Article Text

Abstract
Objective To investigate prevalence, incidence and profile of musculoskeletal injuries in para athletes.
Design Systematic review.
Data sources Searches were conducted in MEDLINE, EMBASE, AMED, SPORTSDiscus, CINAHL and hand searching.
Eligibility criteria Studies were considered if they reported prevalence or incidence of musculoskeletal injuries in para athletes. Study selection, data extraction and analysis followed the protocol. Meta-analyses were conducted to estimate the prevalence and incidence rate among studies and subgroup analyses investigated whether methodological quality and sample size of the studies influenced on the estimated injury prevalence and incidence. The Grading of Recommendations Assessment, Development and Evaluation system determined the strength of evidence.
Results Forty-two studies were included. The prevalence of musculoskeletal injuries was 40.8% (95% CI 32.5% to 49.8%). Because of imprecision, indirectness and inconsistency, the strength of evidence was very low quality. The incidence of musculoskeletal injuries was 14.3 injuries per 1000 athlete-days (95% CI 11.9 to 16.8). The strength of evidence was low quality because of imprecision and indirectness. The subgroup analyses revealed that the sample size influenced on estimated injury prevalence and methodological quality influenced on estimated incidence. Injuries were more prevalent in the shoulder, for non-ambulant para athletes, and in the lower limbs, for ambulant para athletes.
Summary/conclusion Para athletes show high prevalence and incidence of musculoskeletal injuries. Current very low-quality and low-quality evidence suggests that future high-quality studies with systematic data collection, larger sample size and specificities of para athletes are likely to change estimates of injury prevalence and incidence in para athletes.
PROSPERO registration number CRD42020147982.
- epidemiology
- sports
- disabled
- injuries
Statistics from Altmetric.com
INTRODUCTION
Since the first Paralympic Games in Rome in 1960, with 400 athletes with spinal cord injury from 23 countries,1 the number of athletes with disabilities competing at major sports events has grown exponentially, reaching 4328 athletes from 160 countries in 22 sports at the Rio 2016 Summer Paralympic Games.2 Especially for individuals with a disability, sports practice has a positive impact on cardiovascular fitness, self-efficacy, self-perceived quality of life and community participation.3 4 Although sport participation is beneficial, it also comes with a risk of musculoskeletal injuries.5 6
Comparison of the injury incidence rates between Paralympic Games and the Olympic Games shows to which extent sports injuries need attention in athletes with disabilities, henceforward defined as para athletes. During the 2016 summer Paralympic Games, a total of 510 injuries were reported in 441 athletes, with an injury incidence rate of 10 injuries per 1000 athlete-days.7 This incidence rate was almost twice as high when compared with the 5.7 injuries per 1000 athlete-days during the 2016 summer Olympic Games.8 In addition to a high incidence rate, the profile of Paralympic sports injuries is extremely variable.9 The different levels of para athletes’ classification favour the participation of athletes with different types and degrees of disabilities in the same sport modality. This wider presentation of disability may help explain the great variety of injury profiles in Paralympic sports.10 11
The consequences of injuries in para athletes are often not limited to sports time loss or reduced sports performance. Injuries also frequently pose an additional barrier to activities of daily living in para athletes.6 For example, an upper limb muscle injury in a disabled wheelchair javelin thrower can also affect his or her ability for independent locomotion during daily living.4 Thus, to prevent these injuries, the first step is to understand the extent of the sports injury problem.12 Weiler et al 13 conducted a systematic review of sports injuries in athletes with disabilities but the wide variability in reported injury rates prevented the authors to conduct a meta-analysis. The inclusion of studies without clear definition of sports injury might have contributed to this wide variability. Furthermore, another methodological shortcoming in this area is that estimates of prevalence and incidence comes from studies with small samples. Since the publication of this previous review in 2016,13 new large studies on Paralympic sports injuries have been conducted, including longitudinal studies. Therefore, the primary aim of this systematic review with meta-analysis was to investigate the prevalence, incidence and profile of musculoskeletal injuries in para athletes. As a secondary aim, we investigated whether methodological quality and sample size influenced the prevalence and incidence reported.
METHODS
Search strategy
For this systematic review, we followed recommendations from the Joanna Briggs Institute Reviewers’ Manual,14 the Cochrane Collaboration15 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses reporting guidelines.16 The review’s protocol was registered at PROSPERO (CRD42020147982). Search strategies were conducted in August 2019 and updated in May 2020 in MEDLINE, EMBASE, AMED, SPORTSDiscus and CINAHL. In addition, we handsearched the reference list of previous reviews on the topic. There was no date or language restriction. Our sensitive search strategy included the combination of the following terms ‘prevalence’, ‘incidence’, ‘epidemiology’, ‘injury’ and ‘para athlete’. Online supplemental material 1 shows a detailed search strategy for each database.
Supplemental material
Eligibility criteria
We included published studies that reported the prevalence or incidence of musculoskeletal injuries in para athletes, including prospective, and retrospective cohort studies, without language, sample size, age or publication date restrictions. Para athlete is a general term used for athletes with an impairment who participate at any competitive level.10 To be included, studies should report the prevalence or incidence of musculoskeletal injury in para athletes, along with a clear definition of musculoskeletal injury. Given that definitions of musculoskeletal injuries are extremely variable in the literature, any type of definition was accepted. When studies reported data from the same cohort or event, with similar methodology and the same definition of injury, only the study with global data on prevalence and incidence of injury was included.
Study selection and data extraction
Two reviewers (LSPP and FOM) independently screened titles and abstracts and assessed potential full texts. A third reviewer (RR) solved any between-reviewer disagreements.
Two reviewers (LSPP and FOM) also independently extracted descriptive and outcome data of all included studies. A third reviewer (RR) solved any discrepancies between data extractions. Descriptive information included data collection setting, sample characteristics (eg, sex, age, sport, disability, years of practising in para sports), injury characteristics (eg, injury definition, professional responsible for injury diagnosis and record, number of sports injuries), the prevalence and incidence rate of injuries with 95% CIs per study. When these data were not provided, we estimated prevalence and incidence rate using the number of athletes injured, reported number of injuries, total sample and time frame of the competition. For incidence rate, if the time frame of the competition was not reported we contacted authors or performed an internet search to clarify the start and closing dates of the competition, considering the number of days of the competition. When a study reported more than one competition, the injury incidence rate was calculated for each competition. Prevalence was estimated as the proportion of athletes affected by injury at any given time,17 and incidence rate was estimated as the number of injuries divided by the total person-time at risk (athlete exposures).18
Assessment of the methodological quality
Two independent reviewers (LSPP and FOM) assessed the methodological quality of included studies using ‘The Joanna Briggs Institute Prevalence Critical Appraisal Tool’.14 A third reviewer (RR) solved potential disagreements regarding the risk of bias scoring. Each item was rated as ‘yes’, ‘no’, ‘unclear’ or ‘not applicable’ according to information available in each study, with a maximum score of nine points. One of the items in this tool is sample size. To evaluate if the sample size of each included study was appropriate, we used the following equation: sample size= Z 1−α/2 : p(1 − p) d2
where p was the expected prevalence (12.1%), defined based on a previous study,7 Z was the confidence level (1.96), and d was the precision (5.0%).19 The sample size estimation resulted in a minimum required sample size of 163 participants. A third reviewer (RR) solved potential disagreements regarding the risk of bias scoring.
Data analysis
Descriptive statistics were used to summarise data in meta-analysis. The prevalence and in incidence rate estimated from individual studies were pooled, using a random-effects model.15 Studies that reported injury prevalence and incidence from the same subgroups of a larger sample during the same competitive event were excluded from the analysis. I2 was used to explain what proportion of the observed variance was attributed to the variance in true effects rather than to sampling error.20 A prediction interval was used to access the heterogeneity, that is, how much effect size varies across studies.20
Quality of evidence
To summarise the overall quality of the evidence the Grading of Recommendations Assessment, Development and Evaluation (GRADE system)21 was used for the meta-analysis pooling prevalence and incidence data from all included studies. Scoring of evidence started at high-quality evidence which was downgraded one level if one of the following prespecified criteria was present: (1) poor methodological quality (downgraded if ≥25% of the studies included in the meta-analysis used inappropriate sampling method or statistical analyses (ie, items 2 and 8 in The Joanna Briggs Institute Prevalence Critical Appraisal Tool)); (2) imprecision (downgraded if ≥25% of the included studies did not present minimum required sample size of 163 participants); (3) indirectness (downgraded if ≥25% of the included studies did not use valid and reliable methods for data collection, for example, validated questionnaires previously described in the literature or standardised systems for recording sports injuries) and (4) inconsistency (downgraded if prediction interval has a variation ≥0.5 between upper and lower limits). These prespecified criteria were defined considering the items of Joana Briggs that correspond to the GRADE system criterion, for example, items 2 and 8 for poor methodological quality, and the corresponding index of the meta-analysis, such as the prediction interval for indirectness criterion.
We performed subgroup analyses to investigate whether methodological quality and sample size influenced overall estimates of prevalence and incidence. For the subgroup analysis, the criteria used to classify studies in high and lower methodological quality was the median score of The Joanna Briggs Institute Prevalence Critical Appraisal Tool. Studies that presented median risk of bias ≤6 points out of 9 were pooled as lower methodological quality. For the sample size subgroup analysis, the cut-off sample of 163 para athletes were used to classify studies into small and large sample size. For the subgroup analyses, if there was no overlap between 95% CIs between subgroups, we interpreted that each subgroup provided different estimates. All analyses were performed using Comprehensive Meta-Analysis, V.2.0 (Biostat, Englewood, New Jersey, USA).
RESULTS
Flow of studies
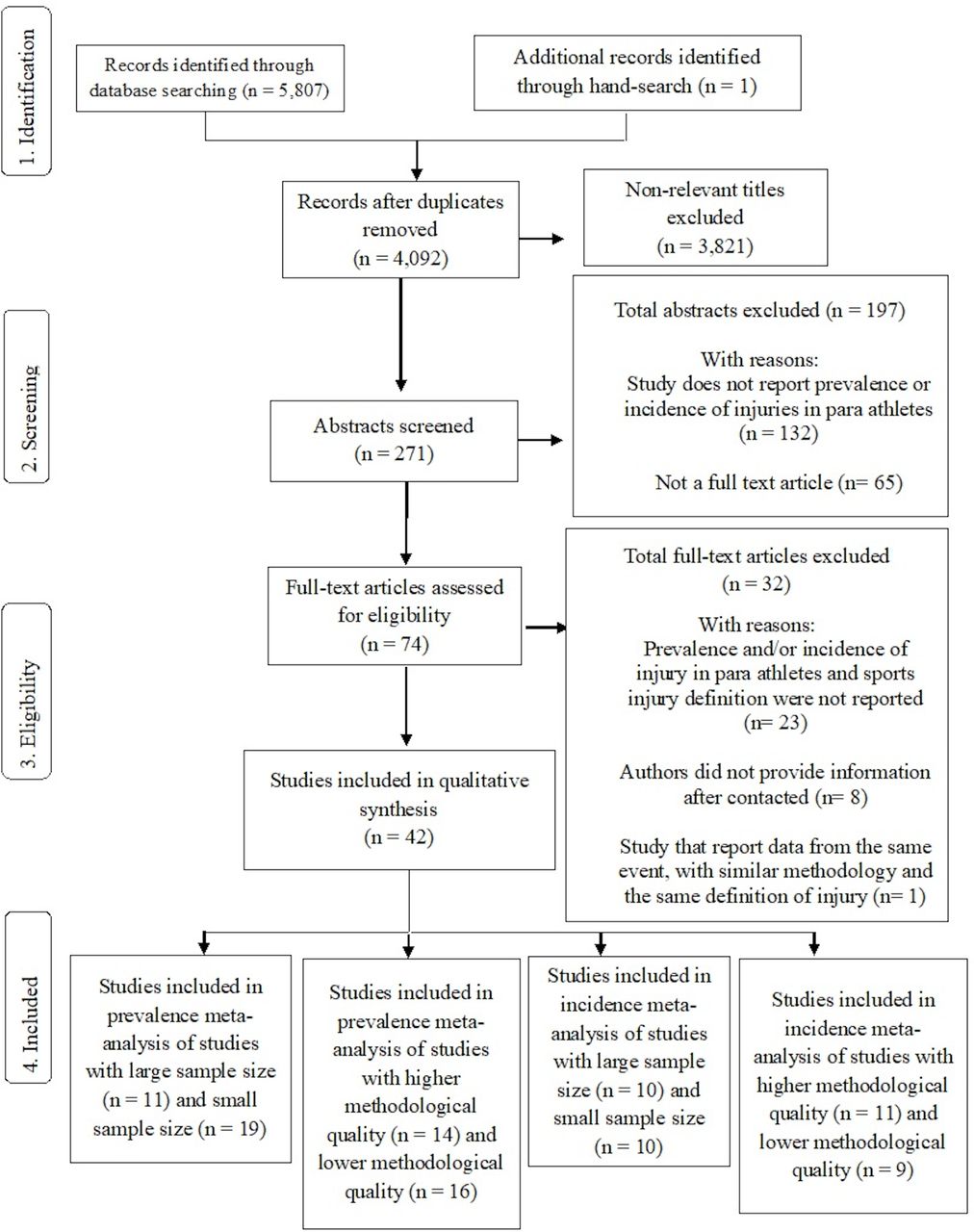
The electronic search strategy identified 4092 records from the selected databases after excluding duplicates. After screening titles, abstracts and reference lists, 74 potentially relevant records underwent full-text review, including one additional study found by handsearching. Twenty-three studies failed to meet the inclusion criteria, eight studies did not provide information after contact and one study was excluded because it reported data from the same event, using similar methodology, and using the same injury definition than another included study. Thereby, 42 studies were included in this review. Figure 1 shows the flow chart of studies through the review.

PRISMA flow chart of studies through the review. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included studies
Twenty-five out of 42 studies included reported both injury prevalence and incidence rates,7 22–45 7 studies only reported prevalence data46–52 and 10 studies only reported incidence rates.3 53–61 Of the 35 studies with incidence data, 20 studies reported injury incidence rate per days,3 22–29 33 39 41–44 53 55–58 5 studies reported incidence per hours,31 32 34 59 60 5 studies reported injury incidence rate in different competitions,35–37 45 54 three studies differentiated the injury incidence rate between precompetitive and competitive periods,7 30 40 one study reported injury incidence rate per 1000 athlete exposures,61 and one study reported injury incidence rate per 100 athlete competitions.38 The number of participants ranged from 1132 to 3657,7 with a mean of 390.9 participants and median of 135.5. Regarding sex, 2 (4.8%) studies were conducted with females,47 50 4 (9.5%) with males22 33 36 58 and 36 (85.7%) with both sexes.3 7 23–32 34 35 37–46 48 49 51–57 59–61 Six studies were performed with wheelchair para athletes,22 27 33 47 50 59 11 studies with ambulant para athletes25 32 34–38 41 44 52 58 and 25 studies with both wheelchair and ambulant para athletes.3 7 23 24 26 28–31 39 40 42 43 45 46 48 49 51 53–57 60 61 Twenty studies were sport-specific,3 22–24 26–28 32 33 35–37 41 44 47 50 52 53 55 59 19 were multisport7 25 29–31 38–40 42 43 45 46 48 49 54 56–58 60 and 3 studies did not report para sport modality.34 51 61 Ten studies did not report para athlete disabilities,26 28–30 39 42 54 57 59 61 22 studies presented information about classification level of para athletes,3 7 22 24 26 31 35–41 43 44 48 50 52 55 57–59 23 studies specified the assistive devices used by para athletes,3 7 22 24 26–28 30 31 33 39 40 46–48 50 51 53 55–57 59 60 and in 30 studies the injury diagnosis was confirmed by a medical practitioner.3 7 23 25 26 28–31 33–40 45 46 48 50 51 54–61 Only five studies presented longitudinal prospective design,23 31 34 59 60 while 37 studies reported retrospective or competitive events data.3 7 22 24–30 32 33 35–58 61 Online supplemental material 2 shows the characteristics of the included studies and demonstrates the level of inconsistency in injury definitions and the report of para athletes’ exposure (days, hours or competition).
Supplemental material
Quality assessment
Methodological quality issues are reported in table 1. None of the studies had a negative or unclear answer to item 2, 22 studies did not present appropriate sample size,22–24 27 31–37 41 44 45 47–50 52 53 55 59 18 studies did not use valid methods for data collection or did not clearly present the methods used for data collection,24 27 29 34–38 44 49 51–54 56 57 59 60 and 5 studies had a negative or unclear answers to item 8.24 29 32 53 54 Twenty-one studies scored ≤6 out of 9.23 24 27 29 32 33 35–38 45 47 49–54 56 57 59 Mean (SD) methodological quality of the included studies was 6.3 (1.8) out of 9 (ranging from 0 to 9).
Methodological quality of the included studies (n=42)
Prevalence of musculoskeletal injuries in para athletes
The pooled prevalence estimates including data from 30 studies (n=12 151)7 22–25 27 29–52 found was 40.8% (95% CI 32.5% to 49.8%; I2: 97.7%; prediction interval: 0.1–0.8). The overall quality of evidence was rated as very low quality (ie, downgraded due to imprecision, indirectness and inconsistency) (table 2). The subgroup analysis based on higher and lower methodological quality revealed no significant difference. The pooled estimate for studies with higher methodological quality (n=10 408)7 22 25 30 31 34 39–44 46 48 was injury prevalence of 34.7% (95% CI 25.4% to 45.4%; I2: 98.2%; prediction interval: 0.1–0.8) and for studies with lower methodological quality (n=1743)23 24 27 29 32 33 35–38 45 47 49–52 was 47.4% (95% CI 32.1% to 63.3%; I2: 95.8%; prediction interval: 0.1–0.9) (figure 2). For the subgroup analysis based on study sample size, studies with large sample size showed significantly lower prevalence estimate than studies with small sample size. While studies with large sample size (n=11 068)7 25 29 30 38–40 42 43 46 51 showed injury prevalence of 18.5% (95% CI 12.7% to 26.1%; I2: 98.3%; prediction interval: 0.1–0.6), the prevalence estimate from studies with small sample size (n=1083)22–24 27 31–37 41 44 45 47–50 52 was 58.3% (95% CI 48.2% to 67.8%; I2: 88.1%; prediction interval: 0.2–0.9) (online supplemental material 3).
Supplemental material

Meta-Analysis for overall injuries prevalence in para athletes and subgroup analysis for studies with higher and lower methodological quality.
Evidence table for outcome measure
Incidence rate of musculoskeletal injuries in para athletes
For incidence rate, the pooled estimate including data from 20 studies (n=11 608)7 22–25 27 29 30 33 39–45 53 55–57 that reported injury incidence rate per days and also the number of injuries, sample size and exposure in days. The incidence rate was 14.3 injuries per 1000 athlete-days (95% CI 11.9 to 16.8; I2: 98.4%; prediction interval was 0.1–0.2). The overall quality of evidence was rated as low quality (ie, downgraded due to imprecision and indirectness) (table 2). The subgroup analysis showed a significant lower incidence rate in studies of higher methodological quality as compared with studies with lower methodological quality. The pooled estimate for studies with higher methodological quality (n=9999)7 22 30 39–44 55 was injury incidence rate of 11.7 per 1000 athlete-days (95% CI 8.9 to 14.5; I2: 98.6%; prediction interval was 0.1–0.4) and pooling of 1609 para athletes from studies with lower methodological quality23 24 27 29 33 45 53 56 57 estimated the injury incidence of 23.1 per 1000 athlete-days (95% CI 17.1 to 29.2; I2: 98.4%; prediction interval was 0.1–0.4) (figure 3). The subgroup analysis showed no clear difference with regards to sample size. While studies with large sample size (n=10 981)7 25 29 30 39 40 42 43 56 57 estimated an injury incidence rate of 14.4 per 1000 athlete-days (95% CI: 11.1 to 17.7; I2: 98.8%; prediction interval was 0.1–0.2) studies with small sample size (n=627)22–24 27 33 41 44 45 53 55 showed an incidence rate of 14.7 per 1000 athlete-days (95% CI: 11.1 to 18.5; I2: 97.4%; prediction interval: 0.1–0.3) (online supplemental material 4).
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Meta-Analysis for overall injuries incidence rate in para athletes and subgroup analysis for studies with higher and lower methodological quality.
Injury profile in para athletes
Eighteen studies found that the shoulder was the body location most frequently affected by injuries,7 22 23 26 28 30–33 39–42 44 46–48 59 mainly in sports with non-ambulant para athletes, like wheelchair basketball,22 wheelchair rugby,33 wheelchair foil fencer59 and powerlifting.26 28 In other four studies, most of the injuries occurred in upper limbs.27 52 53 61 Nine studies reported that lower limbs injuries were the most common for ambulant para athletes,24 34 36–38 43 51 58 60 and in three studies, the trunk was the most frequently injured region.35 54 55 Four studies found similar prevalence of upper and lower limb injuries,3 29 56 57 and four studies did not report injuries by body location.25 45 49 50 In general, strain, sprains and contusions were the most common injuries in para athletes.3 24 25 29 31 33–38 41 45 46 49 52 54 55 59–61 Most of the studies that included sudden and gradual onset injuries reported that sudden onset injuries are more frequent than gradual onset injuries and only one study reported similar data for gradual and sudden onset injuries.45 Between winter sports, para alpine skiing/snowboard had a higher incidence rate of injuries,39 40 while between summer sports, football 5-a-side had the highest injury incidence rates7 30 (online supplemental material 5).
Supplemental material
DISCUSSION
The purpose of this systematic review with meta-analysis was to investigate the prevalence, incidence and profile of musculoskeletal injuries, including body location, type of injury and sports with the highest number of injuries, in para athletes. Our findings showed that musculoskeletal injury prevalence in para athletes was 40.8% (95% CI 32.5% to 49.8%) and musculoskeletal injury incidence rate was 14.3 injuries per 1000 athlete-days (95% CI 11.9 to 16.8). According to the GRADE system, pooling of studies on injury prevalence in para athletes provided very low-quality evidence, and pooling of studies on injury incidence rate provided low-quality evidence. The subgroup analysis based on study sample size showed a significant lower injury prevalence (18.5%, 95% CI 12.7% to 26.1%) in studies of large sample size in comparison to studies with small sample size (58.3%, 95% CI 48.2% to 67.8%). The subgroup analysis based on methodological quality showed a significant lower injury incidence (11.7 per 1000 athlete-days, 95% CI 8.9 to 14.5) in studies of higher methodological quality as compared with studies with lower methodological quality (23.1 per 1000 athlete-days, 95% CI 17.1 to 29.2). Sudden-onset injuries were more frequent than gradual onset injuries. Strains, sprains and contusions were the most common injury type and the body regions most frequently affected were the shoulder for wheelchair athletes and the lower limbs for ambulant para athletes.
Prevalence and incidence rates of musculoskeletal injuries in para athletes are higher than in able-bodied athletes. For example, during the last summer Paralympic Games (Rio 2016), the prevalence of injuries was 12.1%,7 while in the Olympic Games in the same year it was 8%.8 Incidence of injuries followed the same pattern, with 10 injuries per 1000 athlete-days in Paralympic Games7 and 5.7 injuries per 1000 athlete-days during the Olympic Games.8 The high injury prevalence and incidence rates in para athletes show that the mechanisms of occurrence of musculoskeletal injuries in this population need to be better understood. Para athletes can be categorised in different groups, varying between para athletes with loss of muscle strength and para athletes with intellectual impairment.11 Then, these different profiles of para athletes require different approaches to treat and prevent the occurrence of musculoskeletal injuries. Furthermore, para athletes use different equipment to compete, such as a wheelchair or prosthetic devices, which increases the complexity of strategies designed to reduce injury risk.4 Sports injuries in para athletes, unlike able-bodied athletes, can also be related to their own disability or to the assistive device they use in their daily lives. For this reason, to better understand para athletes’ injuries and related factors, full knowledge of the specificities of the sport modality and the para athlete classification level are required to design and implement more individualised approaches. However, some studies still do not report this type of information.13 62 63 Although most of the included studies reported the type of disability (76%) and had injury diagnosis confirmed by a medical practitioner (70%), almost half did not provide information about the para athlete classification level or the use of assistive devices. One of the few studies that provided this information demonstrated that para athletes that did not use any assistive devices had a higher injury prevalence.48 Thus, future studies should report this information to allow better understanding on para athlete injuries profile and related factors.
The subgroup analysis showed that the estimated prevalence and incidence of musculoskeletal injuries in para athletes was influenced by the studies’ sample size and methodological quality, respectively. More specifically, studies with small sample size overestimated the injury prevalence (58.3%) in comparison to studies with large sample sizes (18.5%). For injury incidence rate, studies with higher methodological quality showed significantly lower incidence (11.7 per 1000 athlete-days) than studies with lower methodological quality (23.1 per 1000 athlete-days). This also was observed in previous systematic review with athletes with disability that reported a lower injury risk in studies with larger sample populations and higher methodological quality.13 There are fewer large competitions in para athlete sports in comparison to able-bodied sports, which may help to explain the small number of studies with appropriate sample size to estimate prevalence and incidence of musculoskeletal injuries in para athletes.64 Most of these large sample studies were performed during Paralympic games,7 29 30 39 40 which might not represent injuries rates in non-elite para athletes. Large para athletes training centres and national organisations are key to the development of future studies with large samples, high methodological quality and including prospective data collection throughout different seasons, which will provide more consistent information regarding musculoskeletal injuries in para athletes. Nevertheless, the high prevalence and incidence rates data showed by the present review highlight the need to better understand and hopefully prevent the occurrence of musculoskeletal injuries in para athletes.
The shoulder was the most affected body region in wheelchair para athletes, which can be explained by the higher demands of the upper limbs in their daily activities4 and during sports practice. Studies that assessed scapular kinematics in wheelchair para athletes demonstrated scapular asymmetries during wheelchair propulsion65 66 that, along with muscle imbalance and excessive training load, may increase the occurrence of shoulder injuries.67 68 Most of the ambulant para athletes were from sport modalities that have the highest injury incidence rates in summer Paralympic Games, such as football 5-a-side and athletics, which might help to explain why the lower limbs were the body regions most frequently affected in these para athletes.7 30 In the present review, sudden onset injuries were more frequent than gradual onset injuries. This may be related to the fact that gradual-onset injuries are often under-reported, since most of the injury definitions are based on ‘time-loss’ or ‘medical attention’13 and few studies performed a longitudinal follow-up,23 31 34 59 60 so consequently might not detect most of the gradual-onset injuries.
Our results regarding location and type of musculoskeletal injuries are in agreement with the results of non-systematic reviews.9 10 69 The heterogeneity in para sports, due to a large number of modalities and also to the different athlete classification levels for the same modality, increases the inconsistency of information about prevalence and incidence of musculoskeletal injuries in para athletes. In addition, the heterogeneity in the methods used by studies with para athletes, compromises pooling of data. One of the main problems is the different musculoskeletal injury definitions. Similar to Olympic sports, para sports also has a wide variety of injuries definition.70 As an attempt to solve this problem, the International Olympic Committee very recently established a consensus statement about methods for recording and reporting of epidemiological data on injury and illness in sport.71 A similar consensus should be developed for Paralympic sports and their specificities. Finally, most of the studies used different procedures to report prevalence and incidence rate data, did not mention a clear definition of these variables, and did not present all information used to compute these data, such as number of injuries, number of athletes injured, the total number of athletes and exposure.18 As well as data records, studies should use valid and reliable methods to assess injuries rate, such as the Oslo Sports Trauma Research Center Questionnaire on Health Problems .23 72
Weiler et al 13 conducted a systematic review of sports injuries in athletes with disabilities and also demonstrated high variability in reported injury rates. They suggested that future studies should better define injury, use standardised methods of data collection and report para athletes demographic data to improve quality of injury epidemiological data. Following these steps and focusing on para athletes specificities, future researches will allow the construction of a more consistent and robust knowledge about musculoskeletal injuries in para athletes that will allow para athletes, sport teams and institutional boards to elaborate more effective approaches to the injury in para sport problem.
This study had some limitations. First, age or level of sports participation were not defined as exclusion criteria, which allowed a wider range of included studies and consequently increased heterogeneity levels in the data. However, as studies with para athletes are less common, we had to use less restricted inclusion criteria to review data on musculoskeletal injuries in this population. Level of competition, classification levels, injury severity and type of injury might also influence on estimated prevalence and incidence rates of injuries in para athletes and were not controlled in this review. However, this was not possible because most of the studies did not report this information. The strength of the current evidence was downgraded due to imprecision, indirectness and inconsistency about injury prevalence and downgraded due to imprecision and indirectness about injury incidence rate in para athletes, presenting very low-quality and low-quality evidence, respectively.
Future high-quality studies with consistent information on the parameters used to calculate the injury prevalence and incidence rate, and valid and reliable methods for data collection are likely to impact on the estimated prevalence and incidence of musculoskeletal injuries in para athletes. To improve the quality of injury epidemiological data in para athletes, studies must properly define injury, including their type of presentation (sudden or gradual onset), severity and also follow the recommendations in the scientific literature regarding the appropriate methods to report athlete exposure and to inform about injuries risk and burden.71 In addition, studies should report para athlete’s demographic data, including type of disability, equipment used for sport practice or during daily activities, level of competition and other relevant daily demands, such as side jobs. Finally, more prospective studies that investigate the relationship between modifiable factors and injuries occurrence in para athletes, such as use of equipment and training and competition volume and intensity may form the basis for the design of more effective strategies to prevent and manage injuries in para athletes.
CONCLUSION
The reviewed studies demonstrated that musculoskeletal injury prevalence in para athletes was 40.8% (95% CI 32.5% to 49.8%) and injury incidence rate was 14.3 injuries per 1000 athlete-days (95% CI: 11.9 to 16.8). The subgroup analysis based on study sample size showed a significant lower injury prevalence in studies of large sample size as compared with studies with small sample size. For the incidence rate, studies with higher methodological quality showed a significant lower injury incidence rate in comparison to studies with lower methodological quality. Sudden-onset injuries are more frequent than gradual onset injuries in para athletes. Shoulder was the body region most commonly injured for non-ambulant para athletes, while lower limbs were the most frequently injured region for ambulant para athletes. The heterogeneity between para athletes and the poor methodological quality of the studies promote greater inconsistency in the information on the injury prevalence and incidence in para athletes. Therefore, current very low-quality and low-quality evidence suggests that prevalence and incidence rate, respectively, are likely to change with future high-quality studies, observing a large sample size, systematic data collection with reliable and validated methods and with attention to the specificities of para athletes. Findings of this systematic review demonstrate that para athletes, sports teams and para sport institutional boards should be aware of the high prevalence and incidence levels of musculoskeletal injuries in para athletes.
What is already known
The heterogeneity in para sports increases the inconsistency of information about prevalence and incidence of musculoskeletal injuries in para athletes.
There is still a need for consensus on epidemiological research methodology, including sports injury definition in para sports.
In para athletes, shoulder is the most frequently affected body location by injuries in non-ambulant para athletes, and lower limbs injuries are the most common in ambulant para athletes.
What are the new findings
This was the first systematic review with meta-analysis on injury prevalence and incidence in para athletes that uses Grading of Recommendations Assessment, Development and Evaluation recommendations to assess the overall quality of evidence.
The subgroup analyses revealed that the sample size influenced the estimated injury prevalence and methodological quality influenced the injury incidence rate.
Between winter sports, para alpine skiing/snowboard had the highest incidence of injuries, while between summer sports, football 5-a-side had the highest incidence of injuries.
Ethics statements
Patient consent for publication
Acknowledgments
The authors thank the support given by Secretaria Especial do Esporte do Ministério da Cidadania (Governo Federal, Brasília, Brazil—protocol number 58000.008978/2018-37), Comitê Paralímpico Brasileiro (CPB), CTE/EEFFTO/UFMG, FEPE-UFMG (Fundação de Apoio ao Ensino, Pesquisa e Extensão-UFMG), Pró-Reitoria de Pesquisa (PRPq)—UFMG.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Evertverhagen
Contributors All authors were fully involved in the study and preparation of the manuscript and agreed with the content in the final manuscript.
Funding Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq)—428735/2018-5, Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG)—CDS - APQ-01017-17, Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.