Article Text

Abstract
Background Vitamin D deficiency is common in the general public and athletic populations and may impair skeletal muscle function. We therefore assessed the effects of vitamin D3 supplementation on serum 25[OH]D concentrations and physical performance.
Methods 30 club-level athletes were block randomised (using baseline 25[OH]D concentrations) into one of three groups receiving either a placebo (PLB), 20 000 or 40 000 IU/week oral vitamin D3 for 12 weeks. Serum 25[OH]D and muscle function (1-RM bench press and leg press and vertical jump height) were measured presupplementation, 6 and 12 weeks postsupplementation. Vitamin D deficiency was defined in accordance with the US Institute of Medicine guideline (<50 nmol/l).
Results 57% of the subject population were vitamin D deficient at baseline (mean±SD value 51±24 nmol/l). Following 6 and 12 weeks supplementation with 20 000 IU (79±14 and 85±10 nmol/l, respectively) or 40 000 IU vitamin D3 (98±14 and 91±24 nmol/l, respectively), serum vitamin D concentrations increased in all participants, with every individual achieving concentrations greater than 50 nmol/l. In contrast, vitamin D concentration in the PLB group decreased at 6 and 12 weeks (37±18 and 41±22 nmol/l, respectively). Increasing serum 25[OH]D had no significant effect on any physical performance parameter (p>0.05).
Conclusions Both 20 000 and 40 000 IU vitamin D3 supplementation over a 6-week period elevates serum 25[OH]D concentrations above 50 nmol/l, but neither dose given for 12 weeks improved our chosen measures of physical performance.
- Sports and nutrition
- Supplements
- Nutrition
- Muscle metabolism
Statistics from Altmetric.com
Introduction
There is an increasing body of evidence for a multiplicity of roles for the vitamin D endocrine system throughout the human body.1 Such evidence has developed from an appreciation for the existence of a nuclear receptor (vitamin D receptor—VDR) for the biologically active form of vitamin D (1,25-dihydroxyvitamin D3) and its expression in a large number of tissues.2 The active metabolite is a potent secosteroid hormone that interacts with more than 200 genes via the VDR, giving it a wide range of actions.3 One tissue regulated by vitamin D is skeletal muscle.4 Indeed, in those with a clinical vitamin D deficiency, skeletal muscle myopathy (presenting as a proximal muscle weakness) is often observed.5 ‘Normalisation’ of 25 hydroxyvitamin D (25[OH]D) concentrations in patients with myopathy has been shown to reverse the myopathy.6–8 Histological and electromyographic investigations in vitamin D deficient sample populations have demonstrated muscle fibre atrophy, a reduction in motor unit potentials and muscle weakness.7 ,9 A type II fibre atrophy has also been observed in the non-hemiplegic vastus lateralis muscle of elderly stroke patients, which was corrected with vitamin D supplementation.10
Given the importance of vitamin D in human physiology and disease prevention, an alarming number of populations exhibit low vitamin D concentration,11–15 including athletic populations (table 1). Vitamin D can be obtained from dietary sources, although it is primarily synthesised endogenously from solar ultraviolet B (UVB) radiation.25 Inadequate vitamin D concentrations in developed countries have been attributed to the tendency to live a sun-shy lifestyle26 by living and working indoors for the majority of sunlight hours. In some countries, such as the UK, extreme cloud cover is experienced for many months of the year,27 which reduces the amount of UVB radiation reaching the earth's surface. At northerly lying latitudes (including the UK), the sun is at a more oblique zenith angle, which results in fewer photons striking the earth per area of land,28 resulting in less of a stimulus (ie, UVB radiation) for cutaneous vitamin D synthesis. In contrast, it has been reported that individuals who live and work outdoors in sun-rich environments demonstrate much higher serum concentrations of 25[OH]D with a median concentration of 122 nmol/l reported ((IQR 95–154)29). In athletic populations, it has been reported that vitamin D deficiency is not different between indoor and outdoor athletes,19 which may be related to the use of sunscreen and the type of clothing worn.
25[OH]D concentrations in athletic populations worldwide
Reviewing the data on 25[OH]D concentrations of athletes and the physiological consequences of any deficiency is also complicated by the ongoing debate as to what concentrations of total 25[OH]D constitute vitamin D deficiency, insufficiency, sufficiency and toxicity. Zittermann30 defines ‘optimum’ 25[OH]D concentration as being between 100 and 250 nmol/l, whereas the US Institute of Medicine (IoM) defines inadequate 25[OH]D concentration as being less than 50 nmol/l and suggests that there are potential adverse events associated with levels greater than 125 nmol/l. The Scientific Advisory Committee on Nutrition (SACN) and the Food Standards Agency (FSA) of the UK define deficiency as a 25[OH]D <25 nmol/l, although these policies have been the subject of recent critique.27 It must be stressed that the recommended ‘optimum’ concentrations are defined in relation to adequate bone function/metabolism and there are currently no accepted guidelines to the optimum levels to maximise neuromuscular performance. Interpretation of existing data is also complicated by the variations in biochemical methods used to measure 25[OH]D. In this regard, recent recommendations state that both vitamins D2 and D3 should be assessed using high performance liquid chromatography (HPLC) mass spectrometry (Tandem MS) to allow an accurate assessment of total 25[OH]D concentration.31–34
Despite the equivocal definitions of vitamin D deficiency, it would appear that a large proportion of individuals worldwide are at risk of low 25[OH]D concentrations that may result in subsequent health risks including myopathy. This would suggest a need for correction of poor vitamin D concentration via supplementation, since it is clear that cutaneous synthesis is limited at northerly lying latitudes. Oral supplementation of vitamin D3 has been previously shown to increase serum 25[OH]D in a dose-dependent manner, although these studies have generally been performed using conservative doses of vitamin D aimed at maintaining serum 25[OH]D at 25 nmol/l35 or were performed using non-athletic middle-aged participants.36 To date, the supplementation period and dosage required to increase and maintain serum 25[OH]D concentration>50 nmol/l in athletes are unclear and, moreover, little is known regarding the effect of 25[OH]D concentration on muscle function in athletes. Therefore, the aims of the current study were to (1) investigate two doses of vitamin D supplementation (20 000 vs 40 000 IU/week vs placebo) on serum 25[OH]D concentration in club-level male athletes over 6 and 12 weeks and (2) to assess if there was any effect of changes in serum 25[OH]D on physical performance.
Methods
Participants
After providing written informed consent, 30 club-level athletes (table 2) participated in the study during the months (January to April). All athletes were based in the UK at a latitude of 53°N and were members of various university athletics clubs including football and rugby. Testing took place in the winter months as solar radiation is negligible during October to April at a geographic latitude of ∼53°N.37 All volunteers were non-smokers and free from illness and injury. Any participant taking vitamin D supplements or fish oils, as well as regular sunbed users, was excluded from the study to eliminate potentially confounding variables. All participants were asked to refrain from taking any other supplements for the duration of the study. The study was approved by the Human Ethics Committee of Liverpool John Moores University. Five participants withdrew at 6 weeks due to either phobia of venepuncture (n=1), external injuries (n=2) or an unwillingness to complete the 12-week trial (n=2); therefore, 25 participants completed the study. A power calculation was performed prior to the start of the study using Minitab software (V.15) to allow for any dropouts based on detecting a significant change in serum 25[OH]D in response to the various doses of vitamin D supplementation.38 Pilot work from our laboratories during the winter months suggested that the SD for test–retest serum 25[OH]D concentrations (taken 6 weeks apart) in young athletes is ∼12 nmol/l. To enable the detection of a 25 nmol/l increase between presupplementation and postsupplementation (25 nmol/l was chosen as the concentration change in serum 25[OH]D that would increase the concentration over 75 nmol/l) with 80% power; n=6 participants per group was required, and therefore 10 participants per group were recruited to allow for dropouts.
Subject characteristics at baseline (mean±SD)
Research design
All participants initially completed a test–retest reliability study separated by 7 days on the various performance measures: vertical jump, 20 m sprints, 1-RM bench press (BP) and 1-RM leg press. Resting venous blood samples were then drawn for total 25[OH]D measurement following which participants were allocated to groups via block randomisation based on baseline total 25[OH]D concentration (see table 2). Only participants with baseline total 25[OH]D less than 100 nmol/l were allowed to participate in the supplementation phase. A list of random numbers was generated using an online random number generator by an independent researcher based within the university to randomly allocate participants into their respective groups, and this individual also blinded the supplements and was responsible for unblinding the trial once all data had been analysed. Participants received either 20 000 or 40 000 IU vitamin D3 (cholecalciferol) or a visually identical placebo (PLB) (100 mg maltodextrin) once a week for 12 weeks. Both the vitamin D3 and the PLB were provided by Biotech Pharmacal Inc (Arkansas, USA) and were independently batch tested to ensure that there was no contamination with prohibited substances. Capsules were administered in a double-blind design and provided in identical child-safe containers labelled as either A, B or C. To assess musculoskeletal performance, participants repeated the performance tests listed above prior to supplementation (January), at 6 (mid February) and 12 weeks (end April) and additionally had venous blood samples drawn at these time points for the assessment of total 25[OH]D. As a result of dropouts, final numbers for the 6-week and 12-week tests were n=9, 10 and 6 for the placebo group, the 20 000 IU vitamin D group and the 40 000 IU vitamin D group, respectively. During the testing period, participants continued to perform their own training plans with their various clubs. There was no major change in the level of physical activity during the 12-week study.
Assessment of total 25[OH]D concentration
Resting venous blood samples were taken from each individual and collected in serum separation tubes (Becton Dickinson, Oxford, UK), allowed to clot at room temperature for 1 h and centrifuged at 1000 G for 15 min at 4°C. Serum was removed and stored at −40°C for later assessment of total 25[OH]D. 25[OH]D2 and 25[OH]D3 and deuterated internal standard were extracted from all serum samples, following zinc sulfate protein precipitation, using Isolute C18 solid phase extraction cartridges. Potential interfering compounds were removed by initial elution with 50% methanol, followed by elution of the vitamins using 10% tetrahydrofuran in acetonitrile. Dried extracts were reconstituted prior to injection into a HPLC tandem mass spectrometer in the multiple reaction modes (MRM). The MRM transitions (m/z) used were 413.2>395.3, 401.1>383.3 and 407.5>107.2 for 25[OH]D2, 25[OH]D3 and hexa deuterated [OH]D, respectively. Interassay coefficients of variation for the assays were <10% across a working range of 2.5–625.0 nmol/l for both 25[OH]D3 and 25[OH]D2. Total 25(OH)D is the combination of 25[OH]D2 plus 25[OH]D3. Vitamin D status was classified as defined by the US Institute of Medicine (see table 3).
US Institute of Medicine (2011) vitamin D concentration classification
Performance tests
Performance testing took place on the same day and was performed in the following order: 20 m sprints, vertical jumps followed by maximum strength tests. Prior to performance testing, participants had their height (cm) and weight (kg) measured. Maximum speed was determined by 20 m sprints with a rolling start on an indoor running track and was timed using electronic timing gates (Brower Timing Systems, Wireless Sprint System 2007, Brower, USA). Maximum lower limb power was assessed by vertical jumps using an electronic jump mat (Takei Jump Meter, Jump-MD, Takei, Japan). Hands were placed on the hips to prevent upper limb assistance. In both vertical jumps and sprints, three measurements were taken 1 min apart and an average calculated. Upper and lower body maximum strength was assessed using 1-RM measurements for BP and leg press using an isokinetic dynamometer (Concept 2, Nottingham, UK). Three 1-RMs were completed for each measurement consecutively, and the maximum score was used.
Statistical analysis
Statistical analyses were performed using the Statistical Analysis Package for Social Sciences (SPSS V.15 for Windows, Chicago, Illinois, USA). Statistical difference was set at an α-level of 0.05. For test–retest reliability of the performance variables, data were analysed using paired t tests and the coefficient of variation (CV) was calculated.39 Performance and blood data were analysed using a 3×3 mixed design analysis of variance. When a significant F value was observed, Bonferonni corrected t tests were used to locate the differences between means and statistical difference was set at an α-level of 0.0167.40
Results
Reliability of performance variables
There were no significant differences in any of the performance variables between test and retest (see table 4), with all tests having a CV of less than 5%.
Test–retest reliability for all presupplementation performance tests
Serum total 25[OH]D concentration
There was no significant difference in serum total 25[OH]D concentration (see table 2) between the PLB, 20 000 and 40 000 IU groups at baseline (p=0.966). Although the mean values of all three groups were slightly greater than 50 nmol/l, 17/30 individuals (57%) had concentrations less than 50 nmol/l with 6/30 (20%) being classed as deficient or severely deficient. Of the 30 participants tested, only three (10%) had detectable serum 25[OH]D2 (the mean of which was 11 (±4) nmol/l), and therefore all data are reported as total 25[OH]D as opposed to being split into D2 and D3.
Changes in serum total 25[OH]D can be seen in figure 1. There was a significant change in serum 25[OH]D concentration over the 12-week period in all groups (p<0.0005), although the magnitude and direction of change were significantly different between groups (p<0.0005). Six weeks’ supplementation with 40 000 IU induced greater values than 20 000 IU (p=0.016), although at 12 weeks, there was no significant difference between either of the dosages (p=0.62). In contrast, PLB showed a progressive decline in serum 25[OH]D at 6 (p=0.008) and 12 weeks (p=0.006) compared with presupplementation. There was a negative correlation between baseline serum total 25[OH]D concentrations and the magnitude of the increase in serum total 25[OH]D (figure 2) in both the 20 000 (R2=0.837) and the 40 000 IU/week groups (R2=0.635).
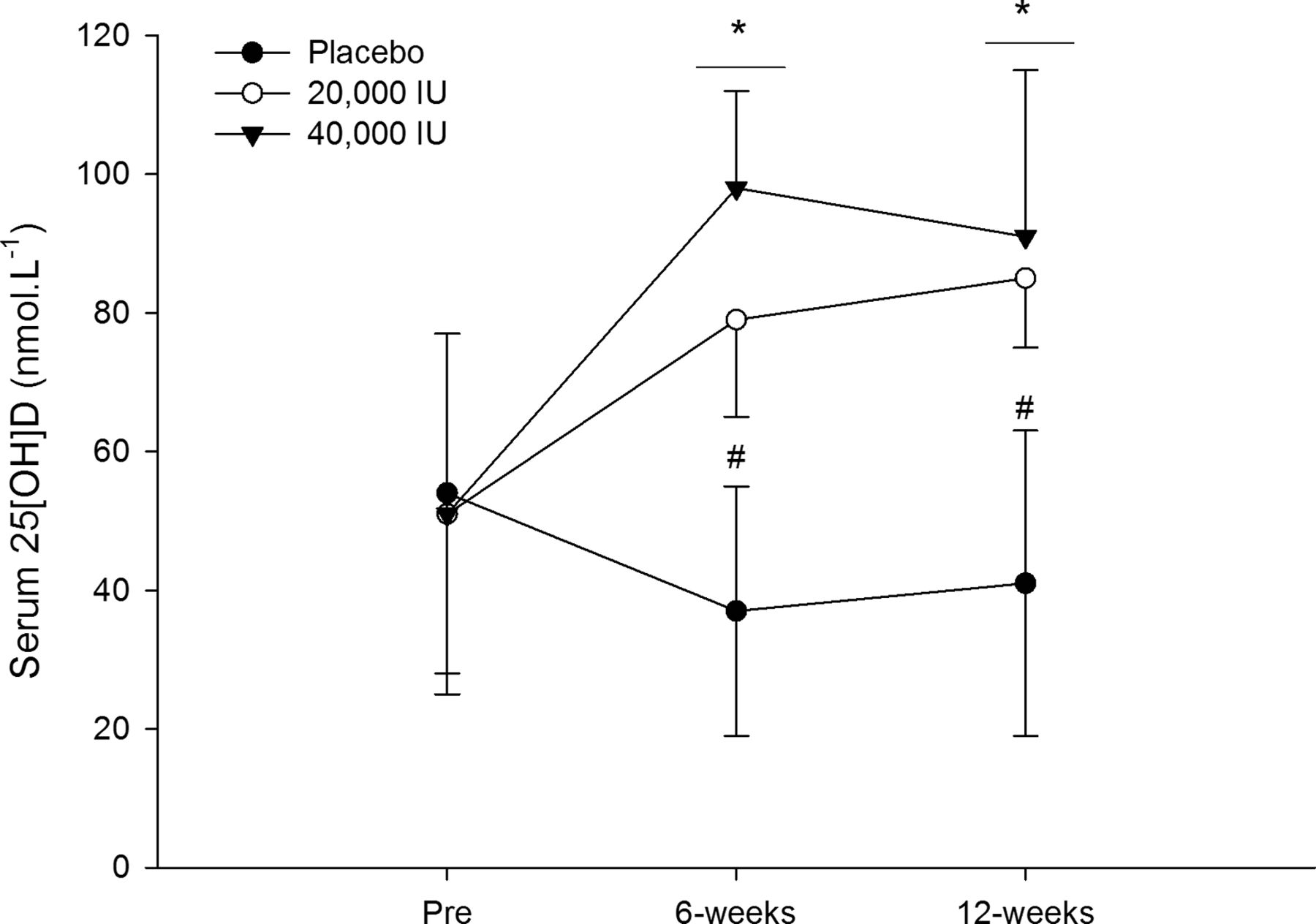
Change in serum total 25[OH]D concentration following supplementation with PLB, 20 000 and 40 000 IU/week of vitamin D3. Line with * indicates significant difference from Pre in all groups at the corresponding time point and # indicates significant difference from the 40 000 IU group (p<0.05).

{kind=link}
{kind=link}
Regression analysis demonstrating the effect of presupplementation serum total 25[OH]D on response to vitamin D3 supplementation at 20 000 (top) and 40 000 (bottom) IU/week.
Performance tests
All data from the performance tests are shown in table 5. There were no significant changes in any of the performance tests over the 12-week period (1-RM-BP, p=0.17; 1-RM leg press, p=0.18; vertical jump, p=0.90 and 20-m sprint, p=0.64).
Performance test data represented as mean (±SD) for PLB, 20 000 and 40 000 IU/week oral vitamin D3 supplementation at baseline, weeks 6 and 12—postsupplementation
Discussion
We were motivated by the rationale that a large proportion of UK based athletes may be vitamin D deficient and that this deficiency could impair athletic performance. In agreement with previous research from our group,24 ,41 we report high levels of vitamin D deficiency (57%), which is likely to be related to a sun-shy lifestyle,26 severe cloud coverage in the UK27 and fewer photons of light striking a given area of the earth during winter months.28 Although the present study has used the US IoM criteria for defining deficiency, there is growing concern that these guidelines could be classed as outdated and conservative.42 ,43 If 25[OH]D concentrations >50 nmol/l are considered replete, the current study identifies potential therapies to correct such vitamin D deficiency in only 6 weeks through supplementation with a minimum of 20 000 IU/week vitamin D3. We report no additional advantage of 40 000 IU/week to achieve a higher 25[OH]D concentration, or 12 vs 6 weeks if the target serum 25[OH]D is >75nmol/l. However, if >120 nmol/l is considered ‘optimal’, as has been proposed,43 then it should be noted that only one participant (from the 16 supplemented participants, ie, 6.25%) reached such a concentration following 12 weeks of vitamin D3 supplementation at 20 000 or 40 000 IU/week, and therefore higher doses of vitamin D may need to be given. It should also be noted that recent data suggest that values consistently in excess of 120 nmol/l may be associated with increased mortality risk compared to lower prevailing values of 50–60 nmol/l.44
We also observed that lower baseline concentrations resulted in a greater magnitude of response to supplementation in both the 20 000 and 40 000 IU/week groups. It is likely that the catabolism of 25[OH]D to 24,25[OH]D is accelerated with increases in 25[OH]D creating a threshold effect, and thus the initial ratio of 24,25 : 25[OH]D is a predictor of response to vitamin D3 treatment.45 Since 24,25 : 25[OH]D was not measured in the current study, this suggestion needs to be confirmed by future studies. Taken together, these findings highlight the need for an individualised approach to supplementation with vitamin D3 with baseline sampling being important in informing the extent of the chosen supplementation protocol.
We failed to identify any concomitant improvements in performance measures with increases in serum total 25[OH]D. It is possible that the endpoint serum total 25[OH]D concentrations achieved by our supplementation protocols may not have been optimal for muscle function. Although values above 50 and 75 nmol/l have been shown to improve physiological function and disease prevention,46–52 it is believed that the response curve of one tissue to a given extracellular signal (ie, hormone) differs from another. This implies that the optimal 25[OH]D concentration for a perceptible physiological response in one tissue may not be optimal for another.53 A higher serum total 25[OH]D concentration may be necessary in skeletal muscle, perhaps in the range proposed by Heaney54 (120–225 nmol/l), whereas in another tissue, a lower concentration is sufficient for a response. It would have been interesting to have included and monitored a more structured training plan for all of the participants to follow during the 12-week supplementation period, and future studies should consider this design. Alternatively, improving 25[OH]D concentration in healthy active young athletes may not induce a detectable improvement to muscle function such as that exhibited in elderly populations. A significant public health problem affecting the elderly is the condition of sarcopenia,55 defined as an age-associated loss of skeletal muscle mass and function, the causes of which are multifactoral.56 Sarcopenia affects all the elderly without discrimination between social status, gender or skin type,57 and therefore elderly participants may be more sensitive to improvements in muscle function induced by vitamin D supplementation due to underlying poor muscle function. To further ascertain whether vitamin D status does affect skeletal muscle function in young healthy participants, it may now be pertinent to also adopt more sensitive measurement techniques (eg, single muscle fibre measurements). Moreover, it may be necessary to perform studies using larger sample sizes powered based on detecting a moderate but meaningful change in athletic performance, although with the growing prevalence of vitamin D supplementation in athletic populations, these studies are becoming increasingly difficult to perform.
In summary, we report novel data that 20 000 IU/week vitamin D3 for 6 weeks is an effective supplement protocol to correct vitamin D insufficiency to levels defined as sufficient (serum total 25[OH]D concentration >50 nmol/l). We also observed that baseline serum total 25[OH]D concentration determines the magnitude of response creating interindividual differences, thus highlighting the need for an individualised approach to vitamin D supplementation. Despite correcting the deficiency and increasing the mean serum total 25[OH]D to greater than 75 nmol/l, supplementation had no significant effects on some markers of physical performance. Further studies may benefit from a greater dosage of supplementation protocols (to achieve greater than 100 nmol/l serum total 25[OH]D concentrations), longer supplementation protocols, larger numbers of athletes studied, as well as including more sensitive measurement techniques to more comprehensively examine the role of vitamin D on skeletal muscle contractile function. Moreover, future studies should monitor the dietary intake of vitamin D as well as attempting to quantify UVB exposure.
What this study adds
-
Serum total 25[OH]D can be significantly elevated to greater than 75 nmol/l after an acute 6-week supplementation period with 20 000 or 40 000 IU/week vitamin D3, although 40 000 IU results in a more rapid increase.
-
Twelve-week supplementation on 20 000 or 40 000 IU/week vitamin D3 does not improve skeletal muscle function in a young active cohort.
-
The increase in serum total 25[OH]D following oral supplementation in young active males is negatively correlated to baseline total 25[OH]D concentrations.
Acknowledgments
The authors would like to thank Ashley Lucas and Christian Bull for their help with the data collection, Jonathan Tang for his assistance with the serum 25[OH]D assessment and all of the participants for participating in the 12-week trial.
References
Footnotes
-
Contributors GLC and JPM designed and supervised the research as well as writing the manuscript. JL, MP, WB and DJO were responsible for the day-to-day running the research and contributed to the writing of the manuscript. WDF performed the vitamin D analysis and contributed to the writing of the manuscript.
-
Competing interests None.
-
Ethics approval Liverpool John Moores Local Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com