Article Text

Statistics from Altmetric.com
In 2007, Wilber1 presented the main altitude/hypoxic training methods used by elite athletes: ‘live high—train high’ (LHTH) and ‘live high—train low’ (LHTL); sleeping at altitude to gain the haematological adaptations (increased erythrocyte volume) but training at sea level to maximise performance (maintenance of sea-level training intensity and oxygen flux). The LHTL method can be accomplished through a number of methods and devices: natural/terrestrial altitude, nitrogen dilution, oxygen filtration and supplemental oxygen. Another method is the ‘live low—train high’ (LLTH) method including intermittent hypoxic exposure at rest (IHE) or during intermittent hypoxic training sessions (IHT). Noteworthy, all supporting references were conducted with endurance elite athletes (ie, cyclists, triathletes, cross-country skiers, runners, swimmers, kayakers and rowers) and there is an extensive literature relative to LHTH as well as LHTL. However, there is a lack of evidence for the applicability of these methods in team-sport athletes.
In recent times, media reports have provided us with coverage of some high-profile clubs or national squads in various team-sport disciplines undertaking fitness programmes at altitude during the early preseason or in preparation of a major competition. Despite the evident observation that athletes from different team sports and from all around the world are using altitude training more than ever before, it is stunning to note that to date there are only two hypoxic training studies that have been conducted with team-sport players.2 ,3 Therefore, there is an urgent need for mechanistic as well as applied studies investigating team-sport performance changes following hypoxic training in a sport-specific population before solid evidence-based recommendations can be definitely formulated.
In parallel, over the last few years, an increasing interest for the practical application of altitude training in team sports—mainly in football but also in the rugby union or the Australian football league—was noted due to several reasons. First, there were controversies regarding the possibility of playing international football matches above 2500 m in the mountainous regions of South America, while guaranteeing players health and safety. Second, the FIFA 2010 Senior (South Africa) and 2011 U-20 (Columbia) World Cups held at altitude have highlighted the need for the squads to achieve optimal acclimatisation. Third, the development of new hypoxic devices (eg, mobile inflatable hypoxic marquees) and methods (repeated sprints in hypoxia). This increased interest was translated by the organisation of international symposia on the topic by the leading sports organisation; for example, FIFA, symposium on playing football at altitude4; International Olympic Committee, consensus statement on thermoregulatory and altitude challenges for all high-level athletes.5 In March 2013, Aspetar Hospital invited several top international experts in the field of altitude training to establish a forum of research and clinical insights for the practical application of altitude training with team-sport players.
The intrinsic differences between factors underlying endurance (eg, maximal aerobic speed, economy) and team-sport performance (eg, repeated-sprint ability) as well as the constraints in the respective competition calendars explain why the aims and contents of the hypoxic methods and their periodisation in the yearly programme are largely different between individual and team sports. As such, we believe that the current nomenclature is probably not appropriate anymore for exploring the new boundaries of contemporary hypoxic methods offered to team-sport athletes. In 2010, we6 therefore proposed to slightly modify Wilber's nomenclature by introducing the possibility of combining different hypoxic methods. New approaches include ‘IHE during interval-training’ (IHIT = IHT + IHE) and ‘live high-train low and high’ (LHTLH = LHTL + IHT). Since more information became available on enhanced glycolysis and buffering capacity with IHT7 we discussed also the potential benefits of these hypoxic methods for anaerobic performance.
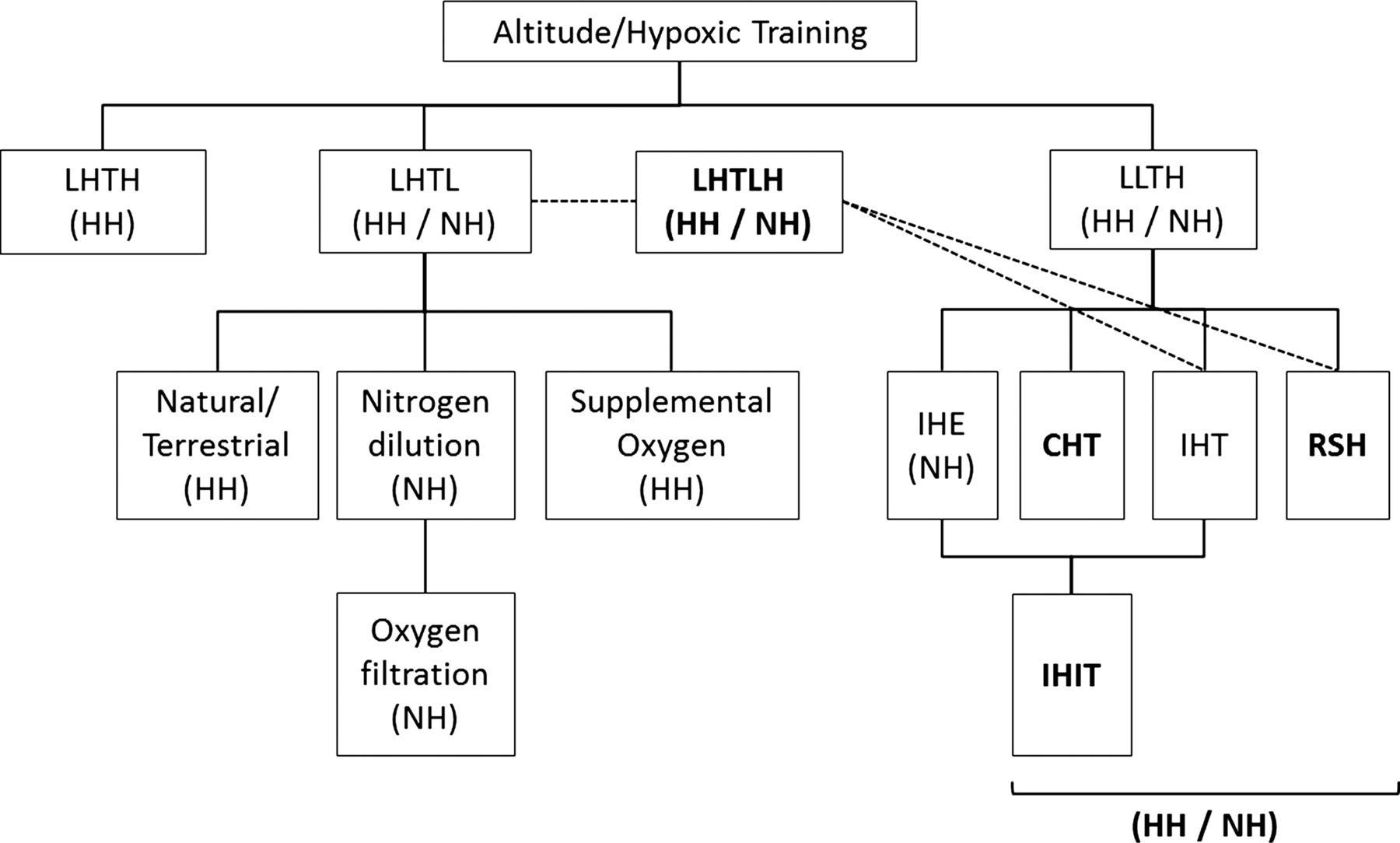
Unfortunately there is to date no expert consensus on how we should name the different hypoxic methods.6 IHT that should refer to interval training in hypoxia8 is also used for continuous low-intensity (<70% VO2max) long duration (>30 min) exercise in hypoxia.9 Recently, we also proposed a new hypoxic method (RSH, repeated sprint training in hypoxia) presumably based on different mechanisms than IHT.10 It is beyond the scope of this editorial to review the mechanisms underpinning these three subcategories of LLTH but, in our view, the time has come to update the current nomenclature since each method is likely based predominantly on different mechanisms; for example, increased oxidative capacity (CHT), buffering capacity (IHT) or compensatory fiber-selective vasodilation (RSH). Our suggestion is therefore to divide the LLTH method in four subsets; that is, IHE, CHT (continuous >30 min low intensity training in hypoxia), IHT (interval-training in hypoxia) and RSH (figure 1). Another point that deserves attention is the nature of altitude stress. If Wilber distinguished ‘natural/terrestrial’ and ‘simulated’ LHTL methods in his classification, such differentiation was absent for the LLTH methods. With mounting evidence suggesting that hypobaric hypoxia induces different physiological adaptations than normobaric hypoxia,11 we therefore believe that it is paramount to systematically report the method lowering ambient oxygen partial pressure.

{kind=link}
Updated panorama of the different hypoxic methods currently available for a range of athletes engaged in endurance and team–sport disciplines. Adapted from Wilber1 and Millet et al6 with proposed changes highlighted in bold. LHTH, live high–train high; LHTL, live high–train low; LHTLH, live high–train low and high; LLTH, live low–train high; IHE, intermittent hypoxic exposure; CHT, continuous hypoxic training; IHT, interval hypoxic training; RSH, repeated sprint training in hypoxia; IHIT, IHE during interval-training; NH, normobaric hypoxia; HH, hypobaric hypoxia.
Pending confirmatory research, we propose that not just one but a combination of various methods targeting different attributes of team-sport athletes over the course of the yearly plan would be more beneficial. It is our hope that the possibility of combining various hypoxic training methods—as described in this editorial—would open unexplored research avenues (eg, preacclimatisation, maintenance of the gains following an altitude sojourn, accelerating return to play for injured players and/or preventing detraining during the off-season) supporting best practice of team-sport athletes.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.