Article Text

Abstract
Objectives To estimate the risk of clinically diagnosed knee osteoarthritis (OA) after different types of knee injuries in young adults.
Methods In a longitudinal cohort study based on population-based healthcare data from Skåne, Sweden, we included all persons aged 25–34 years in 1998–2007 (n=149 288) with and without diagnoses of knee injuries according to International Classification of Diseases (ICD)-10. We estimated the HR of future diagnosed knee OA in injured and uninjured persons using Cox regression, adjusted for potential confounders. We also explored the impact of type of injury (contusion, fracture, dislocation, meniscal tear, cartilage tear/other injury, collateral ligament tear, cruciate ligament tear and injury to multiple structures) on diagnosed knee OA risk.
Results We identified 5247 persons (mean (SD) age 29.4 (2.9) years, 67% men) with a knee injury and 142 825 persons (mean (SD) age 30.2 (3.0) years, 45% men) without. We found an adjusted HR of 5.7 (95% CI 5.0 to 6.6) for diagnosed knee OA in injured compared with uninjured persons during the first 11 years of follow-up and 3.4 (95% CI 2.9 to 4.0) during the following 8 years. The corresponding risk difference (RD) after 19 years of follow-up was 8.1% (95% CI 6.7% to 9.4%). Cruciate ligament injury, meniscal tear and fracture of the tibia plateau/patella were associated with greatest increase in risk (RD of 19.6% (95% CI 13.2% to 25.9%), 10.5% (95% CI 6.4% to 14.7%) and 6.6% (95% CI 1.1% to 12.2%), respectively).
Conclusion In young adults, knee injury increases the risk of future diagnosed knee OA about sixfold with highest risks found after cruciate ligament injury, meniscal tear and intra-articular fracture.
- knee injuries
- knee ACL
- meniscus
- fracture
- osteoarthritis
Statistics from Altmetric.com
INTRODUCTION
Osteoarthritis (OA) is a chronic musculoskeletal disease that frequently affects the large weight-bearing joints and may eventually lead to the need for total joint replacement.1 Important known risk factors for knee OA are older age, overweight or obesity, female sex, high physical occupational load and joint injury.2–4 Knee injury that occurs in adolescence and young adulthood is an important risk factor for the development of knee OA.5–7 However, the majority of studies that investigate knee injury as a risk factor typically include middle-aged or older populations and are based primarily on retrospective analyses.6 Consequently, those relying on self-report of previous knee injury may be susceptible to recall bias and may overestimate the association between injury and OA. Another way that the association between knee injury and OA can be overestimated is through misclassification of the injury. For example, if patients report pain associated with normal activities as injury, when it was actually early knee OA. Because large prospective studies on this topic are scarce, the magnitude of risk in the younger population is still unclear.5 6 Within 10–20 years after a specific knee injury of the anterior cruciate ligament (ACL) and/or a meniscal tear, on average half of all persons have been reported to develop radiographic knee OA.8 9 Thus, these patients may already experience an ‘old’ knee while they are still relatively young.8 10 Further, apart from cruciate ligament injury and meniscal tears, it is currently unclear how other knee injuries with different spectrum of exposure severity that occur at a young age influence the risk for knee OA, for example, fractures of the patella or the tibia plateau, a collateral ligament sprain or dislocation of the patella.6 11 Also, it is unknown whether the time to develop clinically evident knee OA at a young age differs between injured and uninjured persons. Therefore, the aims of this study were to assess the relative and absolute risk of clinically diagnosed knee OA after different types of knee injuries versus those without a diagnosis of knee injury. Supplementary, among those who develop knee OA at young age, we estimate the loss of time free from knee OA due to knee injury.
Methods
Study design
We used a longitudinal cohort design based on healthcare consultations to a physician in primary, specialist and inpatient care in the entire population of Skåne, the southernmost region of Sweden (population of 1.3 million). Data sources included the Skåne Health Register (SHR) from 1998 up to 2017, the population register and Statistics Sweden. In the SHR, all public and private inpatient and outpatient healthcare consultations are entered, including information on the personal identifier, date of visit, healthcare provider, and since 1998 diagnoses set by publicly practicing physicians according to the 10th version of the International Classification of Diseases (ICD-10) system. We used the population register to determine residential status, and Statistics Sweden to obtain sociodemographic data.
Study procedure and participants
Eligible participants were residents in the Skåne region between 1998 and 2007, with at least one healthcare visit during the years of 1999 and 2007, at age 25–34 years and with at least one diagnostic code registered. Persons were included from 25 years of age because from that age it was plausible to develop clinically evident OA within our follow-up time. Persons diagnosed with knee injury during the year 1998 were excluded to remove persons with ‘prevalent’ injuries. The exposed cohort comprised persons with a newly diagnosed knee injury between 1 January 1999 and 31 December 2007 defined as a relevant ICD-10 diagnostic code assigned by the physician (online supplementary appendix, table 1). The date of diagnosis was set as the index date. The reference subjects comprised persons without knee injury, and a random healthcare visit from the same time period was sampled as index date. The outcome, incident knee OA, was defined as an ICD-10 code (M17) registered at a visit to a physician up to the year 2017. The M17 code for knee OA had a high positive predictive value of 88%.12 We excluded all subjects, both exposed and unexposed, if they were diagnosed with knee OA (M17), or with derangement of meniscus due to old tear or injury (M23.2), or with follow-up examination after treatment for conditions other than malignant neoplasms (Z09), during 1 year preceding the index date. Each included person had at least 10 years of potential follow-up time from index date to diagnosis of knee OA, emigration, death or the 31 December 2017, whichever occurred first. To control for surveillance bias, in that additional diagnostics for subjects with knee injury increases the probability to be diagnosed with knee OA, we excluded the persons diagnosed with knee OA in the first 3 years of follow-up.13
Supplemental material
Statistical analysis
To describe the baseline characteristics of the injured and uninjured reference subjects, we provide descriptive statistics of the study sample, follow-up time and cumulative incidence of the outcome. The Cox proportional hazards regression model was used to estimate the HR of knee OA after knee injury as compared with the general population (who consulted healthcare but without injury). This analysis was adjusted for age, sex, residential area, educational attainment and income preceding the index date and was stratified on index year. Age at the start of inclusion was modelled as a continuous variable (in years), as we found no evidence of any non-linearity. Income, as expected, had a heavily skewed distribution, and we categorised it into six groups using cut-off points of 10th, 25th, 50th, 75th and 90th percentile of its distribution. Residential area, educational attainment and income were modelled as categorical variables. Because we had no information on body mass index (BMI) from the register, as a surrogate the model was also adjusted for diagnosis of diabetes (type I or II, ICD-10 codes E10, E11, E14), obesity (E65, E66) and hypertension (I10, online supplementary appendix, figure 1). By stratifying on index year, we ensured that both injured and uninjured persons had the same length of assessment of comorbidities and the same potential follow-up time. We consider the variables adjusted for as being also sufficient to adjust for possible selection bias due to censoring. We assessed the assumption of proportionality with Schoenfeld residuals plots and log-log plots (online supplementary appendix, figure 2). Due to non-proportionality of hazards, we presented interval-specific estimates for 0–11 years of follow-up and 12–19 years of follow-up separately. We fitted a similar model with specific type of injury as exposure (contusion, fracture, dislocation, meniscal tear, collateral ligament tear, cruciate ligament tear, injury to multiple structures and other/cartilage tear) to further estimate the HRs on the development of knee OA. We combined cartilage tear (S83.5) with other strain (S83.6) due to low numbers per category.
In addition to HR, we estimated risk differences (RD) to provide an estimate of the excess risk of knee OA in absolute terms. We also estimated the difference in restricted mean survival time to incident knee OA between the injured and uninjured persons during the 19 years postindex date. To estimate the RDs and restricted mean time to knee OA, we used the pseudo-observation method for regression analysis of the censored time to event data and adjusted for the same confounders as in the Cox model.14 We excluded two persons from this pseudo-observation analysis who developed OA at the end of follow-up when a low number of people were at risk, but who had large influence on both point estimates (ie, increase them) and width of the CIs.
We prespecified two potential effect modifiers: age at time of injury and sex. We dichotomised age at the sample median (≤30 years/>30 years) and presented results stratified by age group and sex.
We performed one sensitivity analysis, where we included the additional diagnoses of cruciate ligament injuries and meniscal tears that were reported within 90 days of the primary injury diagnosis. This differs from the multiple structures diagnosis that was given by the physician if more than one structure in the knee was affected, that is, without specifying the exact combination of injuries. We did this to limit potential misclassification of the injury type and assess potential coexistence of meniscal and cruciate ligament injury. For all estimates, 95% CIs were calculated. As we expected a high number of events in the health register data and were able to include the whole underlying population without additional costs, we did not perform a formal sample size calculation prior to conducting this study. Analyses were performed in STATA (V.15) and in RStudio statistics program (V.3.5.1).
Patient and public involvement
Patients were not involved in this research to comment on the study design or interpret the results. Patients were not invited to contribute in the writing or editing of the manuscript.
Results
Descriptive statistics
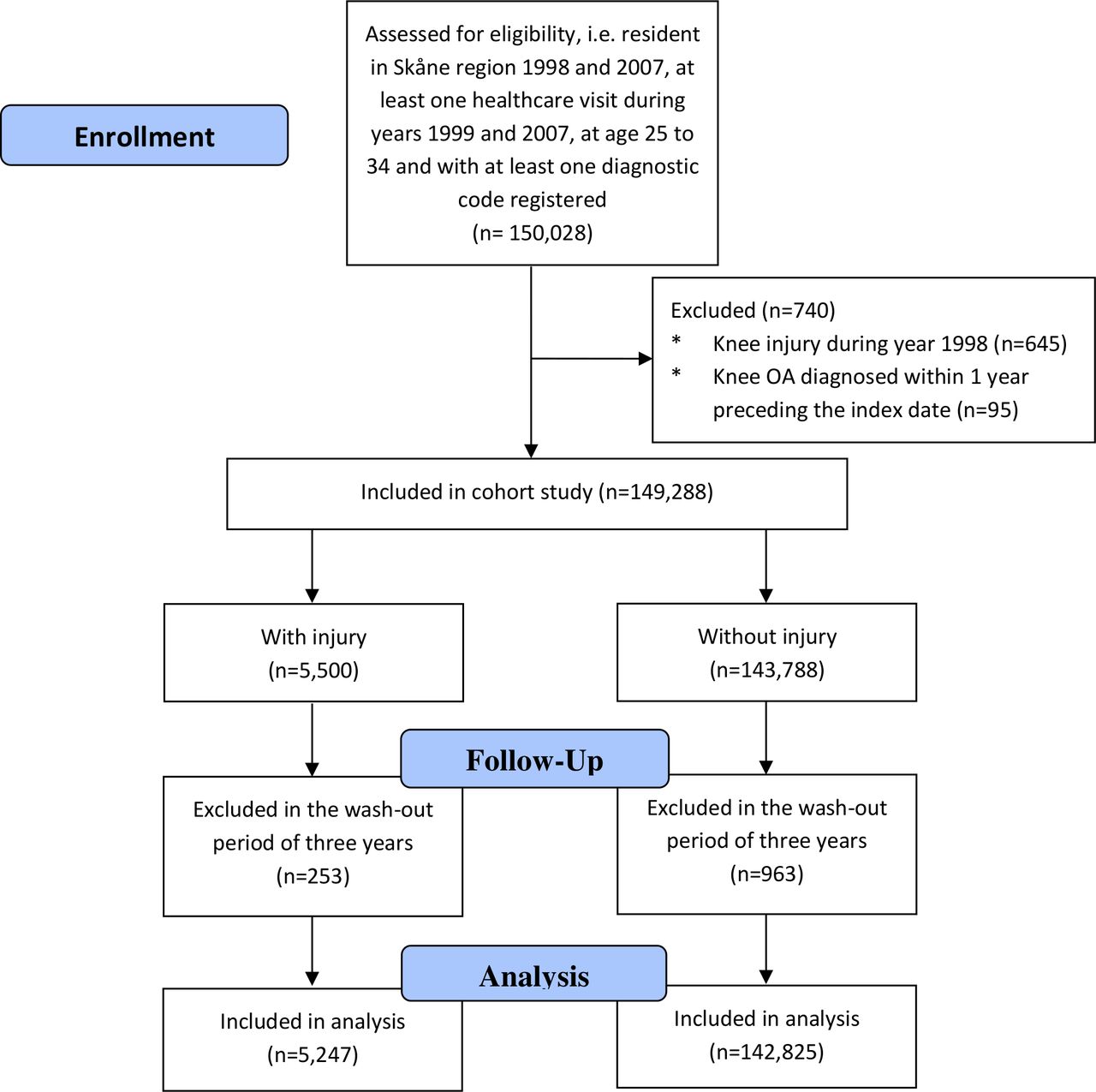
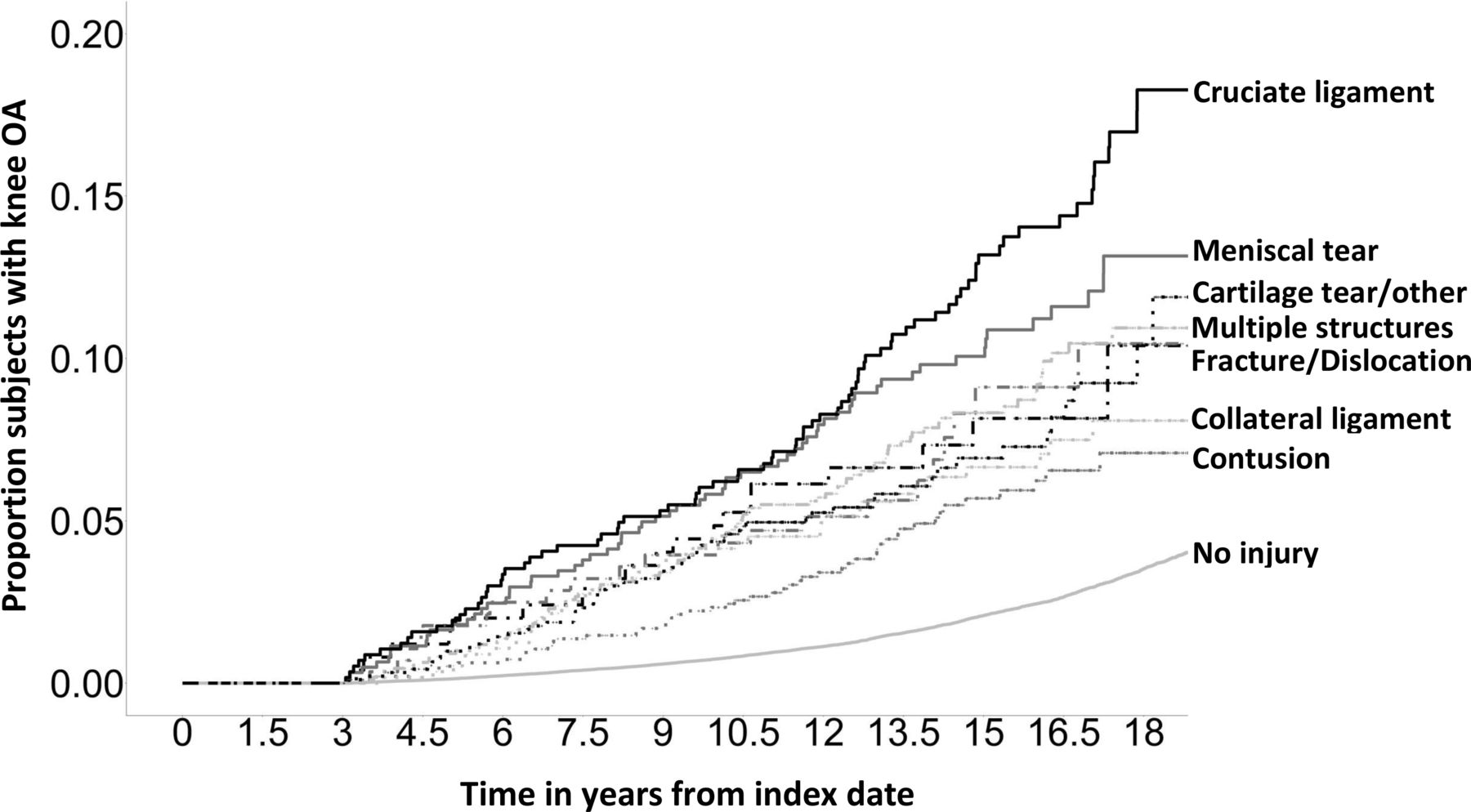
We identified 5247 persons (mean (SD) age 29.4 (2.9) years, 67% men) with a diagnosis of knee injury and 142 825 persons (mean (SD) age 30.2 (3.0) years, 45% men) without a diagnosed knee injury between 1998 and 2007 (table 1, figure 1). In addition to the higher proportion of men, those with a knee injury had lower educational attainment (27% vs 44% with higher education). The most common injuries were injuries to multiple structures of the knee (21%), contusion (18%) and other/cartilage tear (17%, online supplementary appendix, figure 3). The observed median follow-up time was 14.5 years in injured (IQR=12.1–16.9) and 13.9 years in uninjured persons (IQR=11.7–16.8). The rate of censoring before the end of follow-up was 5.67%, of which 0.85% was due to death and 4.82% was due to moving. After 19 years of follow-up, 422 (11.3%) of the persons with a knee injury were diagnosed with knee OA vs 2854 (4.0%) of the uninjured (online supplementary appendix, table 2). The proportion of subjects that developed knee OA differed between specific injuries (figure 2).
Baseline characteristics

Flow diagram of study inclusion and follow-up. OA, osteoarthritis.

{kind=link}
{kind=link}
Cumulative incidence of knee OA between injured and uninjured subjects over time (up to 19 years of follow-up). OA, osteoarthritis.
Association between knee injury and knee OA
The adjusted HR of knee OA after knee injury as compared with uninjured reference subjects was 5.7 (95% CI 5.0 to 6.6) up to 11 years of follow-up and 3.4 (95%CI 2.9 to 4.0) after 11 years of follow-up (table 2). The corresponding adjusted RD up to 19 years of follow-up was 8.1% (95% CI 6.7% to 9.4%). Among persons that developed knee OA up to 19 years of follow-up, the mean restricted time free of knee OA was 8 months shorter among those with injury compared with those without (95% CI −7 to −9 months).
Interval-specific HRs and RDs for injured versus uninjured persons on the risk for knee OA
Interaction with sex and age
The adjusted HR for men was 5.3 (95% CI 4.5 to 6.3) and for women 6.5 (95% CI 5.1 to 8.1) up to 11 years of follow-up. These results were similar after 11 years of follow-up (table 2). For up to 11 years of follow-up, persons younger than 30 years of age had an increased risk of developing knee OA with a HR of 7.6 (95%CI 6.2 to 9.3) compared with persons older than 30 years of age with a HR of 4.7 (95%CI 3.9 to 5.7, table 2), reflecting the lower baseline risk in the younger persons. The corresponding RDs up to 19 years of follow-up were similar in the subgroups, 8.6% (95% CI 6.9% to 10.4%) in the younger age group and 8.0% (95% CI 5.9% to 10.1%) in the older.
Risk of knee OA after specific knee injuries
Compared with uninjured persons, the risk of knee OA increased after a cruciate ligament injury, a meniscal tear and a fracture of the upper end of tibia/patella, with an adjusted HR of 8.2 (95% CI 5.9 to 11.4), 7.6 (95% CI 5.5 to 10.5) and 7.0 (95% CI 4.2 to 11.7) up to 11 years of follow-up, respectively (table 3). The difference in disease-free time from index date to OA between injured persons and those without injury was −16 months (95% CI −17 to −14 months) for cruciate ligament injury, −12 months (95% CI −13 to −10 months) for meniscal tear and −8 months (−10 to −6 months) for fracture. Importantly, all other injury types were also associated with increased risk of future diagnosis of knee OA, with RDs between 3.8% and 8.0% (table 3).
HRs and RDs for specific knee injuries versus uninjured persons and time to knee OA
Sensitivity analyses for cruciate ligament and meniscal injury
In the sensitivity analysis, using 90 days of follow-up to better ascertain the injury exposure information, we found a similarly increased risk for cruciate ligament injuries (RD of 15.0% with 95% CI of 10.5%–19.5%) and meniscal tears (RD of 8.4% with 95% CI of 4.9%–11.8%), as compared with our primary estimate (initial injury diagnoses only). Combined cruciate ligament injuries and meniscal tears yielded the RD of 19.4% (95% CI 10.6% to 28.2%, table 4).
Sensitivity analyses of cruciate ligament and meniscal tears 90 days after the primary diagnosis versus uninjured persons
Discussion
To the best of our knowledge, our study is the first that used a cohort from the general population of young adults to estimate the risk of a wide variety of knee injuries on the development of clinically-evident knee OA. We found that, on average, knee injury was associated with a sixfold increased risk of knee OA. All injury types had an increased risk for knee OA, with cruciate ligament injury, meniscal tear and fracture of the tibia plateau/patella associated with the highest OA risks. Interestingly, the time from index date to OA diagnosis was only 8 months shorter for injured compared with uninjured persons who developed OA at an early age.
Explanation of findings
Knee injury is considered a well-established risk factor for knee OA. However, the evidence comes primarily from case-control studies of prevalent cases of OA in middle/old aged persons.2 6 If more is known about a person’s risk profile, future risk of OA following joint injury could be better determined.15 Our estimate of a sixfold higher OA hazard for persons with knee injury is similar to those obtained from previous smaller studies on young persons.16 17
Additionally, our results indicate that young men and women have a similar risk of developing clinically important knee OA after a knee injury. This is in contrast to a systematic review and meta-analysis where subgroup analysis revealed a higher risk of developing knee OA after knee injury among men although based on very wide CIs.6
Although the hazard for OA was higher for those younger than 30 years vs those older (HR of 7.6 vs 4.7, respectively), the RD was found to be similar (8.6% vs 8.0%). This is expected, as the baseline risk of OA increases with age.2 Also, in our results, the relative differences decrease over time while the absolute difference increases, as the incidence of OA increases with increasing age.
We also shed new light on the OA risk associated with different types of knee injuries in these young persons. For injuries of the cruciate ligament and meniscal tears, we found an increased risk for OA (RD of 19.6% and 10.5%, respectively) compared with the average risk including all types of injuries (RD of 8.1%) corroborating prior findings.1 Radiographical OA signs may appear within a couple of years of ACL injury, and the absolute risk of such radiographical signs increases over time.18 The future risk of such radiographic signs of OA appears greatest in those who have had an ACL injury with concomitant meniscal tear.19 Indeed, a recent systematic review, including prospective as well as retrospective studies, concluded that the odds of future knee OA were lowest for isolated ACL injuries, and similar for meniscal injuries and combined ACL and meniscal injuries.20 In our study, we did not have specific information about joint damage concomitant with a cruciate ligament injury or meniscal tear. However, including relevant diagnostic codes to explore the risk of combined cruciate ligament and meniscal tears, the risk for OA increased slightly compared with ‘isolated’ injuries to one of these structures. We believe there is a substantial degree of underreporting of coexistent injuries as diagnostic codes compared with for example, gold-standard MR examination, and thus the injuries that we now consider isolated must be interpreted with caution.21
Next to cruciate ligament injuries and meniscal tears, we also found that fracture of the tibia plateau/patella was associated with higher risk of knee OA compared with the average risk. In a previous study that retrospectively analysed patients after a tibia plateau fracture, 12.8% had symptomatic knee OA within 10 years after injury for which treatment was warranted.22 This estimate is comparable with the absolute cumulative incidence in our cohort of ~10%; however, our estimate was found after twice the length of follow-up. Literature on this topic is still sparse, and future research should gain more knowledge on OA risk for this specific injury type.
Interestingly, the difference in disease-free time between injured and uninjured persons who developed OA at an early age was small. This is in contrast with our expectations that persons with a knee injury would develop OA faster than persons without injury. We believe that there are two plausible explanations for this. First, the young individuals who develop knee OA without injury probably have other strong susceptibility or risk factors for knee OA, for example, genetic contribution or obesity.23 24 Therefore, it seems that the mechanism/process to develop knee OA is ‘initiated’ through injury, but the process itself is not necessarily faster compared with other risk factors in young individuals. Another explanation could be the relatively short follow-up time, with a median age of 44 years at end of follow-up. Over time, we might have been able to capture more persons who would have developed knee OA, for example, due to genetics or environmental risk factors, but without knee injury. Then, the uninjured persons, who develop OA, would probably on average experience a longer time to develop knee OA compared with the injured persons.
Limitations
There are several important limitations that we would like to point out. BMI is a strong risk factor for knee OA.25 It is potentially also associated with the risk of joint injury, even if such association remains somewhat unclear.26 Unfortunately, we had no information on BMI from the Skåne Healthcare Register. As a surrogate, we adjusted for diagnosis of diabetes (type I or II), obesity and hypertension. However, these diagnoses are not an optimal proxy for obesity and also likely highly underreported in the register. This might have introduced residual confounding, as controlling for the surrogates of BMI is less effective than controlling for exact BMI.27 A second limitation is that we were not able to assess the effect of time-varying confounders like BMI, because they were only measured once.28 Neither could we evaluate potential mediating effects of these factors.
Another limitation is that our risk estimates for knee OA after injury could be overestimated due to surveillance bias.27 If a person presents with knee pain and has a prior record of knee injury, it may be more likely that this person receives additional diagnostics, (eg, imaging of the joint) and a diagnosis of OA compared with uninjured persons. To minimise this potential bias, we excluded outcome events from the first 3 years of follow-up time. This decision was based on the assumption that it is biologically less likely to develop OA during the first 3 years from the index visit. Additionally, to evaluate whether the 3 years was the optimal time to exclude, we modelled the hazard over follow-up time to confirm that it stabilised after 3 years.13
A fourth limitation to mention is the possibility of a misclassification of exposure due to patients who were classified as uninjured but did have an injury prior to inclusion (before 1998). However, due to the low incidence of knee injury, they could only constitute a minor percentage of all reference subjects and are unlikely to have affected the rates of OA incidence in this group.
Another limitation to acknowledge is that persons below the age of 25 years were not included although the incidence of knee injuries is high in this age group. One reason was that many persons at this age group relocate outside of the region and thus they may have less optimal coverage of their healthcare visits in this regional healthcare register. We also expected a relatively low proportion of doctor-diagnosed OA within the follow-up period in this young age category. The choice of age groups for subgroup analysis (eg, 30 years) was not decided a priori but based on the median age in our data.
Last, a certain misclassification of the exposure is likely, for example, individuals with pre-existing knee pain which was aggravated by twisting the knee while, for example, getting out of the car. These patients might have been given an injury code, when it was OA with an a priori ‘negligible’ injury. However, as our cohort was young and as we excluded those with an OA diagnosis within 3 years from index date, only a negligible fraction could have pre-existing OA.
There are several strengths about this study, including a large, population-based sample size with low risk of selection bias and with prospectively registered healthcare data. Further, we provide absolute risk estimates (RDs) for easier clinical interpretation. Last, the impact on knee OA is specified per injury type.
Conclusion
In summary, we found that the risk of clinically diagnosed knee OA at a young age was increased about sixfold after knee injury compared with no injury in the general population. Cruciate ligament injuries, meniscal tears and intra-articular fractures were associated with the highest risk. We also conclude that the time to OA development was only 7–9 months shorter in knee-injured individuals as compared with other individuals who developed OA at young age.
Summary box
What is already known?
Knee injury at a young age is an important risk factor for the development of knee osteoarthritis (OA), but the majority of studies investigating this association only include middle-aged and older populations.
What are the new findings?
Our study is the first that used a cohort from the general population of young adults and found that knee OA at a young age was increased about six times after knee injury compared with no injury.
Of all injury types, cruciate ligament injuries, meniscal tears and intra-articular fractures yielded the highest estimates of increased risk.
The difference in disease-free time between injured and uninjured persons who developed OA at an early age was only 7–9 months, suggesting that persons who develop OA at young age without previous injury have other strong risk factors.
References
Footnotes
Contributors BS takes responsibility for the integrity of the data and the accuracy of the data analysis. BS performed statistical analyses and drafted the manuscript. AT, KM, RF, GP, DY and ME contributed with acquisition of data, conceptual design and analysis and interpretation of data. BS, AT, KM, RF, GP, DY and ME contributed in drafting the article or critically revising it for important intellectual content. All authors gave final approval for the version to be submitted.
Funding This study was funded by the Swedish Research Council, the Greta and Johan Kock Foundation, the Swedish Rheumatism Association, the Österlund Foundation, Governmental Funding of Clinical Research within the National Health Service (ALF).
Disclaimer The funding sources had no influence on the design or conduct of the study, the collection, management, analysis or interpretation of the data, the preparation, review or approval of the manuscript or the decision to submit the manuscript for publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from Lund University ethics committee with ID number DNR 2011/432.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.