Article Text

Abstract
Identification, evaluation and management of disordered eating (DE) is complex. DE exists along the spectrum from optimised nutrition through to clinical eating disorders (EDs). Individual athletes can move back and forth along the spectrum of eating behaviour at any point in time over their career and within different stages of a training cycle. Athletes are more likely to present with DE than a clinical ED. Overall, there is a higher prevalence of DE and EDs in athletes compared with non-athletes. Additionally, athletes participating in aesthetic, gravitational and weight-class sports are at higher risk of DE and EDs than those in sports without these characteristics. The evaluation and management of DE requires a cohesive team of professional practitioners consisting of, at minimum, a doctor, a sports dietitian and a psychologist, termed within this statement as the core multidisciplinary team. The Australian Institute of Sport and the National Eating Disorders Collaboration have collaborated to provide this position statement, containing guidelines for athletes, coaches, support staff, clinicians and sporting organisations. The guidelines support the prevention and early identification of DE, and promote timely intervention to optimise nutrition for performance in a safe, supported, purposeful and individualised manner. This position statement is a call to action to all involved in sport to be aware of poor self-image and poor body image among athletes. The practical recommendations should guide the clinical management of DE in high performance sport.
- eating disorder
- athlete
- position statement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Introduction
The Australian Institute of Sport (AIS) is Australia’s peak high performance sport agency. The National Eating Disorders Collaboration (NEDC), an initiative of the Australian Government Department of Health, promotes nationally consistent, evidence-based responses to disordered eating (DE) and eating disorders (EDs) in Australia. Both organisations are committed to ensuring the safety and welfare of all high performance athletes. A high performance athlete is considered to be any athlete within the performance pathway ranging from junior and senior elite level and including para and able-bodied athletes. From here on, the high performance athlete will be referred to as the athlete.
The AIS and NEDC have collaborated to provide these guidelines for athletes, coaches, support staff, clinicians and sporting organisations. The guidelines support the prevention and recognition of DE, and promote early intervention to optimise nutrition for performance in a safe, supported, purposeful and individualised manner. This position statement is a call to action to all involved in sport to be aware of poor self-image and poor body image among athletes. Sporting organisations should develop sport-specific positions and guidelines that foster a healthy sport system for athletes. The practical recommendations in this document are intended to guide the clinical management of DE in high performance sport, putting in place a core multidisciplinary team (CMT) comprised of the doctor, sports dietitian and psychologist. The clinical treatment and management of EDs is outside the scope of this document. There are further resources available in the National Practice Standards for Eating Disorders,1 the Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of EDs (2014)2 and the UK National Institute for Health and Care Excellence guideline on EDs recognition and treatment (2017).3 In addition, the Australia and New Zealand Academy for EDs is due to publish Clinical Practice and Training Standards in 2020.
DE in athletes
DE in an athlete sits on a spectrum between optimised nutrition and an ED (figure 1). An individual with DE may regularly engage in behaviours such as skipping meals, compulsive eating, compulsive exercise and/or restrictive eating but without fully meeting the criteria for an ED. Comparisons between EDs and DE are shown in table 1. DE may involve short-term restrictive diets, which progress to chronic energy or nutrient restriction, binge eating, active and passive dehydration, use of laxatives, diuretics, vomiting, and diet pills with or without excessive training. Individual athletes can move back and forth along the spectrum of eating behaviour at any point in time over their career and within different stages of a training cycle (eg, during the off-season, preseason, when injured). Athletes are more likely to present with DE than a clinical ED.4–6 However, there are health and performance implications regardless of where an athlete falls along the spectrum and risks increase when DE worsens into a diagnosed ED.
Characteristics of eating disorders versus disordered eating in elite athletes (reprinted with permission from The IOC Consensus Statement on Mental Health in Elite Sport5)

The spectrum of eating behaviour in the high performance athlete from optimised nutrition to disordered eating to eating disorders. DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
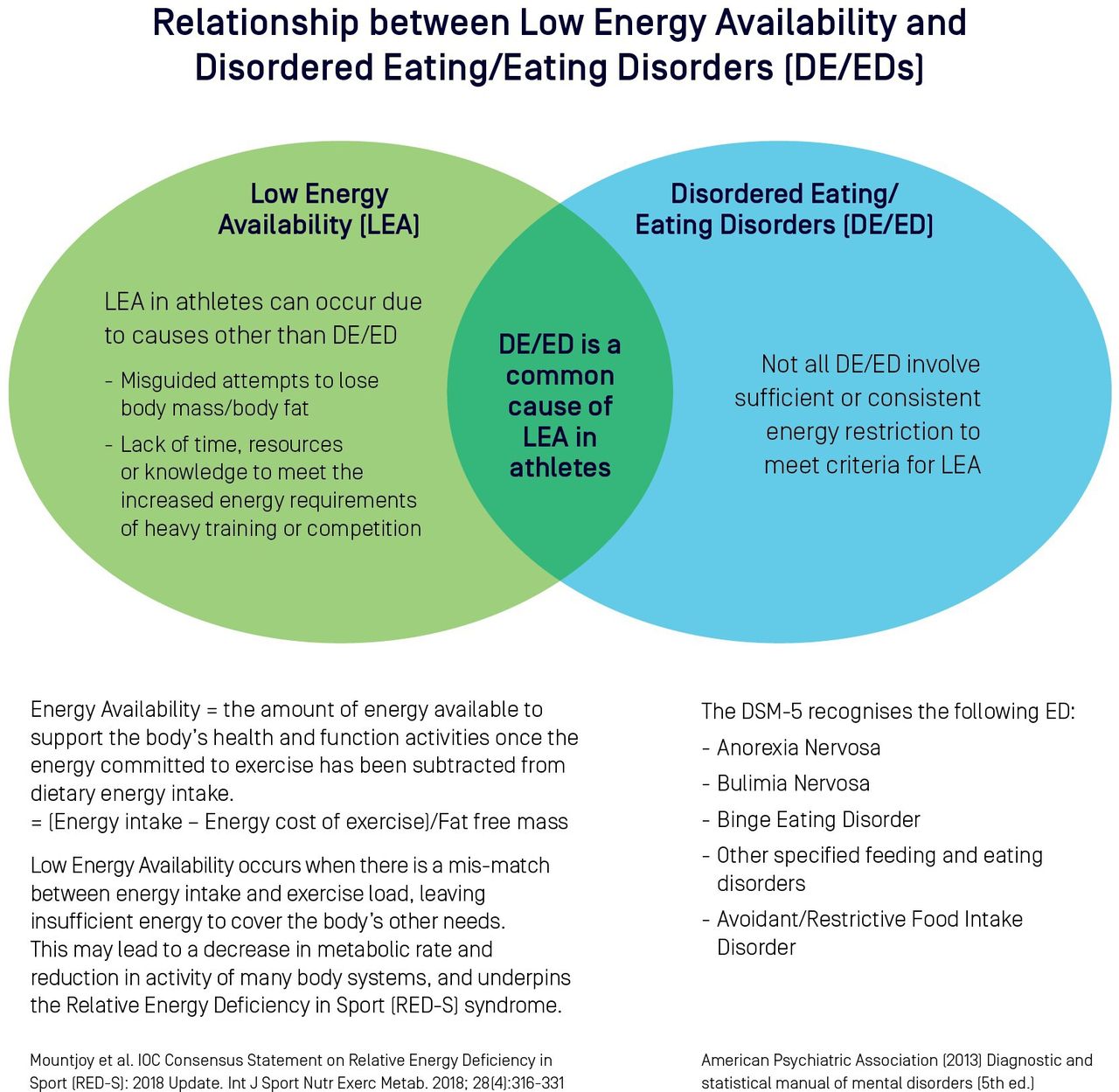
DE and low energy availability (LEA) can occur together, or in isolation (figure 2). Identification of one necessitates the investigation of the other. LEA may be difficult to recognise since an athlete may be stable in weight but deficient in energy.7 8 Added complexity in working with athletes comes from sport-specific pressures and individual comorbidities as well as cultural, familial, individual and genetic/biochemical factors.9

Eating disorders/disordered eating can occur in the absence or presence of low energy availability (adapted from Mountjoy et al)10 78. DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Health and performance consequences of DE behaviours
In addressing the health and performance consequences of DE or EDs, health must be the priority. One of the health risks of DE or EDs is the potential development of relative energy deficiency in sport (RED-S).10 In addition to the direct impairment of physiological and psychological function, DE can increase the risk of illness and injury, compromise training quality and consistency, and indirectly interfere with competition goals.9 Consequences of DE behaviours may include electrolyte imbalances, dehydration, nutritional deficiencies, gastrointestinal problems (dental, gingival, bleeding, ulceration, bloating, constipation) and mental health issues (depression, anxiety, personality disorders, substance abuse, self-harm and suicidal ideation).11 If DE is in conjunction with LEA, there may be suppression of physiological processes, resulting in impairments of bone health, menstrual function, endocrine, metabolic and haematological status, growth and development, psychological well-being, and cardiovascular, gastrointestinal and immunological systems.9 12 The long-term consequences of LEA are particularly critical to the adolescent athlete, affecting the accrual of peak bone mineral density (BMD) and stature, and neurological13 and reproductive system development.7
Performance consequences of DE may arise from interrupted or less effective training (eg, increased illness and injury, reductions in training capacity, recovery and adaptation) as well as acute impairments on competition day from inadequate fuelling for the event (eg, reduction in coordination, concentration, mood, strength and endurance).9
Prevalence and contributing factors to DE in athletes
DE can occur in any athlete, in any sport, at any time, crossing boundaries of gender, age, body size, culture, socioeconomic background, athletic calibre and ability. The estimated prevalence of DE and/or EDs in athletes ranges from 0% to 19% in men and 6% to 45% in women.5 Overall, there is a higher prevalence of DE and EDs in athletes compared with non-athletes14 but sport-specific demands and individual characteristics of the athlete lead to a wide variation in prevalence of DE and EDs across different sports.12 Much of the prevalence data regarding DE in athletes originates from studies of Scandinavian cohorts and North American collegiate athletes, predominantly featuring Caucasian and able-bodied populations.10 15 There is a paucity of prevalence data in para-athletes with further research and understanding required to adequately address and inform best practice in this population.15 An environment in which there is pressure to either lose or gain weight and/or to maintain meticulous control of body composition may contribute to an increased prevalence of DE and EDs. Athletes may be underweight, normal weight or overweight, irrespective of DE or EDs.15 16 Personal attributes which underpin successful performance, combined with the sport environment may leave athletes vulnerable to DE. Three categories of sports, defined as aesthetically judged, gravitational and weight class, are consistently identified as high risk for the development of DE and EDs.7 Risk factors for DE and EDs in high performance athletes are shown in table 2.
Suggested risk factors for disordered eating and eating disorders in high performance athletes4 10 14 17 18
Early identification, assessment and monitoring
Early identification of DE
DE in athletes can occur at any time; both precipitating, or being precipitated by, challenges in the athlete’s life as well as occurring during a time of successful performance.14 While there is a growing openness and support for mental health concerns in elite sport,16 barriers to early identification and treatment of DE and EDs still exist.4 5 19 Athletes’ shame, stigma and fear of discrimination prevent them from disclosing problematic behaviour and seeking help, whereas limited knowledge about ED symptoms and reluctance to ask specifically about eating problems inhibit providers’ detection of DE and EDs.20 It is widely accepted that the early identification and appropriate management of DE leads to better outcomes.21 EDs have one of the highest mortality rates among all mental illnesses, which underscores the importance of prevention efforts, timely detection and specialised treatment.22
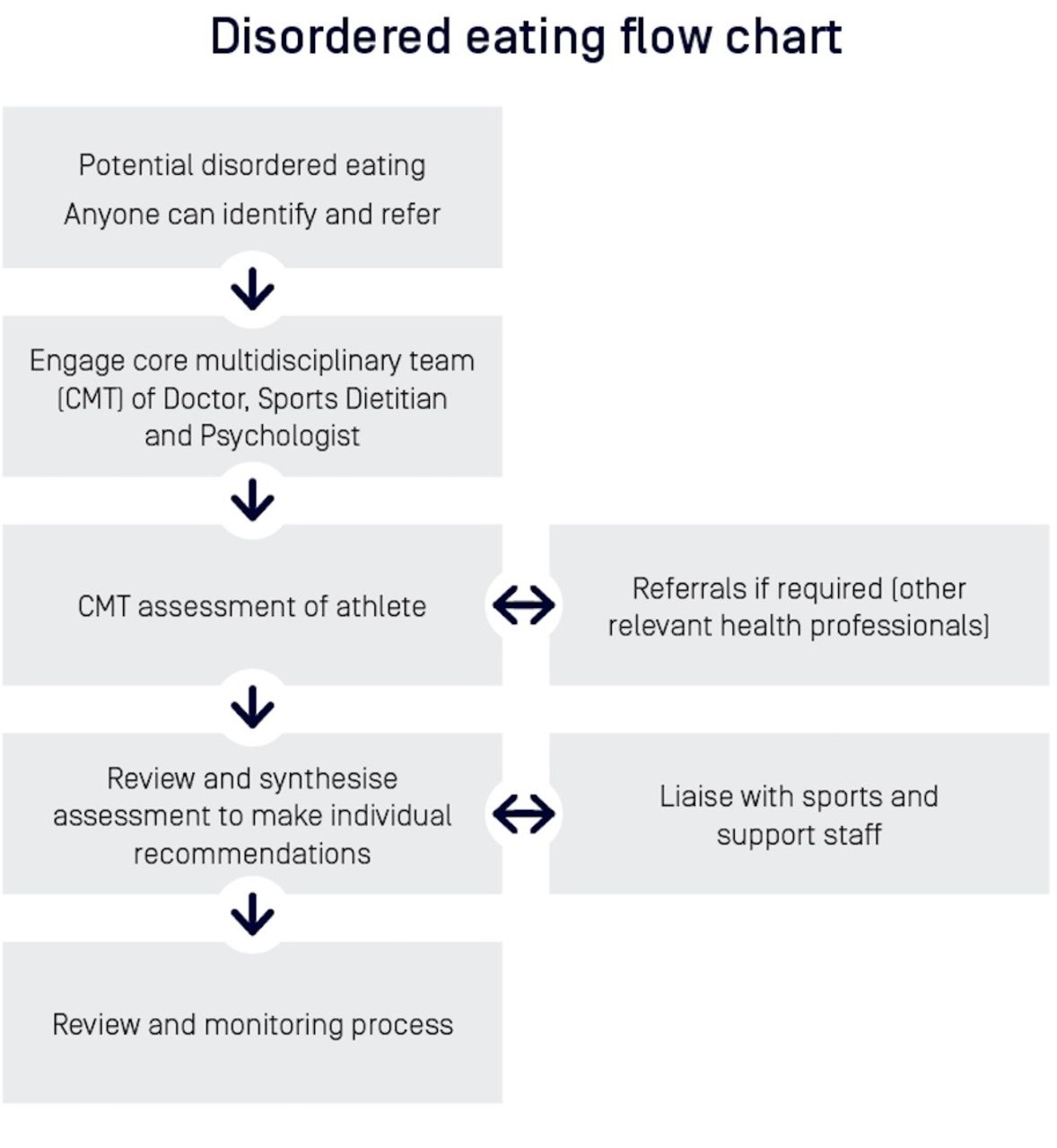
Everyone in the sport system has a role to play in recognition and early intervention, and anyone can refer athletes to, and/or consult with, any member of the CMT (doctor, sports dietitian and psychologist) for further assessment and support.11 It is important for all personnel involved in the sport to be aware of the risk factors and warning signs or red flags of DE and EDs (tables 2 and 3). Personnel should also be informed of effective communication channels for concerns. Some warning signs (table 3) can occur early (behavioural changes) whereas others such as weight changes may occur later in the person’s trajectory of DE.
Warning signs or red flags for disordered eating and eating disorders in athletes4 10 14 17 18
The CMT
The recommended CMT is comprised of the doctor, sports dietitian and psychologist, and together they coordinate the prevention, assessment, management and maintenance care in possible DE cases. As per the Olympic Movement Medical Code, all activities of the CMT should be based on the premise that the health and the welfare of athletes are pre-eminent and prevail over competitive, economic, legal or political considerations.23 Each member of the CMT provides expertise in a mutually supportive manner (figure 3) to deliver optimal care for the athlete in a safe, supported, individualised and purposeful way, governed by the ethos, ‘do no harm’. Doctors, sports dietitians and psychologists working within sport, despite not always self-identifying as experts in this field, need to have an awareness of DE and EDs and regularly seek professional development in this area.

Core multidisciplinary team management by a doctor, sports dietitian and psychologist: the core multidisciplinary team drives the assessment for disordered eating of an athlete, which may involve some overlap between disciplines depending on the trigger for recognition of disordered eating and the individual case characteristics. BMD, bone mineral density; DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; DXA, dual-energy X-ray absorptiometry
The CMT works with the athlete, coach and support staff to investigate and manage health, performance and return to play (RTP) considerations. With the athlete’s permission and respecting patient confidentiality, the ideal management model includes regular and collaborative communication between the CMT and coach. Further input may be sought from a range of specialists including an endocrinologist, gynaecologist, psychiatrist, sport scientist, physiotherapist, occupational therapist, social worker, paediatrician and/or specialist ED service (figure 4).7 21 The CMT is responsible for ensuring continuity of care. This includes effective collaboration between physical and mental health services, private and public health services, sport and community-based services and between professional disciplines.1 It is crucial that there are well-defined roles and a clear communication strategy within the CMT and across relevant stakeholders. A designated member of the CMT should ideally coordinate the flow of information across the team and with relevant sports staff.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disordered eating flow chart: recognition of disordered eating and referral of an athlete for assessment and management, primarily by the core multidisciplinary team within the context of a healthy sport system.
Assessment of DE in athletes
Clinical judgement and an understanding of the high performance sport context is crucial in distinguishing acceptable from problematic behaviours. Warning signs in the general population may be masked within the sporting environment. For example, a disciplined training diet and preoccupation with body weight and shape may reflect a specific sport culture, changes in, or absolutely low, levels of body fat may be balanced by muscle to present an acceptable body weight, and excessive exercise is easily hidden by demanding training programmes.24 25 Although a number of tools have been developed to screen for DE and EDs in the general population, validated and specialised tools for use in sport across varied athlete populations are limited in number and quality.17 26 27 Current recommendations for DE assessment include using self-report screening tools followed by an interview-based assessment, and sport-specific versus general approaches where available.4 5 Whenever feasible, and with the athlete’s permission, assessment may involve interviewing others in the athlete’s support network, including coaches, teammates, family and friends.
Screening tools and questionnaires
There are a range of screening tools and questionnaires available to assist the assessment of DE in athletes. The Eating Disorder Examination 17.0 (EDE 17.0) is currently regarded as the gold standard for clinical interview for diagnostic purposes of EDs in the general population.28 29 The Eating Disorder Examination Questionnaire 6.0 (EDE-Q 6.0) is a short form screening tool based on the EDE 17.0 and is acceptable for use in practice. The EDE-Q 6.0 should form part of a comprehensive assessment of the athlete. Additional tools including the Athletic Milieu Direct Questionnaire Version 2 and Physiological Screening Test, the Brief Eating Disorder in Athletes Questionnaire Version 2, and the Eating Attitudes Test-26; all provide discrimination between athletes with and without EDs.27 29–32 However, there are several limitations of these tools for EDs, particularly for male athletes, and care should be taken to ensure the tool is appropriate for the athlete.33
The assessment of LEA in athletes is also problematic since a quantitative assessment of EA is time-consuming and marred by errors of reliability and validity in calculating its main components (energy intake and exercise energy expenditure).8 The assessment of EA is complicated by errors in the measurement of its component parts and failure to account for other factors such as dietary quality and within-day energy spread.8 The Low Energy Availability in Females Questionnaire is a validated screening tool which may indicate the need for more in-depth assessments such as a measurement of resting metabolic rate or hormonal status.34 However, it is noted that this questionnaire has been principally developed from endurance-trained populations and is unlikely to be as specific and sensitive in other sporting groups. Further work to increase the validity of existing DE screening tools in broader athletic populations is underway while new screening assessment tools are in the validation phase.
Nutritional assessment
An athlete identified with possible DE should be referred to a sports dietitian for nutritional assessment of DE, EDs and LEA (table 4). The sports dietitian can: conduct screening questionnaires and interviews; complete a diet history and nutritional assessment; assess for the presence of special diets and restrictions/intolerances/allergies; perform an EA assessment; evaluate risk factors and warning signs of DE or EDs and assess where an athlete is on the spectrum of eating behaviour (figure 1). An athlete may be stable in weight but deficient in energy. Weight should not be the sole focus of the multimodal assessment of DE. The sports dietitian aims to understand the psychological component to food choices; the athlete’s views of their body and how these thoughts may impact on food selection. In some cultures and countries, food security may also overlay food choice and eating behaviours. Tracking where an athlete sits on the spectrum of eating behaviour helps a sports dietitian to better understand the athlete and apply appropriate and targeted nutrition interventions. An athlete’s ability or inability to follow nutrition advice/recommendations also provides further information as to where the athlete sits on the spectrum.
A nutrition assessment of the athlete with possible DE includes information on a range of issues
Nutrition for health and performance
Nutrition for athletes needs to encompass considerations of both health and performance. The characteristics of optimised nutrition in an athlete include:
Their eating practices are meeting their physical and mental health needs.
They are able to adapt their intake to meet the specific and changing demands of their sport.
They have flexibility around their eating and thoughts about food.
They are able to eat socially.
They are free of restrictive behaviours such as the avoidance of whole food groups; excessive counting of calories or macronutrients; or rigidity around foods consumed.
They have a healthy body image.
A plan for optimised nutrition should be safe, supported, purposeful and individualised. Nutrition practices are considered safe if they support the principle of ‘at first do no harm’ and in doing so, fundamentally prioritise athlete physical and mental health. The delivery of these optimal practices is supported when guided by the appropriately qualified and experienced members of the CMT with interaction and input from the wider performance team.
Medical assessment
The medical assessment of an athlete with identified DE should include thorough history (see online supplementary tables S1-S3 in Supplementary data) based on information provided by the athlete and CMT. All athletes with bone stress injury and/or menstrual dysfunction should be screened for LEA/RED-S and screened/assessed for DE and EDs. Care should be taken to select appropriate first-line and second-line investigations for the individual case to complete general and hormonal screenings, bearing in mind the timing of testing as it may relate to diurnal fluctuations, fasting status and menstrual cycle if known. Second-line biomarkers (online supplementary Table S3, data) of appetite, bone formation/resorption and other potential LEA indicators are an evolving space with some markers, such as ghrelin, currently only used in research settings. Consultation with an endocrinologist for interpretation of results may be required if outside the expertise of the practitioner. Referral to an appropriate specialist should be considered for more complex cases with valuable contributions frequently obtained in the fields of endocrinology, gynaecology and psychiatry.
Supplemental material
A summary of the endocrine effects of RED-S by Elliott-Sale et al (2018) provides the latest background on hormonal/physiological profiles in LEA in men and women provided in the supplementary data (online supplementary table S4).26 34 35 While some biomarkers/hormones show significant change in female athletes, menstrual dysfunction may be a more readily detectable clinical sign of LEA.11 Importantly, menstrual dysfunction should not be accepted as an inevitable consequence of being an athlete and should be investigated. Furthermore, hormonal profiling in a female taking hormonal contraception is not clinically useful. Hormonal profiling may be considered after a trial of 3 months off the combined contraceptive pill (COCP). Changes in biomarkers/hormones in men are different from those in women and may occur at a lower EA cut-off.36 The long-term consequences of impaired hormonal health in male athletes is not well established and requires further research.37
Bone health
Optimisation of bone health is important for short-term and long-term health and performance outcomes and involves the attainment of peak bone mass (between 18 years and 22 years of age) and prevention of accelerated BMD loss thereafter.9 10 38 A medical workup of an athlete with any combination of DE or ED, bone stress injury, menstrual and/or hormonal dysfunction should take into account various modifiers of bone health including nutrition, environmental, sport-specific mechanical loading, hormonal and iatrogenic factors. Instigation of appropriate pharmacological and bone loading treatment may be required. An athlete involved in a non-weight bearing and/or endurance sport (eg, swimming or cycling) should consider a programme involving drop jumps to satiate ground reaction force contribution to bone health,39 40 a typical programme might involve a two-footed landing from a 30 cm platform, repeated 10 times with 10 second gap between jumps.40 41
Athletes with 6 months or more of LEA, DE, ED or amenorrhoea should have BMD measured by dual-energy X-ray absorptiometry (DXA),9 as per the guidelines of the International Society of Clinical Densitometry and the American College of Sports Medicine.28 42 Assessments should refer to Z-scores (age-matched and sex-matched). In the athletic population, low BMD is defined as a Z-score between −1 SD and −2 SD, together with a history of nutritional deficiencies, hypo-oestrogenism, stress fracture or other secondary clinical risk factors for fracture.9 As athletes in weight-bearing sports should have a BMD that is 5%–15% higher than non-athletes, a BMD Z-score less than −1 SD warrants further attention.9 DXA assessments should be repeated in at-risk adults every 12 months and in at-risk adolescents at a minimum of every 6 months, preferably using the same DXA machine.9
Calcium supplementation may be required if the recommended daily intake is not met from food sources, but such decisions should be made only after a thorough dietary assessment by a sports dietitian. Guidelines for calcium intake vary slightly between countries with the daily recommended dietary intake of calcium 1000 mg for men and women aged 19–50 years in Australia and the USA, and 1300 mg for children and adolescents, aged 12–18 years in Australia, and 9–18 years, in the USA.43 44 While the biochemical cut-off for vitamin D deficiency is controversial,42 45 46 blood levels <50 nmol/L in winter months or <75 nmol/L in summer months should be considered for supplementation.45 The endocrine society clinical practice guidelines provide current recommendations for vitamin D supplementation across age ranges and subpopulations.47 Vitamin D deficient adults can be treated with 50 000 IU of vitamin D once a week for 8 weeks, followed by maintenance therapy of 1500–2000 IU daily, with repeat serum vitamin D testing to assess response and prevent toxicity.47 Inadequate EA is likely to be the most important dietary cause of poor bone health; there is evidence of suppressed bone formation once EA decreases below 30 kcal/kg FFM/day in women28 while impaired bone health is likely to occur below 20–25 kcal/kg FFM/day in men.36 48 Serum testosterone within the lowest quartile of the normal clinical range (total testosterone 9–38 nmol/L) is associated with an increased risk of bone injuries in men.36
Female athletes
Amenorrhoea may occur in up to 66% of athletes,49 but its presence for more than 3 months should not be accepted as an inevitable consequence of being an athlete and must be investigated.4 Aetiology of oligo-amenorrhoea may include pregnancy, primary ovarian insufficiency, hyperprolactinaemia, thyroid dysfunction, polycystic ovarian syndrome (PCOS) and functional hypothalamic amenorrhoea (FHA), which is a diagnosis of exclusion.9 50 The underlying cause of FHA is LEA rather than exercise volume or body composition, thus optimisation of energy availability (EA) should be the first line treatment of FHA,37 however it may take more than 6 months for favourable menstrual changes.28 Assessment of an athlete with menstrual dysfunction by a sports dietitian forms a part of the complete care of the female athlete.
The triad amenorrhoea algorithm as produced by Joy et al (2014) provides a succinct and systematic approach to diagnosis and referral of an athlete with menstrual dysfunction.50 The clinical signs and symptoms of menstrual dysfunction can be used as a surrogate marker for LEA, but these may be masked by concurrent use of oral contraception. Treatment of menstrual dysfunction via supplementation with exogenous hormones, such as the COCP, does not correct the cause of FHA and does not protect against BMD loss.9 10 37 50 To protect BMD in these athletes, it is preferable to use transdermal oestrogen, with cyclic oral progestin as an adjunct; this is applied twice weekly as a transdermal51 β-oestradiol (E2) patch (100 µg), with cyclic micronised progesterone (200 mg) for 12 days each month.50 The transdermal hormones are not a form of contraception and risk factors which may preclude use of the COCP should be considered.50
Male athletes
LEA may suppress reproductive and metabolic hormones in men at <20–25 kcal/kg/fat free mass (FFM)/day10 but the clinical signs and symptoms are relatively subtle.28 35 37 Reduction in libido and loss of nocturnal penile tumescence may be a sign of relative reduction in testosterone. A relative reduction in testosterone that may remain at a subclinical threshold may be seen in the LEA state.36 Testosterone is best measured as a fasted, morning sample to avoid wider fluctuations throughout the day. A serial/longitudinal record for the individual in the clinical context may be more beneficial than a single measurement.37
Psychological assessment
Mental health
A comprehensive mental health evaluation is critical to determining intervention and treatment, and can be provided by a psychologist or doctor within the CMT. The mental health evaluation aims to determine range and severity of DE symptoms, diagnose EDs and other mental illnesses, and identify any immediate medical or psychological risk. EDs have one of the highest mortality rates of all psychiatric illnesses, and those diagnosed with an ED have significantly elevated suicide risk.52–54 Therefore, a suicide risk assessment should be undertaken to include suicidal ideation, deliberate self-harm, previous suicidal behaviours and self-harm events, agitation and current or past risk of harm to others.
The use of interview protocols is well suited to evaluating eating behaviours and beliefs according to Diagnostic and Statistical Manual of Mental Disorders diagnostic criteria. The EDE 17.0 or EDE-Q 6.0 can be used for these purposes, as can a mental health evaluation such as the Mini International Neuropsychiatric Interview (MINI 7.0.2).55 The MINI 7.0.2 provides a diagnosis of prior and current comorbid conditions, including EDs as well as suicidality. When a focused ED or thorough mental health evaluation is required, this should be done by an appropriately trained mental health clinician.
Family and social networks
In addition to mental health, psychologists will also examine the athlete’s psychosocial history, social support and perceived stress across relevant life domains (sport, school/work, social). Family history of mental illness is also relevant, particularly the presence of DE or body image disturbances. As part of the social network, assessment and engagement of parental support early in the process is important to facilitate implementation of the recommended intervention, particularly if health deteriorates.4
Where DE symptoms are detected or there is a high risk of developing an ED, additional information regarding the athlete’s readiness for early intervention and treatment is important. This includes the athlete’s readiness to change, as well as anticipated challenges and strengths or protective factors. The athlete’s readiness to change, or motivation for treatment is a consistent predictor of treatment success.56 The complexity of DE requires a biopsychosocial approach, and it is important to know the type and nature of support within the athletes’ social network. A supportive and well-aligned network is critical to successful treatment.57
Treatment and ongoing monitoring of the athlete with DE
Once DE is identified in the high performance athlete, the review and maintenance process of care requires information sharing and progression of treatment goals between the athlete, CMT, sports coaches and support staff. A designated member of the CMT should ideally coordinate the flow of information within the team to formulate individual athlete treatment and maintenance goals, clearly outlining medical and behavioural objectives to ensure safety and sports-specific RTP criteria. This requires engagement with the athlete and follow-through from sports staff. A large amount of information is typically collected in areas of nutrition, medicine and psychology; a consistent, systematic approach is required to ensure that all avenues have been explored and openly communicated. The CMT can formulate a time line for maintenance and review.
Modifications, exclusions and RTP decisions
Given the potential for injury and/or illness if an athlete continues to train through DE, there may be times when training modification or full exclusion is required. An ED diagnosis may not be needed to justify the need for modification to training and/or competition to ensure the athlete’s safety. It is reasonable that athletes with DE can continue to participate in sports, provided they engage appropriately and consistently with their support team.4 Each sport governing organisation or federation should have guidelines to support difficult decisions with respect to affected athletes and the particular diagnoses (eg, RED-S).57 Clinical assessment tools which may assist and guide decision making in relation to RTP, include the RED-S Clinical Assessment Tool10 58 and the 2014 Female Athlete Triad Coalition Consensus Statement (female athletes with DE, menstrual dysfunction and low BMD).50
Currently, there are no accepted values for sport-specific minimum or optimal levels of body fat or body weight.7 As such, these values should not be set by sporting organisations. Within the clinical ED treatment environment, the Safe Exercise at Every Stage guideline may be used to guide clinical reviews and RTP plans.59 Athletes with an ED should be referred to an appropriate ED service and assisted to transition back into the high performance sporting environment as part of their recovery.
Prevention
Prevention and education
Creating and embedding an environment and culture that assists in the prevention of DE is of utmost importance to promoting the health of all athletes and minimising DE risk and incidence. To minimise DE risk and incidence, key points of prevention are identified by Sundgot-Borgen and Torstveit (2010) and include advocating health and well-being, de-emphasising body weight, and making DE a ‘health and safety issue’ not a ‘coaching issue’ among others.57 Prevention of DE can also involve advocacy for changes to unhealthy sport rules and identifying strategies to mitigate existing ‘at risk’ rules. Education programmes are the best method of primary prevention of DE and EDs.60 The main aims of education are to reduce stigma, promote healthy relationships with food and body, encourage open and honest discussion, educate about potential health and performance consequences, and educate about optimal nutritional strategies.4 Best practice in this area would see coaches, sport support staff members and judges undergoing an initial comprehensive education programme and regular refresher education sessions. Athlete prevention efforts are best directed at modifiable risk factors such as body dissatisfaction and low self-esteem, and seek to minimise potential adverse effects of body manipulation.61
Assessment and manipulation of body composition
‘Dieting’, the deliberate restriction of calories and/or specific nutrients for actions to promote the purpose of loss of body mass and/or body fat, is well documented as one of the major risk factors for developing an ED.62 Yet, physique assessment is a common activity undertaken within athlete monitoring protocols, and manipulation of body composition, including weight or body fat loss, is a common goal within an athlete’s sports nutrition plan. Routine assessment of body composition requires careful deliberation of the rationale for the assessment (ie, is it purposeful and necessary), who is undertaking the measurements, the level of training required to take the measurements as well as the level of support available to the athlete to interpret the information and provide recommendations. Examples of body composition assessment techniques include (but are not limited to) body mass weighing, skinfolds and DXA. If manipulation of body composition is indicated, expert nutrition support from a sports dietitian should be provided from end to end: that is, from preassessment through assessment to advice and ongoing monitoring. A sports dietitian can formulate advice as to whether to test athletes or not, based on some of the following factors: history of DE or EDs, age, level of nutrition support in the domestic training environment, and the type of protocols used (weighing, skinfolds and DXA). It should be considered that the coach is not primarily involved in the body composition assessment process. The underpinning philosophies of body composition monitoring are that no harm should be done to the athlete being tested and that the data collected from such protocols should be treated as personal and confidential medical information.63 Education regarding body composition and testing including procedure, rationale, consent and use of information must be conducted for all athletes prior to commencing any testing.
Strategies for safe weighing and body composition assessment
Strategies for safely weighing and assessing an athlete’s body composition include gaining explicit consent for every measurement (verbal), checking in with the athlete prior to the measurement and offering to ‘blind weigh’ the athlete so that they do not see the results of the examination.64 If there is any distress about being weighed or measured, this needs to be taken seriously and the coach and CMT need to discuss the appropriate course of action for this athlete. There are some ED treatment modalities which include viewed weighing as a form of exposure therapy and monitoring (eg, enhanced cognitive therapy),65 however these should not be undertaken by anyone who has not been appropriately trained or does not have adequate support from the CMT and clinical supervision. One member of the CMT will be responsible for ongoing monitoring of this metric, so that the athlete is not weighed or measured either too frequently, or by different clinicians and can foster trust and appropriate interpretation of results to promote continuity of care.
Body image
Positive body image is one of the protective factors against development of EDs, and forms a foundation for most effective ED prevention programmes in athletes.66 It is notable to acknowledge that negative and positive body image are two different yet intersecting constructs and both need to be taken into consideration within both the general and athlete populations.67 An athlete’s perception of their physical self, and the thoughts and feelings that are entailed, can produce perceptual, affective, cognitive and behavioural manifestations. An athlete may frequently have separate body images; an athletic body image and a social body image.68–71 There may be tensions between the socially desirable body image and the ideal physique for performance in the athlete’s sport.72 Both male and female athletes may have a body image that is in conflict with cultural norms and gender stereotypes. Body image dissatisfaction in male and female athletes is a risk factor for DE or ED irrespective of the perceived weight-related performance pressures of their sport.68 72 73 Some subpopulations are at additional risk for body image dissatisfaction; for example, para-sport athletes and those with concurrent conditions such as diabetes mellitus74 75 or PCOS.76 The biological changes that occur during puberty and adolescence may contrast with the ideal physique in a sport, making this a higher risk time for the development of DE or an ED.7
Creating a healthy sport system
Support systems for healthy participation in sport involving individuals with specific expertise in DE and ED will decrease the likelihood that such problems will occur in athletes. Every sporting organisation should be aware of the increased prevalence of DE in high performance athletes and have established guidelines for early identification and prevention of DE. Guidelines should reflect this position statement, be sport-specific, and promote nutrition practices that are safe, supported, purposeful and individualised. Sporting organisations need communication protocols to refer athletes to a member of the CMT, as part of accepted and routine care to support athlete health and performance optimisation. Some sporting organisations may not currently have access to a member of the CMT. Sports should work to build their healthcare network to ensure that they are able to work with a fully comprised CMT.
The rules and regulations for specific sports can influence prevalence of DE behaviours in athletes.77 Sporting organisations should be aware of the implications of the specific rules within their sport and their potential impact on the eating practices of their athletes. It may be necessary for organisations to lobby for rule changes to decrease the risk of practices contributing to DE or EDs within their sport.
Lastly, further research is required in the area of DE in high performance athletes, particularly intervention studies, prevention studies, validation of sport-specific and gender/cultural-specific screening tools, as well as the para-athlete and investigating the prevalence of DE in the variety of athlete subpopulations.
Conclusion
This AIS-NEDC document reviews the current literature and provides a set of positions and key concepts on the approach to early identification, assessment and prevention of DE in high performance sport. Athlete health and welfare must remain the primary focus of preventing and managing DE in sport at all times. Awareness, recognition and referral of the athlete with DE to a CMT comprising a doctor, sports dietitian and psychologist forms the foundation of support for optimised nutrition. Sporting organisations should develop sport-specific guidelines around DE to best optimise health and performance. This document provides guidance for the high performance system to improve the awareness and management of this complex condition.
Summary position statements and key concepts
Disordered eating prevalence and consequences on health and performance
There is a spectrum of eating behaviours in high performance sport that spans from optimised nutrition through disordered eating to clinically diagnosed eating disorders.
Disordered eating and low energy availability can occur together or in isolation. Identification of one necessitates the investigation of the other. Low energy availability underpins the syndrome of relative energy deficiency in sport, which has many health and performance consequences.
Disordered eating can occur in any athlete, in any sport, at any time, crossing boundaries of gender, age, body size, culture, socioeconomic background, athletic calibre and ability.
In addressing the health and performance consequences of disordered eating or eating disorders, health must be the priority.
Inappropriate eating practices increase the risk of illness and injury. Compromised training in turn impairs performance.
Personal attributes which underpin successful performance, combined with the sport environment may leave athletes vulnerable to disordered eating.
Early identification of disordered eating
Everyone in the high performance sports system has a role as early identifiers of disordered eating. Education and literacy are required around risk factors, warning signs and red flags.
The goals of assessment are to identify disordered eating or eating disorders, investigate the presence of low energy availability/relative energy deficiency in sport and its consequences, and manage acute and chronic complications in the athlete.
The core multidisciplinary team
The core multidisciplinary team of doctor, sports dietitian and psychologist form the cornerstone of professional assessment and management of athletes on the spectrum of eating behaviour.
The core multidisciplinary team works with athletes and their support network to investigate and manage the health and performance of athletes taking into account individual case characteristics and sport-specific demands.
Doctors, sports dietitians and psychologists working within sport need to have an awareness and constantly seek to improve their knowledge and skills regarding disordered eating.
The core multidisciplinary team is responsible for ensuring continuity of care.
Athletes with an eating disorder should be referred to a specialised eating disorder service. Where there is a delay in access, the core multidisciplinary team is responsible for the athlete’s care.
It is crucial that there are well-defined roles and a clear communication strategy within the core multidisciplinary team and across relevant stakeholders.
Nutritional assessment
When possible disordered eating or an eating disorder is identified in an athlete, a nutrition assessment is required.
A sports dietitian will determine where an athlete currently sits on the spectrum of eating behaviours (from optimised nutrition to eating disorders) and track their progression along the spectrum based on specific, targeted nutritional interventions.
Manipulation of nutrition practices can play a valuable role in athletic performance. Athletes must engage in optimised nutrition that is safe, supported, purposeful and individualised.
An athlete may be stable in weight but deficient in energy. Weight should not be the sole focus of the multimodal assessment of disordered eating.
Medical assessment
All athletes with bone stress injury and/or menstrual dysfunction should be screened for low energy availability/relative energy deficiency in sport and screened/assessed for disordered eating and eating disorders.
Understanding menstrual function in the individual athlete is essential for providing optimal care. Menstrual dysfunction should be investigated.
While the clinical signs and symptoms are relatively subtle, impaired hormonal health can also occur in male athletes.
Eating disorders can be life-threatening; doctors should have the key clinical competency to identify an athlete who is unstable and requires removal from sport, emergency intervention and admission to supportive care.
Psychological assessment
Athletes being evaluated for disordered eating or eating disorders require a comprehensive mental health evaluation.
Eating disorders have one of the highest mortality rates of any mental illness. An athlete’s medical and psychological safety is paramount and requires ongoing vigilance.
Return to play
The core multidisciplinary team monitors and communicates medical and behavioural objectives to ensure safety and inform athlete-specific return to play criteria, with input from established return to play frameworks as required.
Prevention and education
Education is the best evidence-based method for primary prevention of disordered eating and eating disorders and is included within the well-being and performance health strategy. Education should target the key issues in a sport, and may include elements related to increasing awareness of the problem and its risk factors, improving body image and raising nutrition literacy.
Athletes, coaches, support staff members and judges should undergo an initial comprehensive education programme and regular refresher education sessions.
Body composition assessments in athletes
Body composition assessment and weighing strategies must reflect individual needs and emphasise choice, collaboration, trust, safety and empowerment.
High frequency self-weighing and/or team or service provider weighing should be moderated to reduce risk to athletes.
Body composition assessment should only be undertaken if it is purposeful and necessary to optimise the performance of the athlete.
All athletes should attend an education session with a qualified anthropometrist prior to any body composition testing being conducted. This should include provision of information to explain the rationale for testing, method of assessment, storage and use of information, and allow time for questions.
All athletes should complete a consent process for body composition assessments, with parental consent where appropriate.
Prior to undertaking body composition assessment and/or weighing strategies, serious consideration must be given regarding the purpose of the assessment. Assessment should not take place without adequate nutrition support or if the assessment is considered likely to be harmful to the athlete with disordered eating or an eating disorder.
The entire process of body composition assessment and feedback is treated as personal and confidential medical information. It must be made clear where the information is being stored, who the information is being shared with and for what specific purpose(s).
Body image
Positive body image is one of the protective factors against development of eating disorders, and forms a foundation for most effective eating disorder prevention programmes.
Body image dissatisfaction in male and female athletes is a risk factor for disordered eating or eating disorders irrespective of the perceived weight-related performance pressures of their sport.
Healthy sport systems
Every sporting organisation should have a guideline on prevention and early identification of disordered eating for their sport that encompasses continuity of care, addresses the specific context of their particular sport, and upholds the core principle of ‘first do no harm’ with regards to athlete body image, nutrition, performance and related measures.
Sports have a responsibility to all athletes across the entire high performance pathway to create a healthy sports system, both in the environment and culture of the sport.
Acknowledgments
The authors thank Dr Nicolin Tee and Alice Wallett for assistance with preparation of the manuscript and Dr Kirsten Peterson and Dr Greg Lovell for initial academic discussions. The authors also thank the National Eating Disorders Collaboration Steering Committee and staff team for their contributions, the Australia and New Zealand Academy for the Eating Disorders Executive Team and the Butterfly Foundation Prevention Services for drafting and reviewing this position statement.
References
Footnotes
Correction notice This article has been corrected since it published Online First. Figure 2 has been corrected and replaced.
Contributors KRW, NAJ, RA, HDS, NV, LMB, DH were all involved in the design of the work, KRW and NAJ drafted the manuscript, RA, HDS, NV, LMB, DH critically reviewed the manuscript. All authors gave final approval for the manuscript.
Funding This work was funded through staff allocation by the Australian Institute of Sport and the National Eating Disorders Collaboration. This is a summary version of the full AIS and NEDC position statement on disordered eating in high performance sport, available at: www.ais.gov.au/disorderedeating.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.