Article Text

Abstract
Objective Muscle injury is one of the most common injuries occurring at the Olympic Games often with devastating consequences. Epidemiological injury surveillance is recognised by the IOC as essential for injury prevention and management. We aimed to describe the incidence, anatomical location and classification of MRI-detected muscle injuries in athletes who participated in the Tokyo 2020 Olympic Games.
Methods Two board-certified orthopaedic surgeons, highly experienced in reviewing MRIs, independently and retrospectively reviewed all MRIs collected at the Tokyo 2020 Olympic Games from clinical reports generated by board-certified musculoskeletal radiologists at the IOC Polyclinic. The presence and anatomical site of muscle injuries were classified as: type a: myofascial/peripheral; type b: muscle belly or musculotendinous junction; and type c: injury which extends into the tendon, with reference to the British Athletics Muscle Injury Classification.
Results Fifty-nine MRI-detected muscle injuries were seen in 40 male and 19 female athletes. 24 athletes (41%) were unable to fully compete in their event. Fifty-two injuries (88%) involved lower extremity muscles with hamstring muscle injuries most common (32 of 59, 54%). Half of all muscle injuries occurred in athletes participating in athletics (30 of 59, 51%). 21 athletes (35%) sustained type a injuries, 14 athletes (24%) type b injuries and 24 athletes (41%) type c injuries. Of athletes with type c injuries, 18 (75%) did not complete their competition, a rate significantly higher than types a and b (OR 14.50, 95% CI 4.0 to 51.9, p<0.001).
Conclusion For athletes sustaining muscle injuries during the Olympic Games, our study demonstrates the prognostic relevance of muscle injury anatomical site and severity for predicting completion or non-completion of an Olympic athlete’s competition.
- muscle
- epidemiology
- Magnetic Resonance Imaging
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Epidemiological surveillance of injuries at Olympic events, including MRI-detected muscle injury data from the IOC Polyclinic in the Rio de Janeiro 2016 Summer Olympic Games, has shown that muscle injuries are a frequently experienced sports-related injury. To advance the epidemiological surveillance objectives of the IOC toward the improvement of prevention and treatment strategies, injuries must be examined in detail.
WHAT THIS STUDY ADDS
Our study identified 59 MRI-detected muscle injuries and showed that athletes who sustained muscle injuries extending into the tendon were less likely to complete their competitions than athletes whose muscle injuries did not extend into the tendon.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These results indicate that diagnosis of anatomical site and severity of muscle injuries using MRI may meaningfully inform decisions regarding continuation of competition for Olympic athletes.
Introduction
Muscle injury is one of the most commonly seen sport-related injuries in elite athletes.1–3 Elite athletes who suffer muscle injury experience decreased performance and require time off from training and competition.4 5 The risk of injury intensifies during infrequent, high-stakes sporting events at high levels of competition, with arguably the highest risk during the Olympic Games.6–8 These injuries represent a major challenge for both Olympic athletes and medical support staff with regard to prevention, prognosis and management strategies during the Games. Conducting epidemiological surveillance of sports injuries including muscle strain incidence is the fundamental first step in the sequence of evidence-based injury prevention strategies.9 10
The Olympic Games is the world’s largest sporting event with up to 10 000 participating athletes of multiple sports from more than 200 countries. This provides the most heterogeneous study cohort of elite athletes, and an opportunity to contribute to the optimisation of athletes’ performance. Injury surveillance reports from the Olympic Games serve an important role in injury prevention in high-level athletes and have been continuously published since the London 2012 Summer Olympic Games.11 12 These epidemiological reports help direct appropriate medical care and optimise the health of athletes, as well as promote a positive legacy throughout the world, which are fundamental missions of the IOC.13 Surveillance studies of muscle injury in elite athletes have been performed in several single-sport events.14–16 However, to our knowledge, only limited published data are available specifically for muscle injuries in the Olympic Games.17
The aim of our study was to describe the incidence, the anatomical location, and the classification of MRI-detected muscle injuries and competition completion results stratified by muscle injury site in athletes who participated in the Tokyo 2020 Olympic Games.
Methods
This is a retrospective study of imaging data collected at the Tokyo 2020 Olympic Games from the Radiological Information System and Picture Archiving and Communication System at the Polyclinic. All new or acute MRI-detected injuries were included. Two injuries in two athletes were excluded as MRI was used to monitor treatment for their minor injuries sustained months prior to the Olympic Games.
Data collection
Consistent information was retrieved for all athletes treated for injuries and illnesses in the Polyclinic operated by the Tokyo Organizing Committee of the Olympic and Paralympic Games medical staff. These data were collected through an electronic medical records system (GE AMS, GE Healthcare, Hungary). Medical and imaging services were open for 30 days, from the opening of the Olympic Village on 13 July 2021 to the closing of the Olympic Village on 11 August 2021, at the IOC Polyclinic situated within the Olympic Village.
Diagnostic imaging was performed at the IOC Polyclinic within the Olympic Village using 1.5T MRI scanners (Signa Explorer and Signa Voyager, GE Healthcare, Chicago, USA). All musculoskeletal MRI referrals were ordered by board-certified orthopaedic physicians through the electronic medical records system at the IOC Polyclinic. MRI protocols consisted of fluid-sensitive images (always including fat-suppressed proton density weighted) and T1-weighted images with three-plane acquisition.
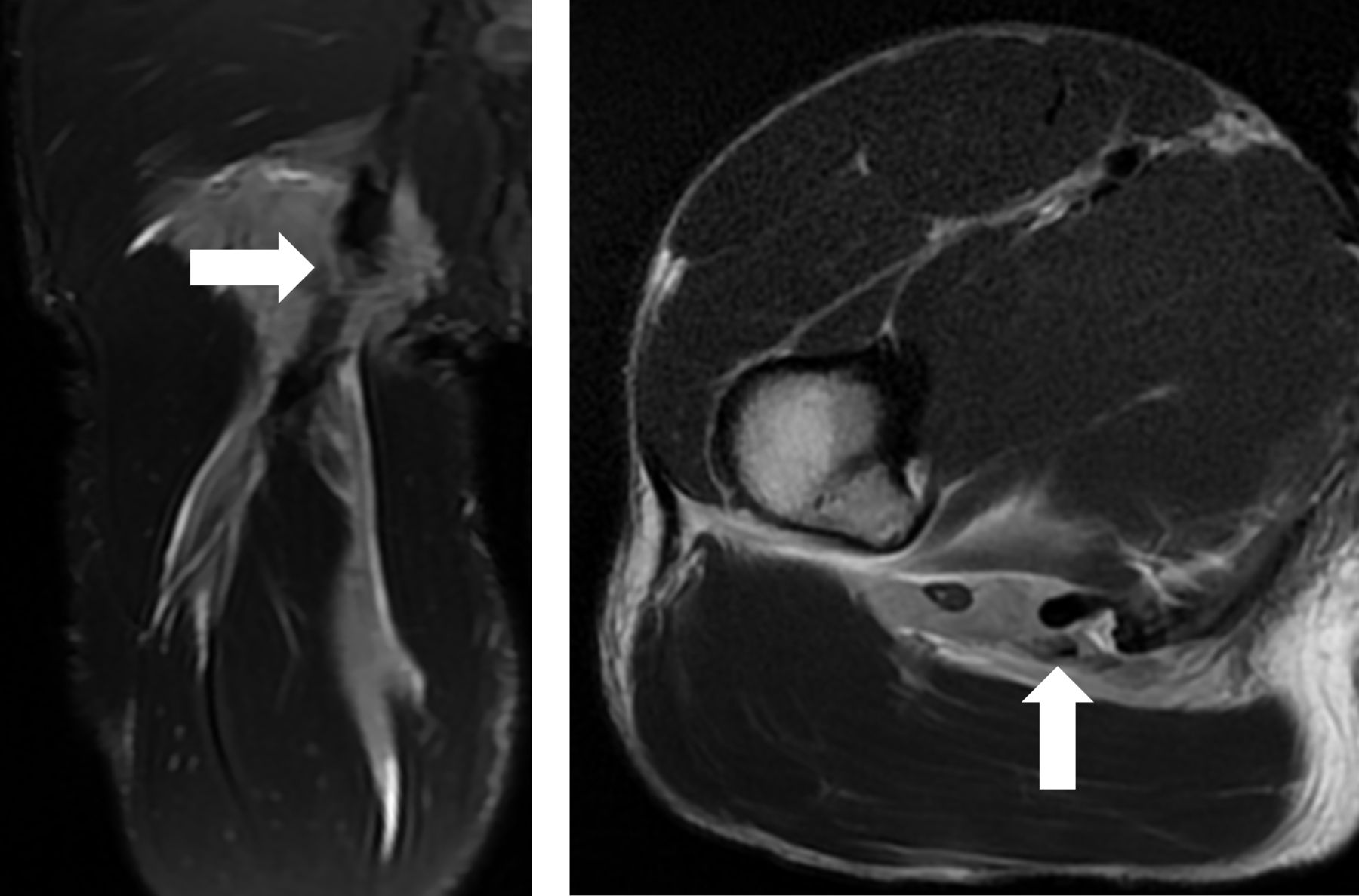
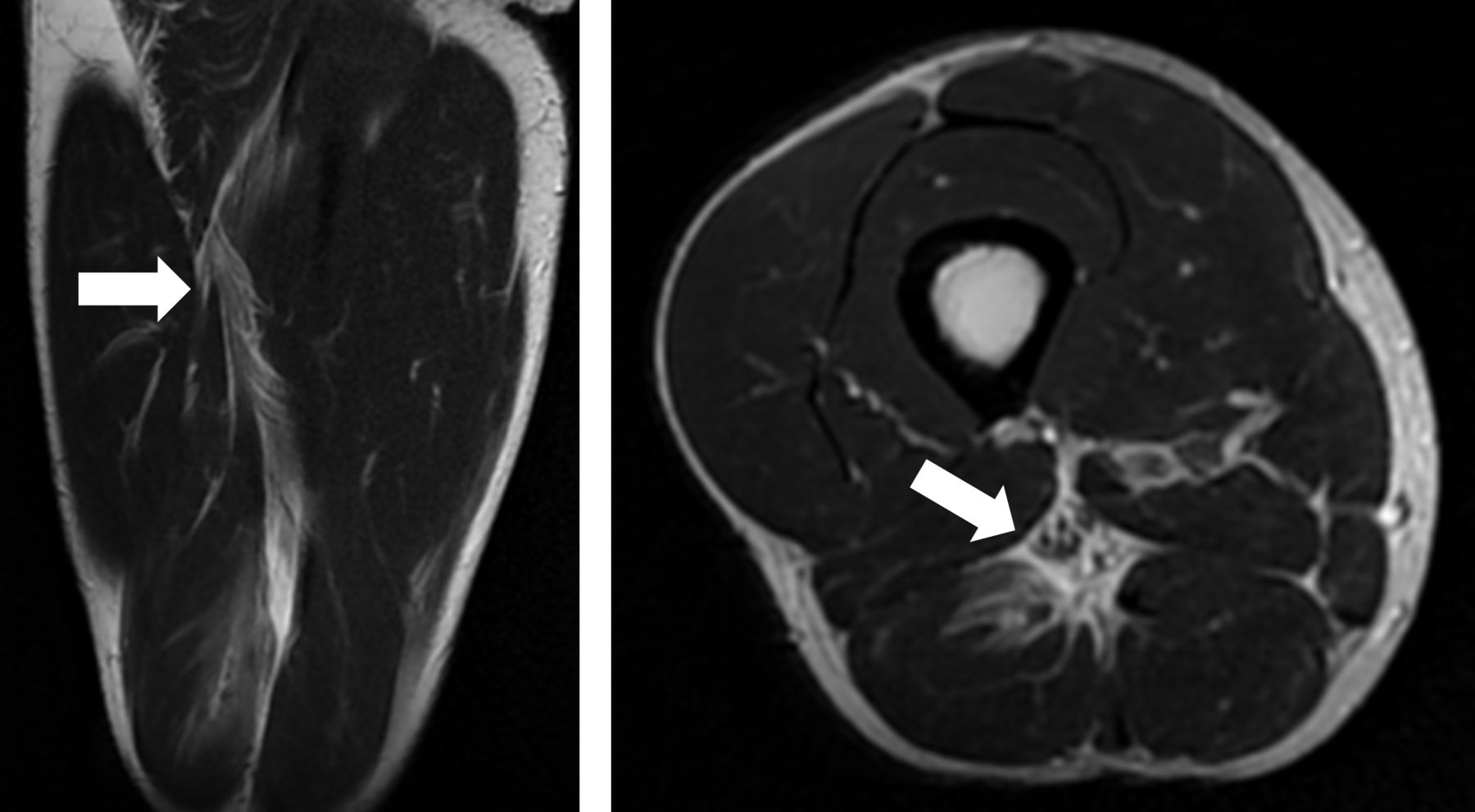
Muscle injury records were retrospectively collected by an orthopaedic surgeon (HKa) from the electronic medical records containing the original clinical reports generated by the Japan Radiological Society board-certified musculoskeletal radiologists at the official IOC Polyclinic. Two board-certified orthopaedic surgeons (HKa and J-SA with 17 and 9 years of experience in reviewing MRIs, respectively) were instructed prior to this analysis regarding muscle injury classification on MRIs by a board-certified musculoskeletal radiologist with 7 years of experience in musculoskeletal imaging analysis (TA). These two surgeons (HKa and J-SA) then independently and retrospectively reviewed all MRIs for the presence and severity of muscle injuries, specifically for the purposes of this study. The injury location was defined by isolating the specific muscle or the muscle exhibiting the greatest extent of injury on MRIs. The anatomical site classification of each muscle injury was determined with reference to the British Athletics Muscle Injury Classification (BAMIC)18 19 as follows: type a: myofascial injury in the peripheral aspect of the muscle (figure 1); type b: an injury within the muscle belly, most commonly at the musculotendinous junction (figure 2); type c: an injury which extends into the tendon (figure 3), with incomplete rupture and complete rupture separately noted. However, in this surveillance study, the BAMIC injury size scale (0–4) was not used in the evaluation of muscle injuries. Any discrepancies in anatomical site classification of muscle injuries between readers were adjudicated by means of consensus agreement between the readers with advice from a board-certified musculoskeletal radiologist. Demographic information was collected for all athletes diagnosed with muscle injuries on MRI in an anonymised fashion from the electronic medical record system at the Polyclinic. Competition results of athletes diagnosed with muscle injuries in the Tokyo 2020 Olympic Games were collected from the official IOC website (https://olympics.com/en/olympic-games/tokyo-2020).
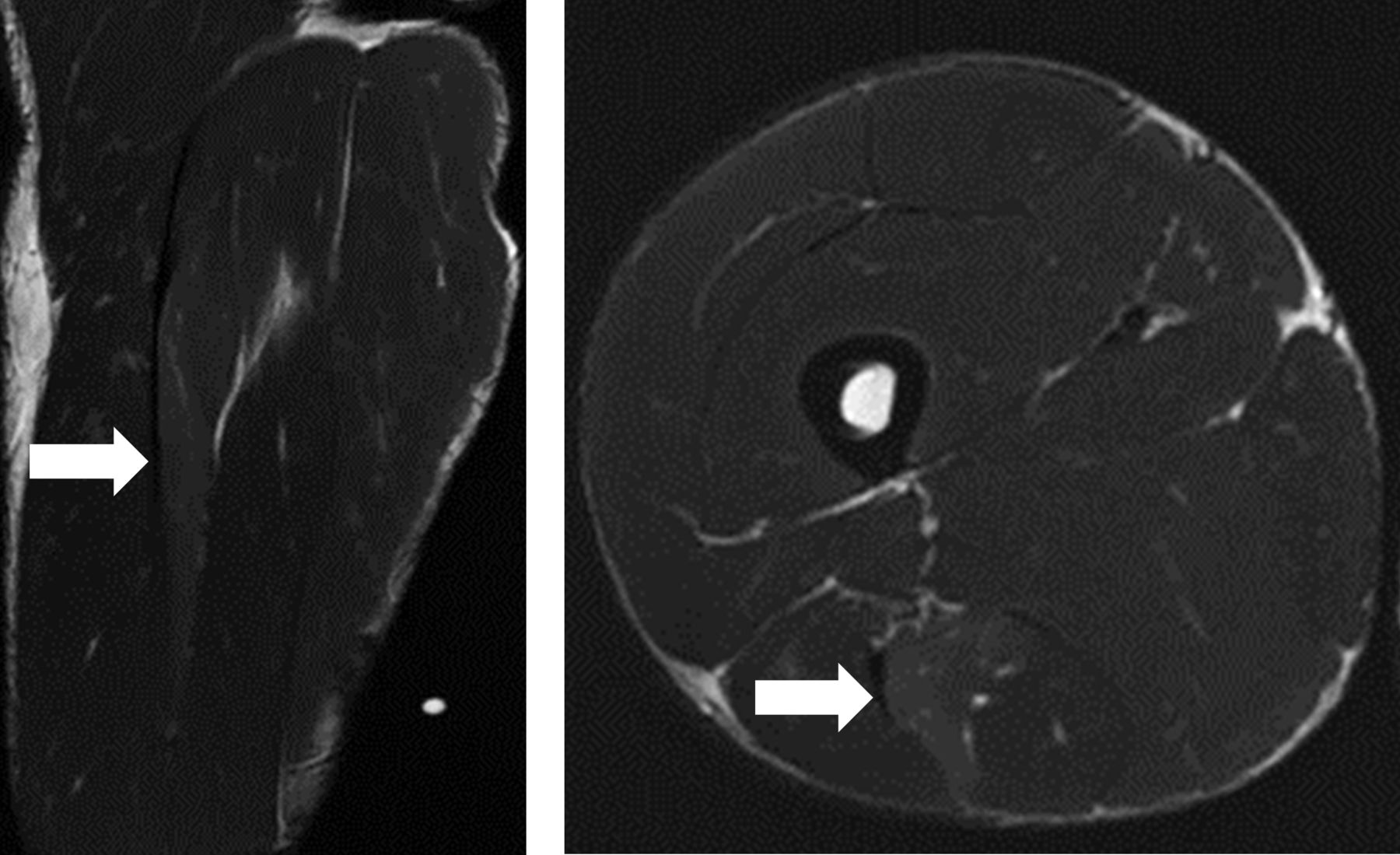
Olympic athlete participating in sprint race (24-year-old man). Coronal and axial T2-weighted image demonstrates a myofascial injury in the peripheral aspect of the muscle at semimembranosus. This injury was consistent with type a (arrow).

Basketball player (28-year-old man). Coronal and axial T2-weighted image demonstrates an injury within the muscle belly at the musculotendinous junction of biceps femoris (arrow). This injury was consistent with type b.
{kind=link}
{kind=link}
{kind=link}
Olympic athlete participating in long jump (24-year-old man). Coronal and axial T2-weighted fat-suppressed proton density weighted image demonstrates rupture of the biceps femoris and semitendinosus conjoint tendon (arrow). This injury was consistent with type c.
Statistical analysis
Statistical analyses were performed using SPSS V.25.0. The IOC provided the number of athletes registered for the Tokyo 2020 Olympic Games. The incidence of muscle injury for each of the various categories such as male/female, age, right and left side (see tables), and the rate of athletes who did not complete between type c versus types a and b, were determined by dividing the number of muscle injuries by the number of participants in each category. The Χ2 test was then used to compare the incidence proportions between the categories, with p values of <0.05 considered statistically significant. Data were expressed as number of muscle injuries.
Results
Our review of images and medical records found 59 MRI-detected muscle injuries, summarised in table 1. A total of 40 male athletes and 19 female athletes suffered muscle injuries. The incidence of muscle injury in male athletes was higher than in female athletes (OR 1.944; 95% CI 1.124 to 3.361, p=0.022). The median age of athletes who sustained muscle injuries was 27 years old (range 19–37 years). No age-related difference in muscle injury incidence was found (p=0.999). Athletes from Europe incurred the highest number of muscle injuries with 18 cases, followed by 16 athletes from America. The injury incidence proportion was high among athletes categorised as refugees, athletes from Oceania and athletes from Africa, at 3.45%, 1.16% and 0.82%, respectively. However, as there were only 29 athletes categorised as refugees, a single injury caused an apparently very high 3.45% incidence proportion, which is unlikely to be reliable.
Demographics of athletes who sustained muscle injuries at the Tokyo 2020 Olympic Games
Body region and circumstances of injury
No difference was found between the frequency of injuries on the left side (30 cases) and injuries on the right side (29 cases; table 2). Fifty-two injuries (88%) affected muscles of the lower extremities. Information on the circumstances of injury was available in the medical records for 52 injuries (88%). Fifty-one per cent of muscle injuries occurred during competition and 32% during training, whereas 5% occurred during daily activities. Thirty-five (59%) athletes completed their competitions, while 24 athletes (41%) did not complete their entire competitions. Fifty-four injuries (92%) occurred during the Olympic Games period.
Characteristics of muscle injuries at the Tokyo 2020 Olympic Games
Incidence of muscle injuries by type of sports
Table 3 summarises incidence number and incidence proportion of muscle injuries by type of sport. Muscle injuries most commonly occurred in athletics (n=30, 17 short-distance runners, 5 middle-distance runners, 5 jumpers, 2 throwers, 1 decathlon), followed by field hockey (n=6). The highest incidence proportion of muscle injuries by sport category was 1.5% in athletics and field hockey.
Incidence of muscle injuries for each sport in the Tokyo 2020 Olympic Games
Anatomical region and specific muscles injured by type of sports
The anatomical regions and specific muscles injured were listed by sport (table 4). In athletics, all muscle injuries were in the lower extremity, except for one injury of an external abdominal oblique in a javelin thrower. All 17 sprinters sustained muscle injuries in the proximal lower extremity muscles related to knee flexion or hip extension (eight biceps femoris, seven semimembranosus, one semitendinosus, one sartorius). In field hockey, injuries in four hamstring muscles were sustained, one obturator externus and one adductor brevis.
Anatomical location of muscle injuries by sport in the Tokyo 2020 Olympic Games
Biceps femoris injuries were the most common with 24 injuries: 14 occurring in athletics, 4 in field hockey, 2 in football, 1 in basketball, 1 in handball, 1 in wrestling and 1 in weightlifting. Semimembranosus injuries accounted for seven injuries in athletics. Five rectus femoris injuries occurred, with two in tennis, one in athletics (javelin thrower), one in volleyball and one in football. One upper extremity muscle injury occurred each in weightlifting and softball. Muscle injuries in the shoulder were seen in handball (1) and gymnastics (1).
Anatomical site classification of muscle injuries on MRI assessment
Twenty-one injuries (35%) were myofascial injuries in the peripheral aspect of the muscle (type a), 14 injuries (24%) involved the muscle-tendon junction (type b) and 24 injuries (41%) which extend into the tendon (type c) (table 5). Of those 24 type c injuries, 3 were complete rupture.
MRI assessment of muscle injury site by anatomical location in the Tokyo 2020 Olympic Games
Type c muscle injuries were seen in 50% of biceps femoris muscle injury cases. Type c muscle injuries were seen in four of seven semimembranosus muscle injury cases. In athletics, 15 athletes (50%) suffered type c muscle injuries including 2 complete tears (table 6). One fencing athlete suffered a type c muscle injury with complete tear in the gracilis muscle. In sport disciplines including football, tennis, softball, equestrian, volleyball, aquatics, gymnastics and judo, all MRI-depicted muscle injuries were type a or b.
Muscle injury site by sport in the Tokyo 2020 Olympic Games
Regarding age, the median age of athletes who sustained type c muscle injuries was 27.6 years old (range 20–37 years). The median age of athletes who sustained type a or b muscle injuries was 27.0 years old (range 19–37 years). There was no significant difference in the ages between athletes who sustained type c muscle injuries and those who sustained other type a or b muscle injuries (p=0.645).
Competition results stratified by muscle injury site classification
Sixteen athletes (76%) who sustained type a muscle injuries completed their competitions, while four athletes did not start their competitions and one athlete was disqualified (table 7). All athletes except one who sustained type b muscle injuries (93%) completed their competitions. Eighteen of 24 athletes (75%) with type c injuries did not complete their competitions. The rate of athletes who did not complete in type c was significantly higher than in types a and b (17%, 6 of 35) (OR 14.50; 95% CI 4.0 to 51.9, p<0.001).
Competition completion results stratified by muscle injury site
Discussion
Muscle injuries represent a significant proportion of injuries in elite athlete competitions across a variety of sports.20–25 In our analysis of the Tokyo 2020 Games, we report 59 MRI-detected muscle injuries in elite athletes who competed in and who were comprehensively surveyed using imaging data and medical records collected at the IOC Polyclinic.
Injury incidence is greater at higher-stakes infrequent events than at lower-stakes annual events.8 It is not surprising that a higher incidence of muscle injury would therefore be seen at the Olympic Games, which include multiple sports and are high-stakes infrequent events. The epidemiological surveillance of muscle injuries during the Olympic Games is an extension of the efforts of previous studies reporting data during single-sport events. In the Athens 2004 Olympic Games, injuries in eight team sports (soccer, handball, basketball, field hockey, baseball, softball, water polo and volleyball) were surveyed and 35 muscle injuries were reported.26 In the London 2012 Summer Olympic Games, injuries that prevented athletes from participating in competition or training for more than a week were surveyed and 38 muscle injuries were reported.11 In the Rio de Janeiro 2016 Summer Olympic Games, Crema et al 17 used imaging data collected at the IOC Polyclinic within the Olympic Village and reported 81 muscle injuries. We detected a similar number of muscle injuries sustained at the Tokyo Olympic Games.
Characteristic injury patterns were observed in the distribution of muscle injuries in Olympic athletes between the sexes, across the sports disciplines, and in anatomical regions and muscles injured. Male athletes had a statistically higher incidence proportion of muscle injury than female athletes. Of all the sport disciplines, the highest incidence of muscle injuries was found in athletics and the majority of those were in the lower extremities. Muscle injuries of the lower extremities most commonly involved the biceps femoris and semimembranosus.
Sex-related differences in muscle injury risk in athletics have been previously reported.27–29 Male athletes suffered more muscle strains and muscle cramps than female athletes during athletics championships in the Daegu 2011 International Association of Athletics Federations World Championships.27 The incidence rates of muscle injuries among men and women per 1000 registered athletes were 28.6±7.6 and 13.0±5.2, respectively. Surveillance of muscle injury during 14 international championships was conducted from 2007 to 2014 to extend previous studies of single athletics championships.29 In that study, male athletes incurred significantly more muscle injuries than female athletes and the relative risk was 1.64 (95% CI 1.33 to 2.04). In our study of the Tokyo 2020 Summer Olympic Games, 5423 female athletes and 5892 male athletes competed, of which a total of 19 female athletes (0.35%) and 40 male athletes (0.68%) suffered muscle injuries (OR 1.944; p=0.022).
For elite athletes registered for international athletics championships, muscle injury is the most common type of injury, constituting 40.9% of all recorded injuries.30 Athletics exhibited the largest number and the highest incidence rates of muscle injury of all sports in the Tokyo 2020 Olympic Games. Similarly, during the Rio de Janeiro 2016 Summer Olympic Games, 39 athletes in athletics sustained muscle injuries, and the incidence rate for muscle injury reached 1.64%.17 Both in the Rio de Janeiro 2016 Summer Olympic Games and in the Tokyo 2020 Olympic Games, the majority of muscle injuries affected sprinters in athletics (64% and 57%, respectively).
In field hockey, a systematic review found that muscle injury is one of the most frequent injury types.31 In competition, muscle injury rates in collegiate female athletes have been previously reported at 0.66–0.96 per 1000 athlete-exposures.32 33 The incidence rate could not be directly compared because of the considerable methodological heterogeneity between studies. During 2004 Olympic Games, which held 42 matches, three men suffered muscle injuries.26 During the Rio de Janeiro 2016 Summer Olympic Games, no muscle injuries were reported in field hockey.17 In the Tokyo 2020 Olympic Games, which held 76 matches, field hockey had the second largest number (four men and two women) and the second highest incidence rate of muscle injuries of all sports. On the other hand, in comparison with Rio de Janeiro 2016 Summer Olympic Games, muscle injury in football, weightlifting, and rugby decreased from 9, 5, and 4 to 3, 2 and 0 in the Tokyo 2020 Olympic Games. This considerable disparity of results demonstrates why it is not possible to draw conclusive findings on injury rates from just one tournament.
The anatomical region and muscles most injured in the current study involved the hamstrings (55.9%), especially in short-distance runners (100%, 17 of 17). The previous study of the Rio de Janeiro 2016 Summer Olympic Games found a similar distribution with 46.2% in the hamstrings, and higher in short-distance runners (60%).17 Similarly, during 13 international athletics championships, muscle injury of the thigh in all disciplines and in short distance was 68.3% and 74.5%, respectively.34 Additional data analyses have shown an increase in the proportion of hamstring muscle injuries with increasing running velocity elicited by the disciplines.35 Other differences observed with regard to sports categories are shown in table 5.
Muscle injuries extending into the tendon (type ‘c’ injuries) are associated with longer recovery times and are considered to be more serious injuries in athletes.19 36 Whether or not a muscle injury involves the tendon is assessed in determining the severity of muscle injuries in the BAMIC system.18 Using this classification system, muscle injuries extending into the tendon (classified as type ‘c’) were noted in 13 (21.3%) of 61 hamstring muscle injuries in elite-level male football players at an English Premier League club between August 2011 and June 2019 as per an electronic medical record system maintained by the club.37 In elite male football players, time to return to full training after type c muscle injury is significantly longer with significantly higher reinjury rate compared with type a and b injuries. The sport incurring the most type c muscle injuries was athletics in the Tokyo 2020 Summer Olympic Games; however, we could not find a report on the distribution of injuries by anatomical site and by sport in any other Summer Olympic Games. In elite track and field, MRI-detected muscle injuries classified as type c were found in 13 of 54 athletes in the British Athletics World Class Programme between 2015 and 2019.38
Limitations
There were some limitations in the present study. First, the potential underestimation of muscle injuries cannot be entirely ruled out as we did not have access to data from participating teams’ own medical set-ups (eg, ultrasound by team physician (National Olympic Committee doctors)), nor to athletes who did not come to the Polyclinic and who may have sought treatment later after leaving Japan. With respect to our review of all electronic medical records, we did not include 12 injuries identified by ultrasound alone (6 in athletics, 2 in volleyball, 1 in field hockey, 1 in basketball, 1 in gymnastics, 1 in table tennis). More data could have been obtained through an athlete questionnaire, but this was not possible as the IOC strongly encourages athletes to focus on their preparation and competition. Second, we evaluated muscle injuries using only anatomical site classifications (a, b, c) from the BAMIC without using that system’s size classifications (0–4).18 19 Future studies are needed to examine the relationship between injury size and injury site classification, and the prognostic relevance of both. Third, sample sizes were not sufficient to draw conclusions regarding any epidemiological trends from one event to the next. In fact, disparities were found between the current results and the results from Rio de Janeiro 2016 in some analyses. Continuous surveillance and analysis of successive Olympic Games will be needed to obtain more detailed evaluation of findings.
Conclusion
While expanding the body of data from previous studies for the advancement of the epidemiological surveillance objectives of the IOC, our study demonstrates the possible prognostic relevance of anatomical site and severity of muscle injury for predicting the completion or non-completion of an Olympic athlete’s competition.
What are the new findings?
Fifty-nine MRI-detected muscle injuries were reported during the Tokyo 2020 Summer Olympic Games. Muscle injuries occurred more commonly in male athletes, mostly in the lower extremities, especially biceps femoris and semimembranosus, and most commonly in athletics.
Forty-one per cent of muscle injuries depicted on MRI involved muscle injury which extends into the tendon.
A significantly higher rate of non-completion was seen in athletes with muscle injury which extends into the tendon than in athletes with muscle injury which does not extend into the tendon.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
An Institutional Review Board (IRB) approval was obtained from Tokyo Medical and Dental University (research protocol identification: M2021-048). All images and demographic data were treated with strict confidentiality and data protection in de-identified fashion during data collection, storage and analysis. Informed consent was waived because all data in our epidemiological study were anonymised such that individuals were unidentifiable. The IOC approved our use of anonymised imaging and demographic data for publication.
Acknowledgments
The authors would like to thank IOC members, Olympic Village imaging centre staff, sports physicians/radiologists who provided clinical service, and Vern Fischer for English language editing.
References
Footnotes
Contributors HKa designed the initial plan, conducted the study and completed the final manuscript. J-SA and TA analysed the data and drafted the manuscript. BBF, LE and HKo designed the initial plan, conducted the study and edited the manuscript. YS and KO collected the data. All authors read and approved the final manuscript. Hko is responsible for the overall content as the guarantor. HKo accepts full responsibility for the work and the conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KO receives royalties from Springer Co for a book titled 'Tendinopathy'.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.