Article Text

Statistics from Altmetric.com
See page 1589 for the question
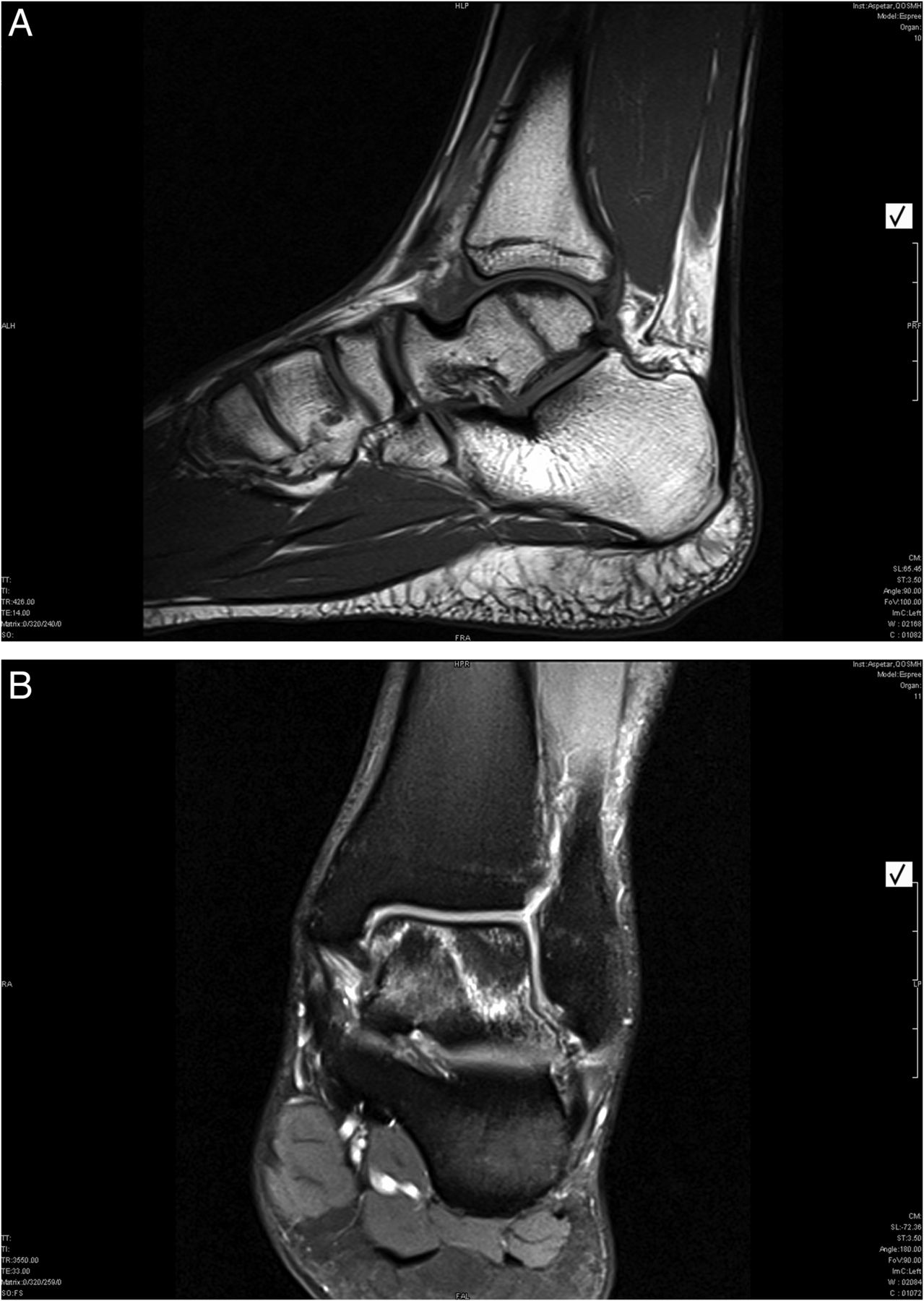
The MRI revealed progressive oedema in the fracture (figure 4A,B). Consequently, it was decided to perform an acute percutaneous internal compression fixation of the fracture by means of an Acutrak screw (figure 5). Since there was a progression of oedema along the fracture line—without real fracture diastasis—the authors chose a single compression screw fixation as the definitive treatment. Postoperatively, the patient was placed in an NWB cast for 2 weeks and a partial weight bearing walker boot for four more weeks. Physiotherapy was started after cast removal and full weight bearing was allowed starting from 6 weeks postoperatively. From the start of week 8 postoperatively, he started training individually with a progressive rehabilitation protocol for four more weeks. Three months postsurgery, he returned to the pitch playing at his preinjury level; he was pain-free and showing a full range of ankle motion.

Transtalar body fracture of the ankle with progressive oedema along the fracture line.

{kind=link}
{kind=link}
Percutaneous internal compression screw fixation of the talar body ankle fracture.
Discussion
Reports on stress fractures of the talar body are rare. Rossi et al1 found three stress fractures of the talar body in 24 562 clinical and radiographic skeletal records. More common, but still rare, are stress fractures of the talar neck or lateral talar process.2 ,3 Only one talar stress fracture without additional anomalies was reported in 1500 stress fractures.4 Stress fractures in athletes are the result of excessive, repetitive cyclic loads on bones that present with a normal form and structure. A stress fracture is considered to be the final stage of cellular events defined as prefailure stress bone response to strains.5 The aetiology is multifactorial, resulting from changes in the individual or athletic training material or programme. Malalignment, lack of flexibility, an increase in training, training of excessive volume and intensity, hard or soft activity surfaces, inappropriate shoes and inadequate coaching are the most usual intrinsic and extrinsic predisposing factors mentioned.1 Additional factors to be considered include age, sex, race, fitness, skill level and hormonal factors.6 The mechanical factors that may lead to a stress fracture remain unclear, but are thought to result either from repeated loading or from repetitive prolonged muscular actions on a bone that has not been conditioned to these heavy and new actions.
Stress fractures are the most common overuse injuries in athletes. Stress fractures of the talar body are extremely rare and have scarcely been described.1 ,7 Owing to the minor displacement, most stress fractures of the talar body (in athletes) are treated conservatively.1 ,8
In athletes, for example, football players, significant pathogenetic movements predisposing to a talar stress fracture can be identified in the repetitive restricted axial loading while sprinting, kicking the ball or landing after a heading attempt. The load that has to be absorbed during these actions created by the ground impact, the extremes in plantar/dorsiflexion of the foot (kicking the ball) and other traumatic actions should be considered as important pathogenetic factors in repetitive ankle injuries. Moreover, it has to be considered that playing at the end of a game, are coordinated less precise as the athlete is often fatigued.6 Diagnosis of stress fracture is based on clinical suspicion, a detailed history and a physical examination, followed by appropriate imaging investigations. The role of conventional radiography is important, although the initial findings are often minimal or absent. The earliest sign, always delayed to the onset of symptoms, may be a lucent linear image; more often, a sclerotic band or a periosteal reaction or callus formation is seen.1 ,6 In the presented case, the diagnosis was not considered by physical examination or by conventional X-rays but by MRI. This case can therefore also contain a message to the young and less experienced physicians not to miss these types of occult fractures. MRI has a high sensitivity to the detection of stress fractures. In addition, MR signs are evident several weeks before radiographic signs. In case of no or minor oedema/displacement at the fracture site, conservative treatment is preferred. There is limited literature on the duration of conservative treatment for stress fractures of the talar body. Stress fractures are known for their prolonged healing period.8 Generally, stress fractures are immobilised for 6–8 weeks.8 ,6 Studies on talar body stress fractures, however, advise a non-weight bearing casting period of 4 weeks.1 ,7 In the authors’ opinion, a non-weight bearing cast period of 2 weeks is preferred. After the immobilisation period, control images are made—preferably MRI—to check for positioning and fracture healing. In case of a satisfied progression, a weight-bearing cast/walker boot is applied after which the patient may gradually resume activity. However, as the vascularity of the talus is suboptimal, it is a relative high-risk location for avascular necrosis. Hawkins classified fractures of the talus to predict the risk of avascular necrosis. The described case can be classified as a Hawkins type 1 fracture. These fractures have a good prognosis as the risk of avascular necrosis is less than 15%. If significant displacement (Hawkins type 2) occurs (even secondary), the chance of avascular necrosis rises to 50% and surgical repositioning and fixation are indicated. As shown in the presented case, proper positioning can be achieved by means of a relative non-invasive intervention, meaning an arthroscopically assisted percutaneous internal fixation with an Acutrak screw. It is unknown how the oedema between the two talar particles progressed after the initial good alignment treated with cast immobilisation. A possible explanation for the increased oedema may lie in the prolonged immobilisation period, as this is known to increase osteopenia. Also, movement of the foot in the cast or walking with the cast could be a cause of oedema progression. In this case, however, the patient stated that he did not walk while wearing the cast and he was found to be compliant by his team staff. The cast was checked thoroughly for proper construction around the foot and leg. Hence, the question remains how the fracture has progressed secondarily. Overuse symptoms, metabolic alterations, lower limb malalignment and all other possible intrinsic and extrinsic factors were all considered as a cause, but it is still unclear why the stress fracture occurred and progressed at the rare location of the talar body. The trigger probably lies within the combination of factors considering the patient’s physical examination, radiological evaluation, skeletal/metabolic presentation and sports activity characteristics.
Since the aetiology of the case can be due to the repetitive stress on the ankle during athletic activities, there remains a possibility of recurrence whether it is treated conservatively or surgically. For this reason, it is advised that the compression screw should not be removed in this case, especially not before the end of the athlete's career.
A case report of a patient with secondary progression of a talar body stress fracture is presented. To our knowledge, a stress fracture of the talar body with secondary progression has not as yet been described.
Conclusion
This is the first report of a stress fracture of the talar body with secondary progression after initial conservative treatment. It is important to keep this in mind in case of a primarily undisplaced fracture which is treated conservatively, as apparently secondary progression—even in an immobilised patient—may occur. Through this case we argue the primary conservative treatment regimes that are being advocated in the literature. If a high-demand athlete presents with a talar body stress fracture—where you see oedema on the MRI T2 images and a visible fracture line on the MRI T1 images—rather than waiting initially, an immediate operative fixation is indicated. If adequate measures are taken with a quick intervention to fix the fracture progression, it is possible to achieve a good and time-efficient outcome without any remaining symptoms. The importance of this case is to alert the clinicians to the fact that talar body stress fractures in high-demand athletes—with a visible fracture line on MRI T1 images—need immediate operative fixation.
Footnotes
Correction notice This article has been corrected since it was published Online First. One of the authors' middle initials was omitted. It should appear as ‘J L Tol’.
Contributors JW was involved in collection of data, references and writing the draft. JT supervised the data acquisition. PL was involved in referral of the patient and assisted in writing the manuscript and follow-up of the patient.
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.