Article Text

Statistics from Altmetric.com
Superstitions and rituals are commonplace in sports and range from simple activities such as each player touching a special inanimate object before entering the field of play to more extreme behaviours such as not washing a uniform or wearing the same underwear during a winning streak. These practices are relatively harmless and may reduce precompetition anxiety, but a concerning ritual that has recently developed in sports is the prophylactic use of non-steroidal anti-inflammatory drugs (NSAIDs).
Athletes misuse NSAIDs
Athletes have relatively unrestricted access to NSAIDs, as they are readily available over-the-counter preparations and not considered as performance-enhancing drugs by the World Anti-Doping Agency.1 It has been known for some years that athletes are frequent users of NSAIDS,2 with approximately a quarter of athletes competing at the Sydney 2000 Olympic Games reporting NSAID use in the 3 days before random drug testing.3 Such prevalent NSAID use may reflect the physical rigors of elite athletic endeavours, but more recent data suggest athletes misuse their open access to NSAIDs. Tscholl and colleagues4 recently reported in this journal that 23% of top-level male football players used NSAIDs in two out of three matches during the 2002 and 2006 Fédération Internationale de Football Association World Cup tournaments and that more than 10% of players took NSAIDs before every match. These data suggest that many athletes use NSAIDs prophylactically and presumably for prolonged periods. This hypothesis is supported by the finding that high-school level American football players who take NSAIDs daily do so because of perceived benefits in terms of blocking pain before it occurs.5
Prophylactic use of NSAIDs is not safe
The prolonged prophylactic use of NSAIDs by athletes is a major concern as use of these agents is not without consequence. NSAIDs exert their anti-inflammatory and analgesic effects via inhibition of the cyclooxygenase (COX) isozymes and, in particular, the inhibition of COX-2. The COX isozymes catalyse the rate-limiting step in the formation of prostaglandins from arachidonic acid. By inhibiting COX-2-mediated prostaglandin synthesis immediately before or following injury, NSAIDs can reduce musculoskeletal pain and accelerate return of function.67 However, the prolonged prophylactic use of NSAIDs by athletes is unsafe. In addition to participating in inflammatory processes, prostaglandins synthesised in response to COX activity have important gastrointestinal and cardiovascular functions. As a result, NSAID use is associated with elevated risk of adverse effects within these systems, irrespective of the relative COX isozyme selectively of the agent.8910 As the adverse gastrointestinal and cardiovascular effects associated with NSAIDs become more pronounced with increased duration of use, athletes risk serious side effects by using NSAIDs prophylactically for prolonged periods. This is further compounded in some athletes as approximately 10% of those who use NSAIDs take up to five different compounds concomitantly.3411
Prophylactic use of NSAIDs may negatively impact musculoskeletal pathology
A paradoxical consequence of the prophylactic use of NSAIDs by athletes is that these agents can compromise the musculoskeletal system.12 NSAIDs taken before activity may mask pain and thus cause athletes to inadvertently allow pathology to progress. Even more significantly, NSAIDs’ inhibitory effects on the COX isozymes and prostaglandins may impede the synthesis of the extracellular matrix (ie, collagen) that confers strength to tissue. This has two important ramifications for athletes. First, COX-2 and prostaglandins are important mediators in the responsiveness and subsequent adaptation of connective tissues to mechanical stimuli.1314 Athletes who regularly take NSAIDs before exercise may have reduced tissue adaptation to prevailing loads potentially predisposing them to future injury. Second, prolonged prophylactic use of NSAIDs has the potential to reduce the rate of matrix production and subsequent tissue repair following microscopic or macroscopic injury. This has been shown most convincingly following fracture where prolonged NSAID use delayed healing,15 but NSAIDs also delay healing of acute ligament, muscle and tendon injuries.16171819
Recommendations for NSAID use by athletes
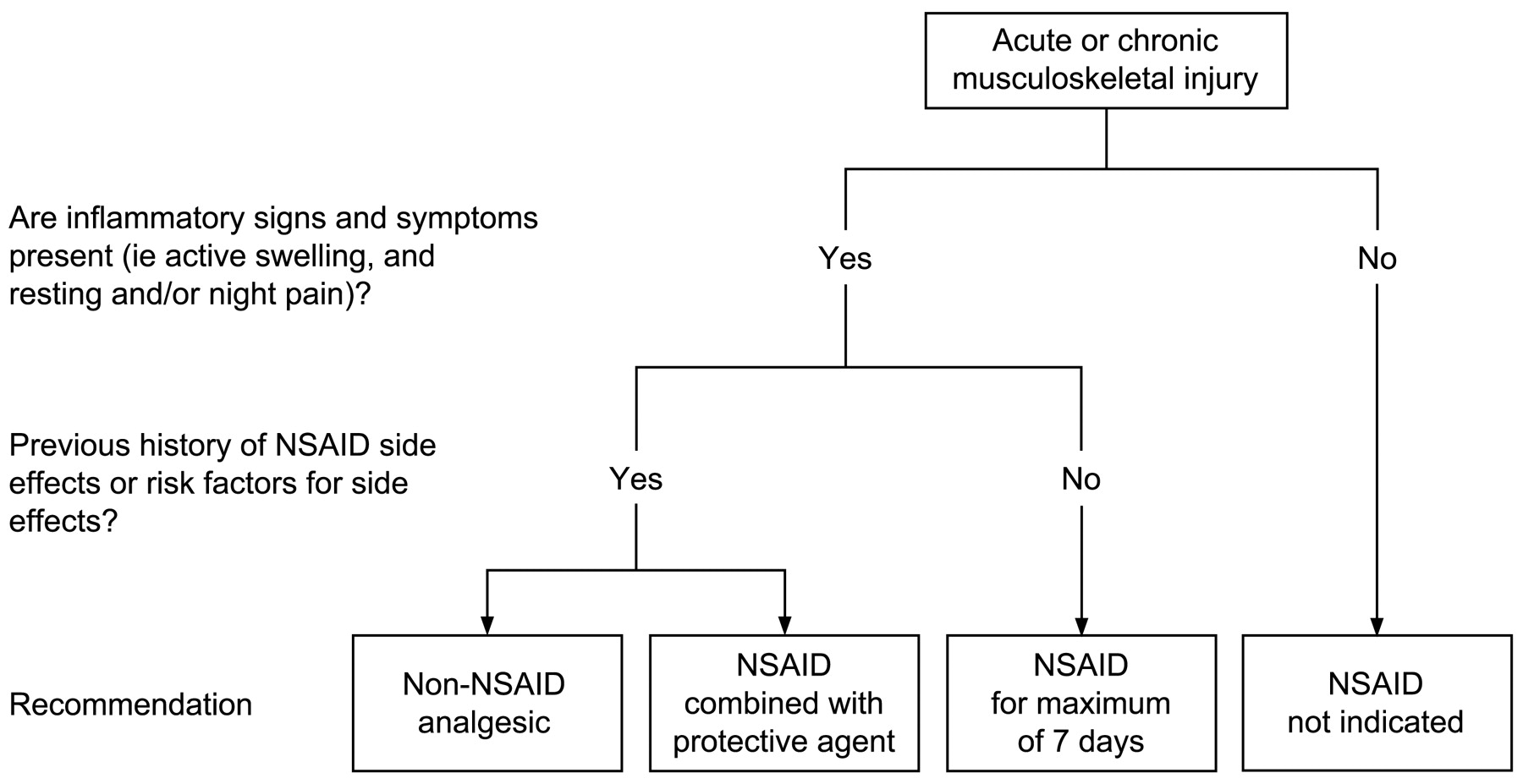
There is no clinical evidence to suggest that regular use of NSAIDs reduces injury risk or improves function in the typical athlete. While “absence of evidence is not evidence of absence”, there is sufficient concern regarding potential side effects of NSAIDs to warrant their judicious use. Athletes require education that NSAIDs are principally indicated as short-term adjuncts for the alleviation of acute pain and inflammation during rehabilitation. This means that NSAIDs should not be used prophylactically (in the absence of injury) and that they do not represent a solo therapy or a substitute to active rehabilitation. Supporting the use of NSAIDs for clinical indications (ie, injuries, rather than prophylactically) is the observation that their negative effect on musculoskeletal tissue adaptation can be diminished if the NSAID is taken after the fact (ie, after exercise) rather than prophylactically.20 If an athlete wants to use an NSAID, he or she should consult a sports medicine professional. If it is decided that NSAID intervention is indeed indicated (fig 1), its use should be restricted to the minimal dose and for the minimal duration—for instance, during the early stage (up to 1 week) following injury when inflammatory signs and symptoms (ie, active swelling and resting and/or night pain) are present. Taken during this stage, NSAIDs reduce pain and promote function following injury6 and there is evidence to suggest that short-term use limits the negative effects of NSAIDs on tissue-level healing.2122 Athletes with a history of side effects or risk factors for side effects with NSAIDs should be provided lower-risk non-NSAID analgesia such as paracetamol, which may be as effective as NSAIDs at treating acute musculoskeletal pain.23 Alternatively, at-risk athletes may be offered the option of taking a concomitant protective agent, such as a proton pump inhibitor for gastroprotection.9 Ultimately, there is no indication or rationale for the current prophylactic use of NSAIDs by athletes, and such ritual use represents misuse of these potentially dangerous agents.
{kind=link}
Decision tree for the prescription of non-steroidal anti-inflammatory drugs (NSAIDs) to athletes with an acute or chronic musculoskeletal injury.
REFERENCES
Footnotes
Competing interests None.