Article Text

Abstract
Background This study examines sickle cell trait (SCT) as a cause of sudden death in National Collegiate Athletic Association (NCAA) athletes and explores the cost-effectiveness of different screening models.
Methods The authors reviewed the cause of all cases of sudden death in NCAA student-athletes from January 2004 through December 2008. The authors also explored the cost-effectiveness of screening for this condition in selected populations assuming that identifying athletes with SCT would prevent death.
Results There were 273 deaths and a total of 1 969 663 athlete-participant-years. Five (2%) deaths were associated with SCT. In football athletes, there were 72 (26%) deaths. Of these, 52 (72%) were due to trauma unrelated to sports activity and 20 (28%) were due to medical causes; nine deaths were cardiac (45%), five were associated with SCT (25%). Thirteen of the 20 deaths due to medical causes occurred during exertion; cardiac (6, 46%) SCT associated (5, 39%), and heat stroke unrelated to SCT (2, 15%). All deaths associated with SCT occurred in black Division I football athletes. The risk of exertional death in Division I football players with SCT was 1:827 which was 37 times higher than in athletes without SCT. The cost per case identified varied widely depending on the population screened and the price of the screening test.
Conclusions Exertional death in athletes with SCT occurs at a higher rate than previously appreciated. More research is needed to (1) understand the pathophysiology of death in SCT-positive athletes and (2) determine whether screening high-risk populations reduces mortality.
Statistics from Altmetric.com
Introduction
Sickle cell trait (SCT) has received significant attention as a cause of death in American football athletes. It has been cited in the medical literature as a leading cause of death in military basic training and civilian organised sport,1,–,4 and the lay press has characterised death in football athletes with SCT as nearly epidemic. SCT is common, with 1 in 14 (7%) of blacks having SCT and up to 1 in 625 Caucasians carrying the gene.5 However, while SCT is common in the general population, the RR of exertional death related to SCT is unknown.
Normal haemoglobin (Hgb) is composed of two α and two β chains. Hgb S results from the substitution of a valine for glutamic acid at the sixth amino acid of the β globin chain. Hgb S produces a haemoglobin tetramer that is poorly soluble when deoxygenated which can cause the red blood cell to form a sickle shape. Sickle cell disease occurs when an individual is homozygous for Hgb S. Vaso-occlusion and haemolysis leading to sickle cell crisis are the hallmark of sickle cell disease which is generally incompatible with strenuous exercise. SCT occurs when an individual has one normal Hgb gene and one for Hgb S and is usually considered benign. Although there is an increased incidence of exertional death in those with SCT, the underlying pathophysiological mechanism is unclear.
An association of SCT with sudden death was first reported in 1970 when it was noted that a disproportionate number of deaths in military recruits training at moderate altitude were positive for SCT.6 Kark expanded on these findings reporting that the risk of sudden death in black recruits with SCT was 28 times those without SCT in a review of medical records and autopsy data.7 Other studies in military basic training have confirmed an association of sudden death with SCT.8 9 Concern of a similar association in athletes developed after the 1973 death of a college football player and was first addressed by an National Collegiate Athletic Association (NCAA) guideline in 1975. Despite NCAA guidelines, there have continued to be intermittent deaths related to SCT in the NCAA. There is no published literature quantifying the risk of death in NCAA athletes with SCT; however, in 2010 legislation was enacted requiring all Division I schools to screen athletes or have them sign a waiver declining the screen, if the athletes' SCT status was not already known from neonatal birth screening. This study examines SCT associated sudden death in NCAA athletes and explores the cost-effectiveness of different screening models.
Methods
All cases of sudden death in NCAA student-athletes from January 2004 through December 2008 were examined for cause of death using a previously defined database of death in athletes.10 The database was developed using two different data sources:1 the NCAA Resolutions list and2 from the Parent Heart Watch (PHW) database. The NCAA Resolutions list is compiled annually in honorarium of NCAA student-athletes who have died of any cause and is voluntary. PHW is a not-for-profit group dedicated to the prevention and awareness of sudden cardiac arrest (SCA) in young people. They keep an ongoing database of sudden death and SCA in young people created from weekly internet searches. The PHW Database was reviewed, and deaths in NCAA athletes were identified and cross-referenced with the NCAA Resolutions list, which was then combined into a single database.
Missing information regarding cause of death was acquired through internet searches and media reports, reports in the NCAA News as well as emails and telephone calls to sports information directors, head athletic trainers, athletic directors and coroners. When possible, the student-athlete's parents or guardians were interviewed. The study was approved by the University of Washington Division of Human Subjects.
Demographic data in NCAA athletes were obtained from the NCAA Sport Sponsorship and Participation Rates Report11 and the NCAA Student Ethnicity Report.12 The gender and ethnic information is provided by institutions to the NCAA annually, and these reports are compiled periodically by the NCAA Department of Research. The number of athletes participating overall and in football in each division was recorded. The numbers of black athletes and non-black athletes were also noted, and the numbers of those with SCT were estimated as being 7% of black athletes and 0.16% of non-black athletes (the vast majority of who were Caucasian) according to prevalence rates reported by the Centers for Disease Control (CDC).5 Death in NCAA athletes was noted and death in football athletes was examined with particular attention to death in athletes with SCT.
The cost-effectiveness of screening athletes for SCT was explored to estimate the cost per life-year gained of different screening models assuming that identification of an athlete with SCT would prevent their death. The cost of screening tests used to identify SCT varies according to the type of test as well as regional variations in cost. Three test costs were examined:1 $5,2 $30 and3 $150. The ‘simple $5 screening test’ was initially identified by the NCAA as a viable test method. Beginning in October 2011, the NCAA has contracted with a laboratory to provide screening haemoglobin solubility tests to member institutions for about $10 and haemoglobin electrophoresis for ∼$30. Haemoglobin electrophoresis can cost up to $150 at some institutions. Cost-effectiveness was calculated assuming an initial start-up year when all athletes were screened. Screening in subsequent years occurred only for incoming athletes and was calculated assuming no start-up year. For simplicity, it was assumed that testing for SCT was 100% sensitive and specific and that identification of an athlete with SCT would prevent their death representing a best-case scenario. It was also assumed that prevention of death in a college-aged athlete would afford an additional 50-year life expectancy (approximating the average life expectancy). A cost per life year saved less than $50 000 was considered cost-effective.
Results
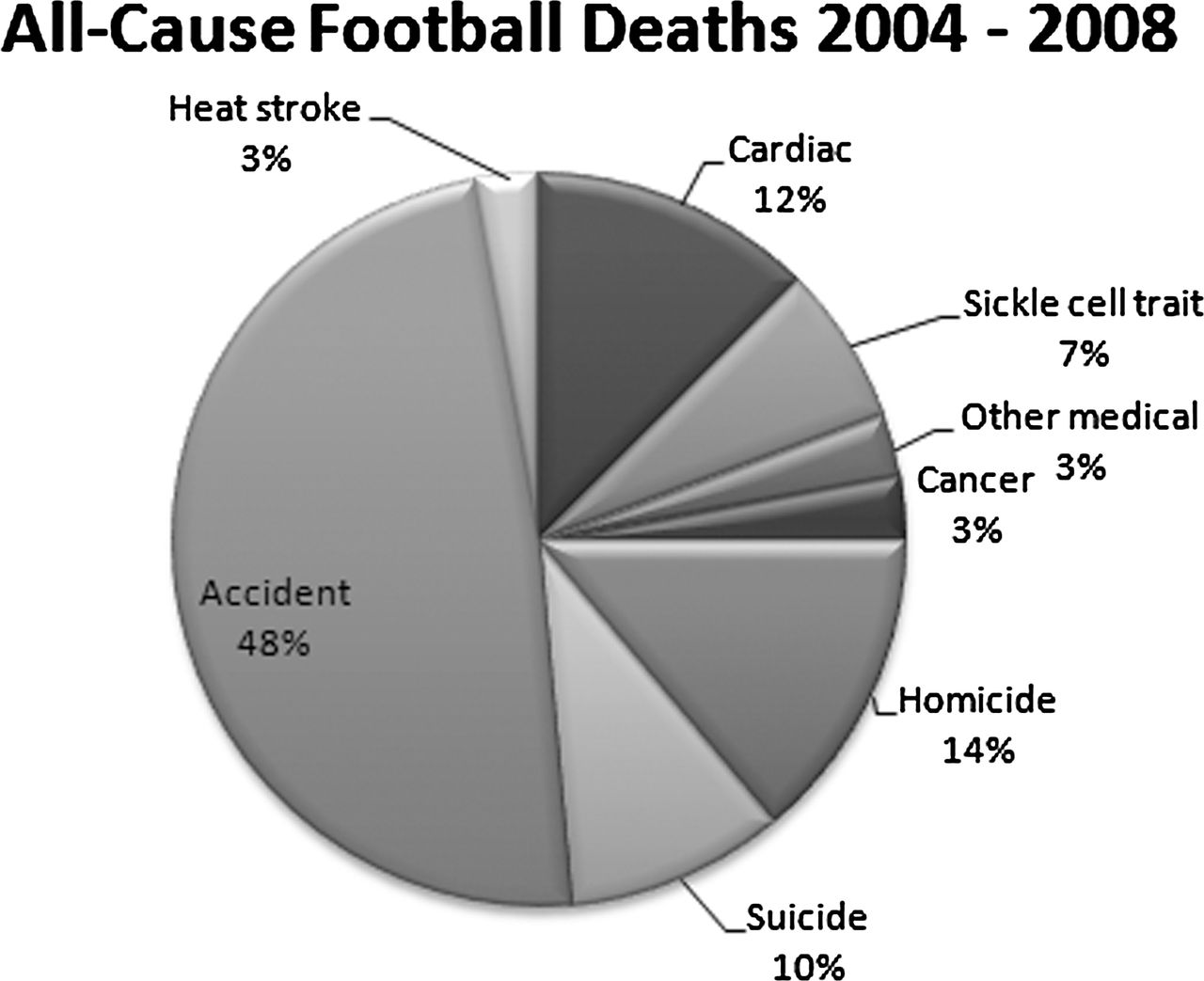
During the 5-year period from 2004 to 2008, there were 273 deaths and a total of 1 969 663 athlete-participant-years. Five (2%) of all deaths occurred in athletes with SCT(figure 1). Football represented 72 (26%) of all student-athlete deaths. Of these, 52 (72%) were due to trauma unrelated to sports activity and 20 (28%) were due to medical causes (figure 2). The leading medical cause of death in football athletes was cardiac (9, 45%), followed by death associated with SCT (5, 25%), heat stroke unrelated to SCT (2, 10%), cancer (2, 10%), diabetes (1, 5%) and sepsis (1, 5%). No deaths were related to head trauma or concussion. No deaths occurred during competition.

All-cause NCAA deaths 2004–2008.

All-cause football deaths 2004–2008.
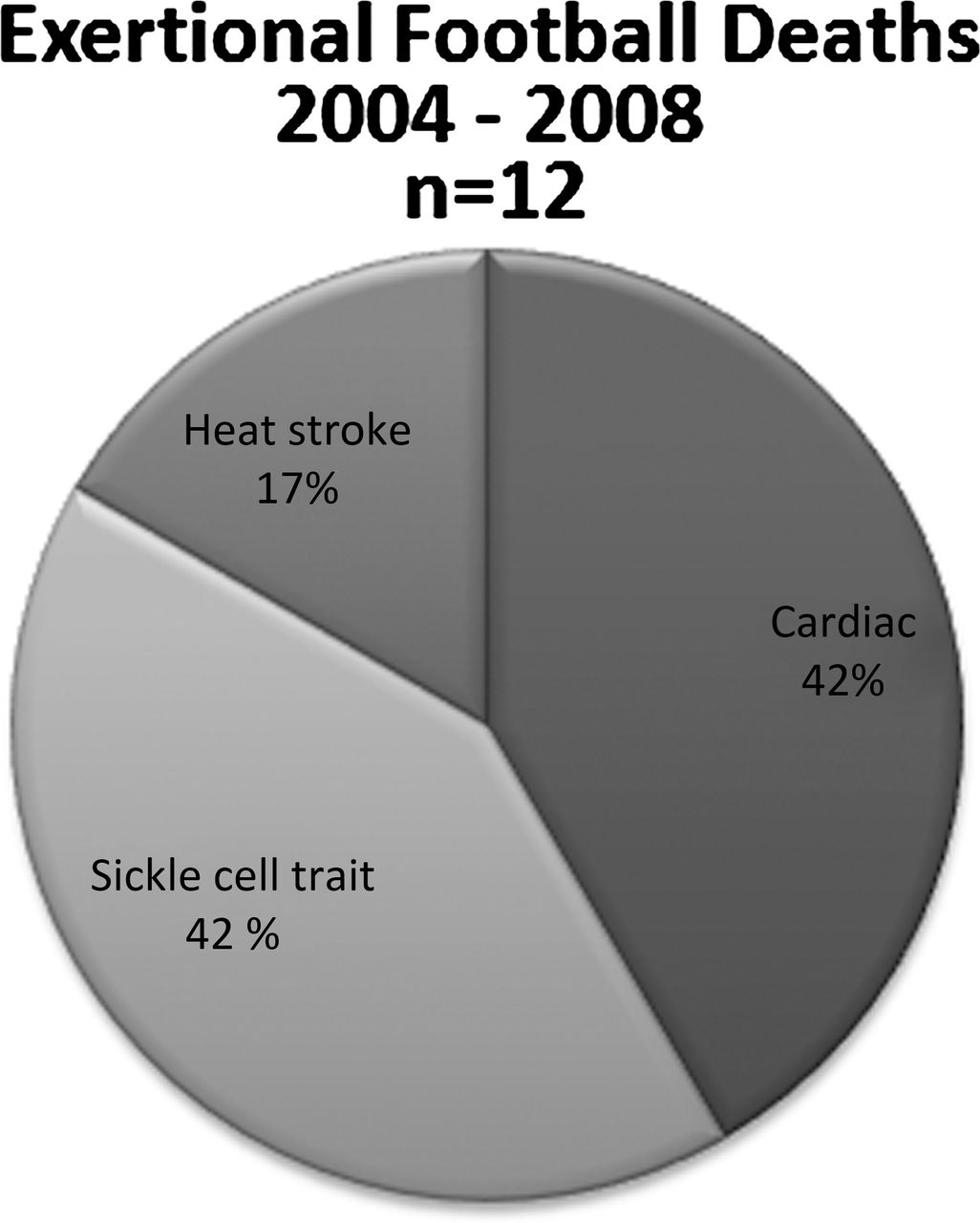
Deaths which occurred with exertion were analysed. These included deaths due to cardiac causes, heat illness and deaths associated with SCT. In football players, there were 12 exertional deaths. Of the exertional deaths, five were related to cardiac causes (42%), five were in athletes with SCT (42%) and two were from heat stroke in athletes without SCT (15%) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Exertional deaths 2004–2008; n=12.
All deaths in athletes with SCT occurred in black Division I football athletes during practice or conditioning. Thus, the risk of death associated with SCT in non-football athletes or non-black athletes in this cohort was zero. For those identified with SCT, the risk was quite high. Overall, the risk of exertional death associated with SCT was 1:4706 for all athletes (all sports, all divisions, all ethnicities) and 1:4171 for black athletes (all sports, all divisions). For Division I football players (all ethnicities) with SCT the risk of death was 1:827, and in black Division I football athletes with SCT the risk was 1:805 (table 1).
Exertional death rates with and without sickle cell trait
The RR of exertional death in athletes with SCT (all divisions, all sports) was 15 times higher than exertional death in athletes without SCT. In Division I football athletes (all ethnicities) with SCT, the risk of exertional death was 37 times greater than exertional death in those without SCT, and in black Division I football players with SCT the risk of exertional death was 22 times greater than exertional death in black players without SCT (table 1). The overall risk of exertional death from any cause was 5.2 times higher in black athletes with or without SCT compared with that in non-black athletes.
Cost-effectiveness of screening was dependent on the population screened, the price of the screening test and the assumption that identification of athletes with SCT prevents death. Four subgroups were examined;1 black football athletes (all divisions),2 football athletes (all ethnicities, all divisions),3 black athletes (all sports, all divisions) and4 all athletes (all ethnicities, all sports and all divisions). The cost estimate included a first year of screening all athletes at an institution followed by only screening incoming athletes over the 5 year study. The total cost of the programme ranged from $202 900 (black football athletes) to $119 539 920 (all athletes). The cost to prevent one death over 5 years ranged from $40 580 (black football athletes) to $23 907 984 (all athletes). The cost per life-year saved ranged from $812 to $478 160 (table 2). Screening only incoming athletes was cost-effective in all groups if a $30 test was used costing $2435 per year life saved (black football athletes) to $47 816 (all athletes) (table 3).
Cost-effectiveness analysis of sickle cell screening for 2004 to 2008 (including first year start-up cost)
Cost-effectiveness analysis sickle cell screening for 2004 to 2008 (no start-up costs with $30 test)
Discussion
SCT is associated with exertional death in NCAA football players with a rate of 1:827 in Division I football athletes. The death rate is 37 times higher in football athletes with SCT than those without. Death in other athletes with SCT or those undergoing strenuous physical exertion has been reported although in this cohort no other sports were represented.1 3 4 8 9 13,–,15 The National Center for Catastrophic Sport Injury Research has documented 12 deaths association with SCT, seven of which occurred between 2000 and 2008. Other experts have cited up to 19 deaths associated with SCT in NCAA athletes since 1973 (Eichner, personal communication). All but 2 of these 19 deaths have been in Division I football players. There has been one NCAA male basketball athlete playing pick-up basketball and one male track athlete who have reportedly died from exertional collapse in athletes with SCT.
Although there is an association between exertional death and SCT, the pathophysiology of death is unknown. It has been proposed that a combination of high-intensity exercise, dehydration and thermal strain may induce sufficient hyperthermia, hyperosmolality, acidosis and red cell dehydration to lead to significant erythrocyte sickling, inflammation and microvascular occlusion causing exertional collapse in some exercisers with SCT.2 15,–,18 Blood viscosity and adhesion properties are also altered in athletes with SCT.19,–,26 The proposed mechanism of death is arrhythmia caused by hyperkalaemia from muscle necrosis and altered ion channel permeability.1 2 16 18 However, others argue that this is unlikely citing the contrast between the proposed pathophysiology and the known problems seen in people with sickle cell disease who experience sickling episodes with splenic, pulmonary and bony infarcts. Environmental factors such as exercise intensity, altitude, hydration status and concurrent illness likely play a role in the development of exertional death in SCT. There may also be other genetic co-factors which make some athletes with SCT more likely to be affected than others.18
Strategies to prevent death in those with SCT seem warranted. Restriction from play is not recommended, but instead screening and targeted interventions are needed in those with SCT.27 28 Determining the SCT status of athletes can be accomplished by reviewing previous medical history or repeat testing. All newborns are screened at birth for sickle cell disease where early interventions in those homozygous for Hgb S have shown to positively impact health. While SCT status is also identified, this information may not be communicated and is often not recalled by the athlete or their parents. If SCT status is not known, testing can be accomplished by several methods. A haemoglobin solubility test is recommended by the NCAA at a minimum. In this test, a reagent is added to blood. Hgb S is insoluble compared with other haemoglobins and the blood will appear cloudy instead of clear. This test does not distinguish between sickle cell disease, SCT and other haemoglobin variants and false positives and false negatives occur. A positive test should be followed up with additional testing to confirm and further define any abnormalities. The NCAA has contracted with a national laboratory to provide this testing to NCAA institutions for less than $10.
Haemoglobin electrophoresis is a more accurate method to determine haemoglobin type. With electrophoresis, the haemoglobin migrates through a gel at different rates when an electrical charge is applied. Hgb electrophoresis can differentiate between different Hgb subtypes and is considered the most accurate method for identification of haemoglobinopathies. Isoelectric focusing has also been used to identify those with SCT. This test is similar to electrophoresis except the blood is run through a gel with a pH gradient. Electrophoresis and isoelectric focusing are considerably more expensive and more time-consuming to perform than Hgb solubility testing. Many institutions do not have the capacity to quickly perform multiple tests which can be problematic if athletic participation is restricted until SCT status is known.
From a public health perspective, screening should only be performed if there is an effective intervention. It is unclear if recommended interventions in athletes with SCT are effective. Recommended interventions include screening to identify athletes followed by education, targeted modifications of training and conditioning, an acclimatisation schedule, cessation of activity with any symptoms, and allowing SCT athletes to set their own pace. Athletes must also emphasise hydration, controlling asthma, oxygen availability at altitude and restricting workouts if he/she is ill.27 However, deaths do occur in athletes despite knowledge of sickle cell status. During the cohort studied, the status of one athlete with SCT who died (20%) was known. In the last decade, there have been 10 exertional deaths in NCAA football players with SCT. The SCT status was known in three athletes (30%) based on publicly available records.
The armed services have different approaches to prevention of exertional death related to SCT. The United States Navy, Marine Corps and Air Force all screen recruits for SCT. The Army does not screen for SCT status; however, in 1982 in response to the increased number of basic training deaths in SCT recruits, the US Army implemented strict hydration policies including direct observation of recruit drinking and measurement of wet bulb globe temperature with modification of training if a certain threshold was reached. During the 10 years of the study period (1982 to 1991), there were no deaths related to SCT in the intervention group (2.3 million recruits) compared with an unchanged rate of deaths in non-participating centres (1.2 million recruits).29 The conclusion of this study was that exertional heat illness is the predominant factor causing exercise-related deaths associated with SCT. It has also been demonstrated that exertional sickling can be prevented with adequate hydration.17 30 Recruit deaths in the Army have increased since the initial intervention prompting the military to re-examine its policies.
Conclusions
SCT is associated with an increased risk of death in NCAA football athletes. While the most common medical cause of death in football athletes is sudden cardiac death, most athletes dying during exertion in football are positive for SCT. NCAA football players identified with SCT have an exceedingly high-risk of exertional death (1:827) that is 37 times higher than those without SCT. Screening for SCT status or signing a waiver is required of NCAA Division I athletes although the value of SCT athlete identification and targeted training modifications to reduce mortality has not been proven. If identification of athletes with SCT is effective in preventing mortality, then screening high-risk groups would be cost-effective.
Additional research is needed to understand the value of screening for SCT in NCAA athletes. Given all deaths in athletes with SCT in this cohort occurred in black Division I football athletes during practice or conditioning, it seems medically and ethically prudent to screen the highest risk group of athletes – at least black Division I football players, with consideration in all black athletes and/or all football players – and target educational interventions for the player, coaches and medical staff. The value of screening in other populations, for instance high school or recreational athletes, is unknown. Strict attention to heat and hydration has been demonstrated to prevent death in US military recruits and should be heavily emphasised in football practice and conditioning. Universal attention to adequate hydration, heat mitigation practices and not continuing to push a struggling athlete should be adopted in all sports.
What this study adds
▶ This study is the first study to examine the incidence of death associated with sickle cell trait (SCT) in college athletes.
▶ Sudden cardiac death is the leading cause of death in National Collegiate Athletic Association football athletes but SCT is an important and potentially preventable cause of death associated with exertion.
▶ The incidence of exertional death in athletes with SCT is 1:827.
▶ It is unknown whether screening prevents death associated with SCT.
References
Footnotes
-
Competing interests None.
-
Ethics approval Human Subjects Division at the University of Washington.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement De-identified data may be available. Requests should be made to the corresponding author.