Article Text

Abstract
Objectives Clinicians who use the biopsychosocial approach to manage musculoskeletal pain disorders aim to understand how patients make sense of their symptoms. Treatment includes targeting the negative beliefs and coping responses that can lead to progressive pain and disability. We aimed to explore how people seeking care for persistent hip pain and disability make sense of their symptoms.
Methods Cross-sectional qualitative study. People were eligible if they were aged ≥18 years, were consulting an orthopaedic surgeon for persistent hip pain and offered a non-surgical intervention. Data were collected through interviews that explored patients’ beliefs about the identity (diagnosis), causes, consequences, timeline and controllability of their symptoms, their strategies to cope with pain and their experiences in seeking healthcare. Transcribed interview data were analysed thematically using a framework approach.
Results Sixteen people (median age=51, range=33–73 years; median duration hip pain=3 years, range=3 months–20 years) participated. Most participants (10/16) believed their pain was caused by an exercise-related injury. Because of the results of imaging and interactions with healthcare professionals, all participants believed they had damaged hip structures. All described ineffective strategies to manage their pain and multiple failed treatments. For many (7/16), a lack of control over symptoms threatened their physical and mental health.
Conclusions The way participants with persistent hip pain and disability made sense of their symptoms contributed to them avoiding physical activity, and it impaired their sleep, emotional well-being and physical health.
- qualitative
- hip
Statistics from Altmetric.com
Introduction
One in five people aged over 60 years1 and one in four women aged over 50 years2 experience pain and tenderness in the greater trochanter, groin or gluteal region. Hip pain is associated with physical and functional impairments, disturbed sleep and psychological distress3–5 and may result from several conditions in the hip region.
Common diagnoses in patients who present with ‘hip pain’ include trochanteric bursitis, gluteal tendinopathy, femoroacetabular impingement syndrome, acetabular labral tears and osteoarthritis, some of which are often coexisting.6 These conditions are also present among the non-symptomatic population,7 and the correlation between radiographic findings and hip pain and disability is weak.8 Cognitive factors including beliefs about musculoskeletal pain strongly influence pain-related distress and the behavioural responses that drive persistent pain and disability.5 9 10
The Common Sense Model11 states that people who experience musculoskeletal pain draw on a set of beliefs to make sense of their symptoms and decide what to do about them. This set of beliefs, composed of beliefs about the identity, causes, consequences, controllability of the symptom and how long it will last, are informed by previous personal experiences, observing others and incorporating external sources of information such as that from healthcare professionals (HCPs) and the media. Studies in low back pain (LBP)12 and osteoarthritis in multiple joints13 have shown that the way people make sense of their pain is associated with disability up to 6 years later. Among patients awaiting joint replacement surgery, a negative set of beliefs (eg, lower control over symptoms) is associated with reduced functional capacity postsurgery,14 while a positive set of beliefs (eg, lifestyle less impacted by the illness) is associated with better functional outcomes.15
Identifying and addressing negative beliefs in people who present for the treatment of persistent musculoskeletal pain should be a key objective of the clinical encounter,16 17 but little is known about what people with hip pain believe about their condition. The limited research investigating cognitive factors in hip pain has been based on self-report questionnaires.4 5 8 We have previously explored how people with LBP and knee pain make sense of their pain through qualitative interviews based on the Common Sense Model.18 Adopting a similar approach, the aim of this study is to explore how people seeking care for persistent hip pain make sense of their hip symptoms.
Patients and methods
Design
This qualitative interview study was the baseline phase of a prospective case series for hip pain management.
Recruitment
Between October 2016 and June 2017, two orthopaedic surgeons from a private clinic in Perth, Western Australia, identified candidates who met the eligibility criteria (see box 1). Both surgeons receive a high volume of referrals for hip surgery consultations.
Eligibility criteria
Inclusion criteria:
Aged 18 years and over.
Experienced hip pain in the groin, lateral hip or gluteal region.
Were candidates for surgery but had agreed to participate in a physiotherapy-directed cognitive functional intervention.21
Exclusion criteria:
Previous major ipsilateral hip surgery (ie, total hip arthroplasty and/or osteotomy).
Evidence of severe ipsilateral hip osteoarthritis involving non-congruent articular surfaces.
Women who were pregnant or seeking to become pregnant during the study period.
Individuals who were physically or mentally compromised (ie, currently being treated for a psychiatric disorder, senile dementia, Alzheimer’s disease, presence of alcohol or substance abuse), rendering them unwilling or unable to comply with scheduled evaluations and/or rehabilitation.
Comorbidities causing severe mobility impairment (eg, limb amputation, multiple sclerosis, muscular dystrophy, Parkinson’s disease, morbidly obese, hemiplegic and lower limb fracture).
All eligible candidates were invited to participate in the prospective case series. Of the 28 people referred, 11 declined or were unable to be contacted. One further individual was excluded from analysis due to being pregnant. Sixteen people were enrolled in the case series. This paper reports findings from the baseline interview, which all 16 participants took part in 1 week prior to commencing the intervention (see figure 1).
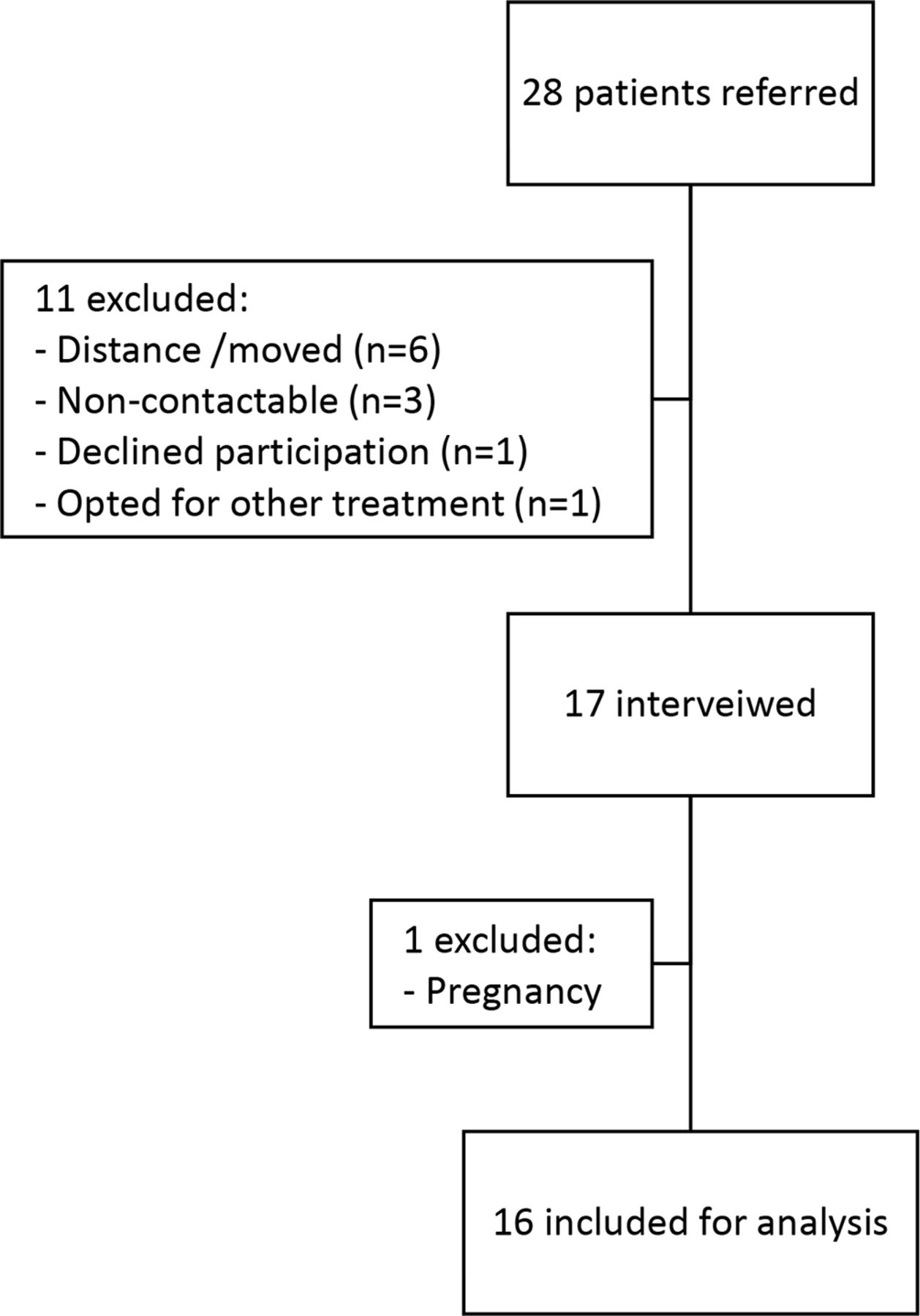
Participant recruitment.
Data collection
Participants completed an online questionnaire in the week prior to their interview. Demographic data composed of age, sex and work status. Clinical characteristics included the duration of pain, impact of hip disease (assessed using the International Hip Outcome Tool 1219—see online supplementary box 1), the risk of persistency and disability (assessed using the Örebro Musculoskeletal Pain Questionnaire Short Form20—see online supplementary box 2). Where available, reports from diagnostic imaging procedures participants had undergone in the last 3 years were reviewed and summarised by the research team.
Supplemental material
Individual interviews were conducted in a consultation room of the participating clinic (n=15) or over the phone (n=1). Interviews were scheduled before participants began a physiotherapy-directed cognitive functional intervention.21 Interviews were conducted by a female academic physiotherapist experienced in qualitative interviewing (BIRdO), who was not previously known to the participants or involved in their treatment. Informed by our previous studies in people with LBP and knee pain, the interview schedule was structured on the Common Sense Model.11
To explore how people made sense of their symptoms, the interviewer asked participants to explain any diagnostic labels they had been given for their symptoms and what these labels meant to them (Identity beliefs). We asked them what they thought the cause(s) of their symptoms were (cause beliefs), what consequences they perceived the symptoms had (consequence beliefs) and how long they expected the symptoms to last (timeline beliefs). We also asked them how much control they believed they had over the symptom, the actions they took to address their symptoms, how effective they perceived these actions to be and what they believed it would take to get control over their symptoms (control beliefs). Interviews lasted on average 60 min, were audio recorded and transcribed prior to analysis.
Analysis
Transcripts were uploaded into NVivo 10 (QSR International, Melbourne, Australia) to facilitate analysis. Data analysis involved a framework approach.22 For each transcript, two authors (SB and BIRdO) classified interview responses into a priori categories (see ‘Category’ column table 2). Data classified under each category were then analysed using inductive coding methods; that is, codes were identified from the raw data rather than defined a priori. For example, under the a priori category ‘Cause’, the codes: ‘ageing processes’ and ‘weakness’ were identified in the raw data. The two authors then independently performed inductive coding on four transcripts to develop an index of codes. One author (SB) then applied the index to all transcripts. The refined index appears in table 1 in the ‘codes’ column. Interview extracts were charted onto a matrix template with categories and codes as row headings, and participant identifiers as column headings. Reoccurring codes within and among codes were identified and emerging interpretations were discussed and challenged among the researchers in this study with different professional backgrounds: clinical physiotherapists (AJS, PPBO, SH and SB), orthopaedic surgeons (DF and RK) and physiotherapists with expertise in qualitative designs (BIRdO and SB).
Demographic characteristics, International Hip Outcome Tool 12 (iHOT-12) scores, Örebro scores and diagnostic imaging report
Results
Participants were each given a pseudonym, and their demographic and clinical characteristics are presented in table 1. Their median (range) age was 51 years (33–73 years) and the median (range) duration of hip pain was 3 years (3 months–20 years). The median (range) iHOT-12 score was 33 (11–57), suggesting that for most participants, the impact of pain was equal or greater than that reported among people undergoing hip arthroplasty.23 The median Örebro Musculoskeletal Pain Questionnaire Short Form score was 57, with 12 individuals scoring above the cut-off (>50) for high risk of future disability.20 Eleven participants provided diagnostic imaging reports (eg, MR images). The most common findings on diagnostic imaging were labral tears, chondral damage and gluteal tendinopathies and tears (see table 1.)
Participants reported they had engaged in the health system and had consulted with multiple HCPs including general practitioners, orthopaedic surgeons, radiologists, physiotherapists, exercise physiologists, chiropractors, nurses, natural medicine and regenerative medicine consultants. The outcome of the analytic process is presented in table 2. Four key themes were identified: (1) ‘Lay’ versus ‘informed’ perceptions of cause; (2) ‘Fissures and tears’: the use of the diagnostic jargon; (3) ‘Fixing damage’ and ‘controlling symptoms’; and (4) Exercise, sleep and the threat to mental health. Each theme is described below, with supporting quotes presented in table 3. Themes are further illustrated within the Common Sense Model11 in figure 2.
Outcome of analytic process
Supporting quotes

{kind=link}
{kind=link}
Making sense of hip pain within the Common Sense Model.
‘Lay’ versus ‘informed’ perceptions of cause
A range of perceived causes were reported. Common to the narratives of eight participants was a history of high intensity physical activity, either in their younger years (Q1) or leading up to onset of hip pain. Ten participants believed their hip pain was caused by excessive exercising or altered movements (Q2). Another eight participants believed their hip pain may have been attributed to their previous history of persistent LBP (Q3). The experiences of younger participants could be differentiated from older participants who perceived that hip pain was a normal part of ageing (Q4). Often multiple causal attributions could be identified in participants’ narratives. For example, one participant attributed her hip pain to lifting young children; muscle loss following cancer treatment; and a leg length discrepancy ‘diagnosed’ by a chiropractor (Q5) (table 3, quotes 1–9).
All participants had widely sought care for their hip pain from various HCPs. Participants appeared to differentiate between what they thought was the cause of their pain (‘lay’ perceptions) and what HCPs had told them was the cause of their pain (‘informed’ perceptions). Sometimes ‘lay’ and ‘informed’ perceptions of cause conflicted (Q6). ‘Lay’ perceptions of cause were favoured over ‘informed’ perceptions of cause when they made more sense in the timeline of pain (Q7) or when informed causal attributions provided little hope of ‘fixing’ the problem. This was particularly the case for three women who reported their HCP telling them that tendons can ‘spontaneously’ break down in women over 50 years (Q8). Conversely for some, ‘informed’ perceptions of cause were favoured over ‘lay’ perceptions when they provided more hope of getting control over pain. This was illustrated by one participant who had thought that her hip was caused by the sexual abuse she had suffered in the past until an HCP suggested that it was caused by a previous back injury (Q9).
‘Fissures and tears’: the use of the diagnostic jargon
All participants had undergone multiple diagnostic imaging, usually a radiograph, CT scan and MRI. When describing the imaging findings, the participants used precise diagnostic medical terms. They used anatomical terms such as ‘acetabulum’, ‘gluteal muscles’ and ‘labrum’. They used terms such as ‘fissuring’ and ‘tearing’ to describe how the tissue in their hip structures were ‘damaged’ (Q10). Many participants perceived that the imaging findings could explain the symptoms they were experiencing. For example, one participant described how she had always felt like something was catching in hip, and the torn labrum seen on the MR images provided her with a way to make sense of this symptom (Q11). While some participants were reassured to receive a diagnosis that could explain their symptoms, others found it frightening to receive imaging reports detailing so many things wrong with their hip (Q12). Only a couple of participants believed that the imaging findings did not satisfactorily explain their symptoms and felt that they needed more invasive investigation (Q13) (see table 3, quotes 10–13).
Fixing damage and controlling symptoms
Participants differentiated between strategies to ‘fix the damage’ and ‘control the symptoms’ (Q14). Most were optimistic that their ‘damaged’ hip structures could be ‘fixed’, and despite almost all having done physiotherapy directed exercises in the past, most believed they would benefit from further ‘strengthening’ their hip and core muscles. In particular, participants who perceived their hip to be ‘unstable’ believed strengthening exercises were the key to fixing their problem (Q15). Four participants suggested that stem cell technology had the potential to regenerate their damaged tissue and resolve their condition; two had already undergone stem cell injections. One participant was optimistic that the recent stem cell injection would ‘knit’ the labral tear together (Q8), while another described feeling disappointed when the second plasma injection did not provide him with the pain relief he experienced with the first (Q16). Five participants believed that a future hip replacement was inevitable because there was nothing else that they could do to address the underlying structural abnormality (Q17) or because they felt they had exhausted all non-surgical treatment options (Q18) (see table 3, quotes 14–24).
Older participants felt that they needed to accept that they were not as young as they used to be (Q19). Most participants controlled their symptoms through avoiding the activities and movements that they believed would aggravate their symptoms (Q20). When avoidance was not possible, they described attempts to modify their behaviour during these activities and movements (Q21). Two participants had gone to extreme lengths, learning alternative therapies such as self-administered needling in order to control their symptoms (Q22). Almost all participants had undergone cortisone injections, but these had failed to provide sustained relief (Q23). The repeat experience of failed treatments took a psychological toll on the participants, with many describing feelings of distress associated with ‘not knowing what else to do’ to get control over their symptoms (Q24).
Exercise, sleep and the threat to mental health
For many participants, exercise had played a central role in their lives and was seen as fundamental to their psychological well-being. Seven described how their inability to exercise threatened their mental health (Q25). The perceived consequences of being unable to exercise included irritability and frustration as well as worry about one’s general health. One participant who had survived cancer described her fear that the cancer could return if she did not maintain a high level of exercise (Q26). Three participants were particularly concerned that their inability to exercise would exacerbate their underlying mood disorders (Q27). Eight participants experienced pain at night that awoke them from sleep. A lack of sleep impaired emotional well-being by sparking a cascade of consequences including inability to concentrate and participate in paid work and disrupted relationships (Q28) (see table 3, quotes 25–28).
Discussion
This qualitative study explored how patients seeking care for persistent hip pain made sense of their symptoms.
Making sense of persistent hip pain through a biomedical lens
All participants made sense of their pain through a biomedical lens. They believed that hip pain and disability were due to ‘damaged’ hip structures, ‘degeneration’, ‘fissures’, ‘tears’, ‘detachment’ and/or ‘arthritis’. Participants reported that these beliefs derived from a combination of diagnostic imaging reports and information provided by HCPs.
Some participants believed their ‘damaged’ hip structures were caused by physical activity, loading and/or an injury; many reported being told by HCPs that their ‘damage’ had been caused by ‘faulty biomechanics’ and ageing. These findings are similar to reports among people with knee osteoarthritis18 24 and LBP.25–27 The belief that structural pathology based on radiological imaging is an accurate measure of a person’s pain experience is common at a societal level and among HCPs.28 29 This is despite evidence that levels of pain and disability do not correlate closely with radiographic findings in people with hip pain,8 that ‘pathology’ is prevalent in asymptomatic populations30 and that informing patients of imaging findings can lead to poorer health outcomes.31
This biomedical lens appeared to influence the participants’ coping responses. The participants attempted to limit further damage and control their pain through activity avoidance and movement modification, such as avoiding squatting movements, adopting an antalgic gait or using upper limb strength to push themselves up from a sitting position or lift themselves out of a car. Activity avoidance and modification due to fear of doing more damage has also been reported among people with persistent LBP (eg, avoiding ‘bending’ their back or pacing activities) and knee osteoarthritis (eg, avoiding/pacing activities or choosing activities believed to cause less damage, such as cycling).18 24 32 Research has demonstrated a relationship between negative pain beliefs, greater functional disability and motor control impairments in people with LBP33 and knee arthritis,34 35 further highlighting the interplay between cognitive factors and coping responses to pain.
Although some participants in this study believed they could ‘fix’ or ‘control’ the ‘damage’ to their hips through strengthening exercises, stem cell treatment and steroid injections, previous attempts to do so had failed to provide long-term benefit. These ‘failed treatments’ reinforced the belief among some participants that the damage to their hip structures was irreversible and that a hip replacement was inevitable. The belief that a joint replacement is the only definitive ‘cure’ for painful joints is common among older people with lower limb osteoarthritis and HCPs and may underlie low referral rates and low adherence to effective non-surgical management options.36–38 The repeated experience of ‘failed’ treatments has been suggested to play a role in symptom incoherence (an inability to make sense of pain) and the development of pain-related fear in people with musculoskeletal pain.33
Peoples’ experiences of persistent hip pain were described through a biopsychosocial lens
The biomedical lens through which the participants in this study made sense of their pain contrasts with the biopsychosocial lens through which they experienced pain. The participants in this study perceived that disrupted sleep and an inability to engage in physical activity threatened their physical and mental well-being by increasing emotional distress, frustration and compromising their ability to cope. The bidirectional relationship between depression, sleep and persistent musculoskeletal pain is well documented.39 40 Furthermore, the interaction of disrupted sleep, depression and reduced activity contributes to vicious cycle of pain, distress and disability.4 40 By illustrating the role of biopsychosocial factors influencing a person’s hip pain and disability, these findings strengthen calls to action to change the prevailing biomedical paradigm and reduce reliance on imaging as a sole explanation of a person’s pain experience.21 36 41
Clinical implications
To facilitate this change in paradigm, the use of the CLEAR principle when reporting on imaging has been advocated: (1) consistent language: the use of minimally threatening language so as not to create fear; (2) epidemiological information using age-matched findings for asymptomatic populations; and (3) assessment of relevance: explaining that imaging findings must be considered with clinical features.42 In addition, recent guidelines recommend the screening and assessment of biopsychosocial factors including pain beliefs and concerns, fear, depression, social context, sleep, obesity as well as physical activity levels and strength in people with musculoskeletal pain.36 43 Where persistent musculoskeletal pain presents with health comorbidities such as obesity, sleep and/or mental health disorders, multidisciplinary care is recommended.21 36 However, all patients presenting with musculoskeletal pain can benefit from education regarding the multidimensional complexity of musculoskeletal pain. Highlighting the important role that modifiable risk factors such as beliefs, physical activity, sleep and weight management play in their pain disorder provides opportunities for self-management.44 Recent research supports the long-term benefits of interventions that target these factors in people with hip and knee pain.45–47 Table 4 provides examples of alternative health messages that aim to facilitate positive health behaviours.
Suggested alternative health messages when communicating with people with persistent hip pain
Design considerations
We authors are interested in cognitive behavioural interventions for musculoskeletal pain. We selected the Common Sense Model11 as a validated framework to explore how people make sense of their musculoskeletal symptoms. As is inherent to qualitative research, our lens (world view) necessarily influenced the design and conduct of this study. Thus, alternative interpretations to those presented in this paper are possible. By declaring our lens, providing the interview schedule, code book and supporting quotes, we have attempted to leave an ‘audit trail’ that makes our assumptions and interpretations explicit.
While this study comprised a small convenience sample, we employed qualitative techniques to exhaust new concepts such as concurrent data collection and data analysis to enable us to explore and challenge emerging concepts in subsequent interviews. The patterns we identified among the 16 participants were sufficient to answer our research question. We acknowledge that the insights gained from this small convenience sample are of limited generalisability. To assist readers make judgements about the transferability of these findings to their own clinical settings,48 we have provided a rich description of the demographic and clinical characteristics of this sample. Prior to enrolling in the study, the participants had all sought an opinion from an orthopaedic surgeon in a private practice setting and had agreed to participate in a physiotherapy-directed cognitive functional intervention. We did not collect demographic data on the 11 people who were referred to the intervention but declined to participate.
Did health literacy influence our study results? People who seek care from doctors in private orthopaedic practice in Australia have higher health literacy than those seeking care from the public system.49 Whether higher health literacy influenced the beliefs of the participants in this study is uncertain. There is some evidence that people with higher health literacy hold more positive beliefs about musculoskeletal pain.50 However, there is evidence that negative beliefs about musculoskeletal pain are, in part, iatrogenic and can arise from conflicting advice from HCPs.27 33 Given that people with higher health literacy find it easier to seek care,51 it may be that this sample (which had widely sought care) held more negative beliefs than the wider population. While we emphasise that similar biomedical beliefs have been documented in other musculoskeletal pain populations in different healthcare settings,18 24 52 future research involving larger, more generalisable samples is needed to understand how widespread the beliefs described among this sample are.53
Conclusion
Participants in this study seeking care for persistent hip pain reported negative beliefs relating to ‘damaged’ hip structures, which appeared to lead them to coping responses such as activity avoidance and movement modification. Participants reported subsequent psychological distress, disrupted sleep and reduced physical activity, threatening their physical and mental well-being. Targeting pain beliefs and coping strategies may provide opportunities for more effective self-management of persistent hip pain.
What are the findings?
Interactions with healthcare professionals can lead to people with persistent hip pain developing ‘hip damage’ beliefs.
Discussions of imaging findings may contribute to people developing ‘hip damage’ beliefs.
Negative beliefs can lead to ineffective coping strategies such as avoiding physical activity. This in turn impairs physical well-being and mental health in people with persistent hip pain.
How might it impact on clinical practice in the future?
Healthcare professionals influence health beliefs and coping responses of people with persistent hip pain. Our findings highlight that clinicians need to be taught that their choice of words—communication content—influences patient outcomes. Future research should address the question—‘What is the ideal message for patients with hip pain?’.
Supplemental material
Acknowledgments
The authors acknowledge all participants of the study, as well as staff members from The Joint Studio and Body Logic Physiotherapy for facilitating data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @BeatrizIRdeOli1
Presented at This study was presented at the World Confederation for Physical Therapy Congress 2019.
Contributors BIRdO, SB, AJS and PPBO designed the study and were involved in drafting and reviewing of the manuscript. PPBO, SH, DF and RK facilitated participant recruitment. BIRdO, SB and AJS analysed and interpreted the data. All authors provided critical revision of the manuscript. All authors take responsibility for the integrity and accuracy of the data in this study. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PPBO is a Director of Body Logic Physiotherapy but at no time received any funds from the research.
Patient consent for publication Not required.
Ethics approval This study was approved by the Hollywood Private Hospital Research Ethics Committee (HPHREC - HPH441) and the Curtin University Human Research Ethics Committee (HR56/2016).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Data are in the form of digital voice recordings of interviews, which were also transcribed verbatim into Word files. These data are stored in a password-protected research drive only accessible to the researchers of this study. Voice recordings contain identifiable data and will not be made available on request to maintain participant anonymity. Transcriptions with deidentified participant data may be made available on reasonable request.