant (χ2 2.07, p=0.150) or when adjusting for covariates (RR 1.64, 95% CI 0.65 to 4.10) (online supplemental table 1).
Demographics of high schools with a case of exercise-related sudden cardiac arrest and death, 1 July 2014 to 30 June 2018
Survival by SES indicators
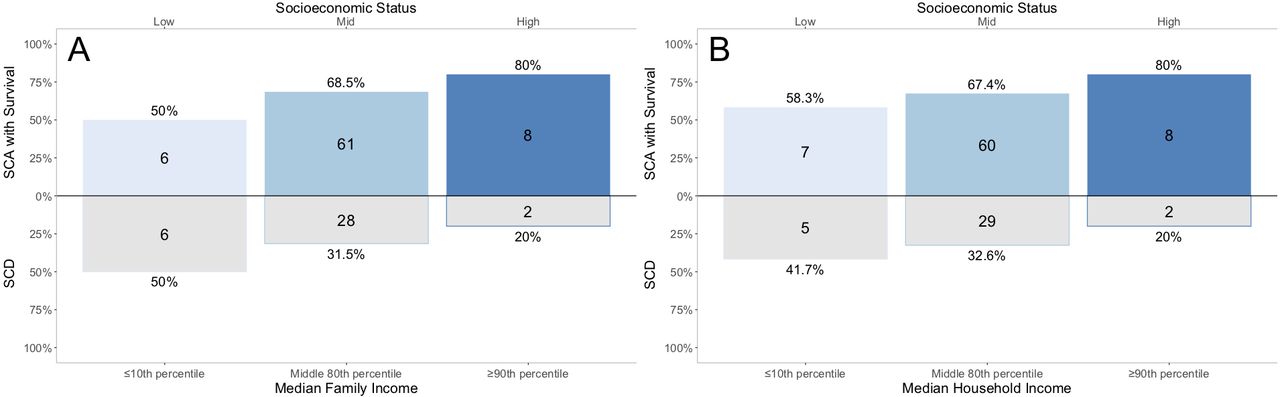
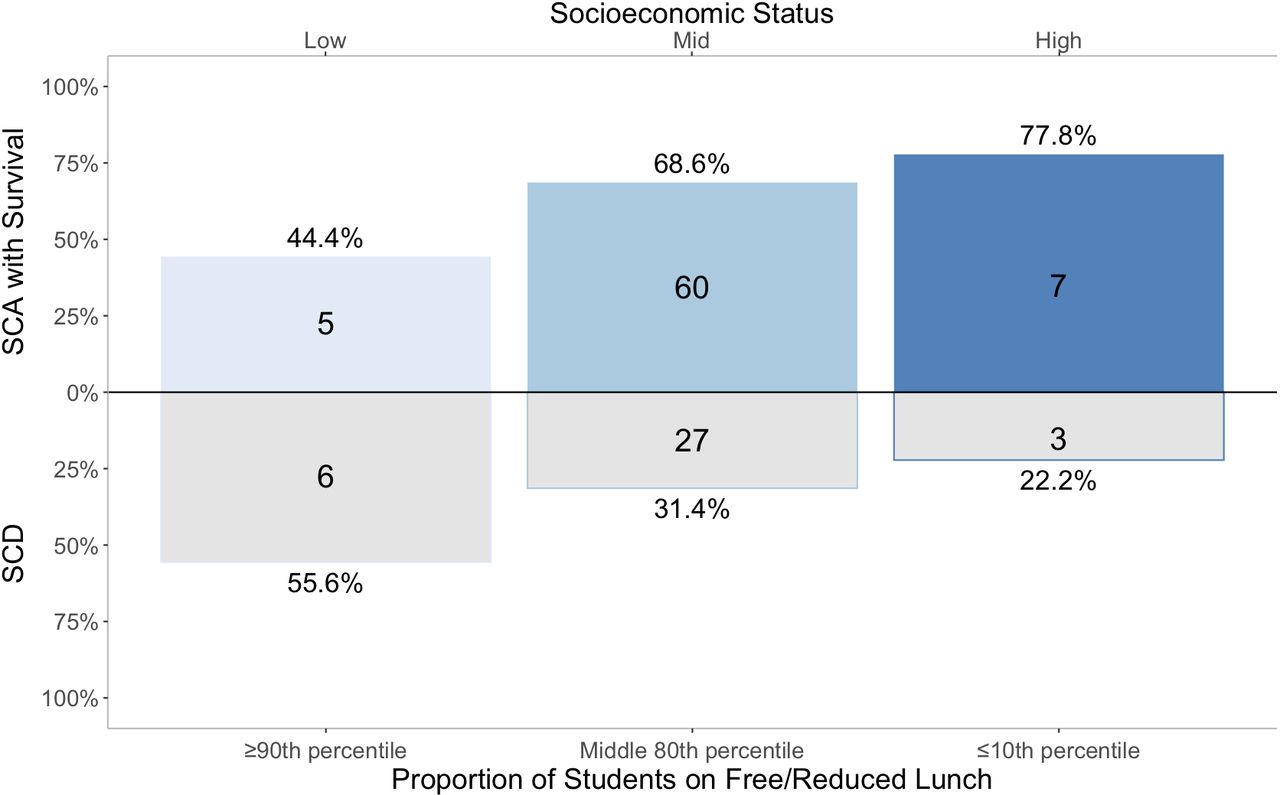
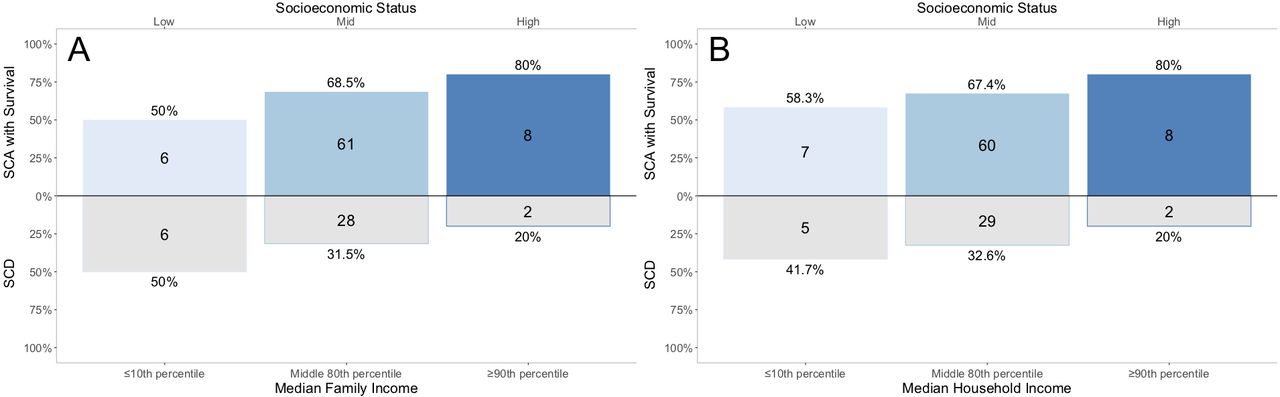
Survival according to minority status and SES indicator percentiles (lower 10th, middle 80th and upper 90th) are shown in figures 3–5.

Survival for exercise-related sudden cardiac arrest in student-athletes on high school campuses based on the proportion of minority students. High proportion: ≥90th percentile of minority students; mid-proportion: middle 80th percentile of minority students; low proportion: ≤10th percentile of minority students. SCA, sudden cardiac arrest; SCD, sudden cardiac death.

Survival for exercise-related sudden cardiac arrest in student-athletes on high school campuses based on the proportion of students on free/reduced lunch. Low SES: ≥90th percentile of students on free/reduced lunch; mid-SES: middle 80th percentile of students on free/reduced lunch; high SES: ≤10th percentile of students on free/reduced lunch. SCA, sudden cardiac arrest; SCD, sudden cardiac death; SES, socioeconomic status.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival for exercise-related sudden cardiac arrest in student-athletes on high school campuses based on median family or household income. (A) Survival based on median family income and (B) survival based on median household income. Low SES: ≤10th percentile of median family/household income; mid-SES: middle 80th percentile of median family/household income; high SES: ≥90th percentile of median family/household income. SCA, sudden cardiac arrest; SCD, sudden cardiac death; SES, socioeconomic status.
A summary of the univariate and multivariate analysis is shown in online supplemental table 1. A monotonic increase in survival was observed in univariate analyses with increasing median household or family income, but this trend attenuated when adjusting for covariates. A monotonic decrease in survival was observed in univariate analyses with increasing percent minority population or proportion of students on free/reduced lunch, but this trend also attenuated when adjusting for covariates.
Resuscitation details
Resuscitation and defibrillation details are shown in online supplemental table 2. The SCA event was witnessed in 107 (96%) cases. The administration of bystander CPR was confirmed in 88 (79%) cases and unknown in 23 (21%) cases. In cases where bystander CPR was performed, 80% (70/88) of athletes survived. An AT was on-site at the time of SCA in 46 (41%) cases, not on-site in 5 (5%) cases, and the presence of an AT on-site was unknown in 60 (54%) cases. In cases where an AT was confirmed on-site at the time of SCA, 83% (38/46) of athletes survived.
An on-site AED was available at 65 (59%) schools where the SCA event occurred and used in 61 (55%) of the total cases. If an on-site AED was used in the resuscitation, 85% (52/61) of cases survived. Information on defibrillator use by the responding EMS was difficult to obtain. Defibrillator use by EMS was confirmed in 14 cases with 9/14 (64%) surviving, not used in 29 cases in which an on-site AED was already used and the athlete survived, and unknown in 68 cases.
Discussion
We report a 68% survival rate in high school student-athletes with exercise-related SCA occurring on a school campus. Nationwide survival for EMS-treated children that suffer out-of-hospital cardiac arrest is approximately 8%.3 21 The higher survival rate found in this study is likely linked to the high proportion of cases that were witnessed and received prompt resuscitation. In a 2013 study of 2149 high schools in which 87% had a school-based AED programme, survival was 89% (16/18) in student-athletes with SCA during exercise.22 The larger sample size (n=111) in this study of exercise-related SCA and inclusion of all schools independent of their emergency preparedness provides more generalisable and encouraging results.
This is the first study to analyse the relationship between school SES indicators and survival outcomes from exercise-related SCA on US high school campuses. Our findings suggest an association between SES indicators of high schools and SCA survival that attenuated when adjusting for all covariates. Low SES communities and those with a higher minority population may be disproportionately affected by SCA and death.23–27 Across all age groups, studies report SCA rates are higher, but survival to hospital discharge is lower, in communities with a lower SES.23–27 For example, in New York City, black patients had twice the age-adjusted incidence of out-of-hospital cardiac arrest and nearly half the rate of age-adjusted survival of white patients, consistent with earlier research in Seattle and Chicago.28 ,29 ,30 When looking specifically at SCA in youth, counties with lower SES were shown to have a higher incidence of sudden death in the young.31 In 2018, a previous study using 2 years of the NCCSIR surveillance data reported lower survival from SCA in minority compared with white non-Hispanic athletes of all ages.12 In this study with a longer study period and a focus only on high school athletes, minority athletes also had lower survival from exercise-related SCA than white non-Hispanic athletes. Since SES factors did not fully account for these differences in survival, future studies should explore more details of school emergency response training as well as intrinsic factors such as the specific etiologies of SCA.
Disparities also exist in communities with low SES or a higher minority population in regard to emergency preparedness to respond to SCA. Among laypeople in the USA, there is a strong correlation between SES factors and the likelihood a layperson has received CPR training.32 A 2012 systematic review and meta-analysis identified that black patients were less likely to have a witnessed cardiac arrest, receive bystander CPR, and survive out-of-hospital cardiac arrest in the USA than white patients.33 A 2016 study identified that black and Asian patients were less likely to suffer a witnessed arrest or receive bystander CPR than white patients.34 In addition, patients that suffer out-of-hospital cardiac arrest in predominantly black neighbourhoods have lower rates of bystander CPR, AED use and survival than those in predominantly white neighbourhoods.35 36 When looking specifically at schools, disparities also exist in emergency preparedness. In Michigan, schools with more students eligible for free/reduced lunch or in lower SES counties were less likely to have cardiac emergency response plans in place and the number of AEDs per student varied inversely with the size of the minority student population.31 37 Although not directly investigated in this study, systemic or structural inequities in resources, training and emergency preparedness may exist in schools with a higher proportion of minority students and may explain in part the lower survival rate observed in minority student-athletes in this cohort. Further research is needed to understand racial/ethnic differences in outcomes from SCA in student-athletes.
Schools are in a unique position to implement targeted interventions that improve outcomes from SCA. In Japan, a nationwide survey determined that students that suffered out-of-hospital cardiac arrest in a school were more likely to be defibrillated by bystanders and had better overall outcomes than in other locations.9 In this study, 96% of exercise-related SCA events that occurred on high school campuses were witnessed, providing a critical opportunity for a prompt emergency response.
Current emergency health and safety best practice policy recommendations for high schools advise that all schools implement and practice an emergency action plan for SCA, provide CPR and AED education for anticipated responders, employ an AT that is available for practices/competitive events, and have well-maintained AEDs accessible within 3 min of collapse.6–8 Additionally, guidelines from the American Heart Association advise that high schools provide formal CPR education to all freshman and junior students.6 The cost for schools to purchase an AED, institute a medical emergency response plan, educate students in CPR, and institute a lay rescuer AED programme is estimated at US$7965 per school in the first year, with an annual cost of US$3065 in subsequent years.6 Although these costs may be difficult in schools with limited resources, implementation of these policies undoubtedly provides a foundation to improve survival from out-of-hospital cardiac arrest. Our study found that when bystander CPR was performed, 80% of student-athletes survived; when an on-site AED was used in the resuscitation, 85% of student-athletes survived; and when an AT was on-site and involved in the resuscitation, 83% of student-athletes survived.
Our study demonstrated a trend towards improved SCA survival in the latter 2 years of the study. When comparing the first 2 years to the final 2 years of the study, overall survival improved by 15%. Additionally, the minority status disparities in survival also appear to narrow in the latter 2 years of the study. Whereas there was a 28% difference in survival between white non-Hispanic athletes and minority athletes in the 2014/15–2015/16 academic years, this difference decreased to 20% in the 2016/17–2017/18 academic years. Although this narrowing of the survival gap between white non-Hispanic and minority students in more recent years is encouraging, there is undoubtedly still work to be done.
One avenue to close SES and racial disparities in SCA survival is through broader legislation and funding to ensure all high schools meet best practice recommendations for SCA preparedness. In the USA, the majority of states do not mandate the placement of AEDs in schools and even fewer provide adequate funding to cover the associated costs.38 In Washington, 82% of high schools without AEDs identified financial resources as either the first or second obstacle to acquiring an AED, with 60% of all schools with AEDs relying on donations to implement an AED programme.39 These findings present an opportunity for advocacy and increased legislation to improve SCA preparedness in schools. A 2017 study identified that state legislation in Connecticut led to an increase in AED prevalence among local high schools.40 In Oregon, high schools with an AT were both more likely to have an AED available and to implement venue-specific emergency action plans.41 high schools with AED programmes also are more likely to establish a comprehensive emergency action plan.42
Limitations
This study has limitations that should be acknowledged in the interpretation of results. First, there is no mandatory reporting system for SCA in high school student-athletes which may result in missing SCA cases in this study. However, this study used a national ongoing surveillance system for capture of SCA cases and the details about each event, as well as application of a rigorous, expert-informed adjudication process to evaluate all SCA cases. Second, acquisition of case details, medical records and autopsy reports is difficult and resulted in missing data regarding race and ethnicity and the details of the resuscitation. In cases where more explicit records were unavailable, media reports and athlete photos were used to determine race and ethnicity which may have been inaccurate. Although this study had a process in place to contact families and schools involved, in many cases family or school staff would not respond or were hesitant to provide information regarding the case. Third, with only 111 cases, power for some analyses were limited, and a longer study period is needed to better understand the relationship between school SES indicators and survival. Fourth, while AT employment information is continually updated in the ATLAS database, a potential mismatch in AT services and AED presence at the time of the SCA may have occurred as we were unable to match the ATLAS data to the precise year of the event. Fifth, Bonferroni is a conservative method for assessing differences and may miss significant differences. Similarly, using 95% CIs of the RR that exclude 1.00 (null value) to determine statistically significant differences may be overly conservative (ie, fail to reject the null when it should have been rejected).43 Finally, although the median household and family incomes and proportion of students on free/reduced lunch are useful indicators to estimate a school’s SES, they are not exact measurements of school resources. Investigation of other markers of SES and school resources such as the Area Deprivation Index, the Center for Disease Control’s Social Vulnerability Index, educational attainment, and the proportion of residents living below the poverty line should be considered in future studies.
Conclusion
This study demonstrates that exercise-related SCA in a student-athlete on a high school campus is largely a survivable event with prompt on-site resuscitation. However, minority student-athletes with exercise-related SCA have a lower survival rate than white non-Hispanic student-athletes, and this difference is not fully explained by markers of SES in the high schools. All SES indicators suggest a possible relationship between higher SES in schools and greater SCA survival. Wider advocacy, legislation, and funding aimed to increase emergency preparedness, the presence of AEDs, and AT employment in high schools may help narrow the disparities in SCA survival based on minority status and school SES factors.
What are the new findings?
From July 2014 to June 2018, the overall survival rate in US high school student-athletes with exercise-related sudden cardiac arrest (SCA) was 68%; survival rates were >80% if an athletic trainer was present or an on-site automated external defibrillator (AED) was used in the resuscitation.
Minority student-athletes with exercise-related SCA on high school campuses have lower survival rates than white non-Hispanic athletes (51.1% vs 75.9%; RR 0.67, 95% CI 0.49 to 0.92); this difference is not fully explained by socioeconomic factors of the schools.
How might it impact on clinical practice in the future?
Universal emergency preparedness for SCA with trained responders and access to an AED are strongly encouraged at all schools and athletic venues hosting competitive sport.
Wider advocacy, legislation and funding aimed to increase the presence of emergency action plans, AEDs and athletic trainer employment in high schools may help narrow disparities in SCA survival based on minority status or school socioeconomic factors.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
The authors acknowledge the support of the Korey Stringer Institute at the University of Connecticut and National Athletic Trainers’ Association, Athletic Training Locations and Services (ATLAS) Project, for this project. Conclusions drawn from or recommendations based on the data provided by the KSI and NATA are those of the author(s) and do not necessarily represent the official views of the KSI and the NATA.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rob_huggins_6, @DreznerJon
Contributors JS, KLK and JAD were responsible for the conception and design of the study, data acquisition and analysis, and drafting and revision of the manuscript. DFP and RAH were involved with data acquisition and analysis and provided critical revisions to the manuscript. All authors approve the final version and are accountable for all aspects of the work. JAD is the guarantor and responsible for the overall content.
Funding Supported by the National Center for Catastrophic Sports Injury Research (University of North Carolina at Chapel Hill), funded in part by the National Collegiate Athletic Association, the National Federation of State High School Associations, the American Football Coaches Association, the National Athletic Trainers’ Association, the National Operating Committee on Standards for Athletic Equipment and the American Medical Society for Sports Medicine. JS also received support from the University of Rochester School of Medicine and Dentistry, Research Training Program for his work on this study.
Competing interests JAD is editor-in-chief of BJSM.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.