Article Text

Abstract
Objective To conduct a comprehensive systematic review and meta-analysis of studies assessing the incidence of concussion in youth athletes. Specifically, we estimate the overall risk of concussion in youth sports and compare sport-specific estimates of concussion risk.
Design Systemic review and meta-analysis.
Data sources A search of Medline, Embase (1980 through September 2014), and SportDiscus (1985 through September 2014) supplemented by manual searches of bibliographies and conference proceedings.
Inclusion criteria We included studies if they met the inclusion criteria of study design (prospective cohort study), relevant sports identified from the literature (eg, American football, rugby, hockey, lacrosse, soccer/football, basketball, baseball, softball, wrestling, field hockey, track, taekwondo, volleyball and cheerleading), population (males and females ≤18 years old), and outcome (concussion).
Results Of the 698 studies reviewed for eligibility, 23 articles were accepted for systematic review and 13 of which were included in a meta-analysis. Random effects models were used to pool overall and sport-specific concussion incidence rates per 1000 athlete exposures (AEs). The overall risk of concussion was estimated at 0.23 (95% CI 0.19 to 0.28). The three sports with the highest incidence rates were rugby, hockey and American football at 4.18, 1.20 and 0.53, respectively. Lowest incidence rates per 1000 AEs occurred in volleyball, baseball and cheerleading at 0.03, 0.06 and 0.07, respectively. Quality of the included studies varied, with the majority of studies not reporting age and gender-specific incidence rates or an operational definition for concussion.
Conclusions There are striking differences in the rates of incident youth concussion across 12 sports. This systematic review and meta-analysis can serve as the current sport-specific baseline risk of concussion among youth athletes.
- Concussion
- Athlete
- Adolescent
- Young
- Sports
Statistics from Altmetric.com
Introduction
Participation in sports is popular among child and adolescent populations. An estimated 30–45 million children and adolescents participate in non-scholastic sports1 ,2 and over 7 million adolescents participate in high school sports in the USA each year.2 ,3 Despite high participation rates, sports-related injuries are common, accounting for almost 25% of all patients presenting to the emergency department (ED) with a head injury.4 Furthermore, the Centers for Disease Control and Prevention have reported that 20% of the estimated 1.7 million concussions that occur each year are sports-related.5 ,6
Concussion is a serious concern for youth athletes who engage in contact and collision sports, accounting for 3–8% of all athletes with sports-related injuries presenting to the ED.4 Although the scientific study of concussion has progressed rapidly in recent years, the literature is still evolving.7 ,8 While the literature on concussion in the adult competitive athlete has progressed dramatically, little attention has been focused on the young athlete and how this outcome varies across sports.9 ,10 Adolescent concussion is a common sports injury that has been underappreciated and mishandled.7 Evidence suggests that children and adolescents take longer to recover than adults after a concussion, often requiring a more conservative approach to management and return to play.7 Young athletes may also be more susceptible to concussions due to a larger head to body size ratio, weaker neck muscles and/or the increased vulnerability of the developing brain.11
Although a systematic review of concussion incidence in contact sports has been completed, we are not aware of a systematic review evaluating concussion incidence that focuses on youth athletes. Koh and Cassidy9 conducted a systematic review in 2002 on high school and adult competitive athletes, in which they reported an incidence rate of concussion in collegiate hockey, American football and professional rugby. This systematic review is over 10 years old and given the increased risk and growing concern for youth athletes, we performed a systematic review and meta-analysis of observational cohort studies reporting on the incidence of concussion among male and female adolescent athletes aged 18 years and younger. The primary aim was to estimate the overall risk of concussion in youth athletes participating in any sport and to compare sport-specific estimates of concussion risk across sports.
Methods
Data sources and searches
We performed this systematic review using a predetermined protocol and in accordance with published guidelines for reporting of observational studies.12 We identified all potentially relevant articles regardless of publication language by searching Medline between 1980 and September 2014, Embase between 1980 and September 2014 and SportDiscus between 1985 and September 2014. Searches were enhanced by scanning bibliographies of identified articles and review articles, as well as reviewing conference proceedings from the International Conference on Concussion in Sport and the Sports-Related Conference on Concussion and Spine Injury within the past 10 years. Using the strategy recommended for systematic reviews of observational studies we searched the electronic databases using four comprehensive search themes. Theme 1 included terms to identify relevant outcomes: ‘concussion’ or ‘brain injuries’ or ‘brain concussion’ or ‘head injury’ or ‘mild traumatic brain injury’. To identify relevant sports (Theme 2), we included the terms: ‘Sports’ or ‘Sport’ or ‘Athlete’. Theme 3 included terms to identify relevant populations: ‘Adolescent’ or ‘youth’ or ‘Child’ or ‘School’ or ‘Students’. To identify relevant study designs (Theme 4), we included the terms: ‘Prevalence’ or ‘Cohort Studies’ or ‘Cross Sectional Studies’ or ‘Follow-up Studies’ or ‘Incidence’. For each theme, terms were searched as text words (or title/abstract words) or database-specific subject headings when available. These four themes were then combined using the Boolean operator ‘and’ to complete our search strategy (see online supplementary file 1). Experts in the field were also contacted for information about other ongoing or unpublished studies.
Study selection
Two individuals (KP and TP) independently reviewed identified abstracts for eligibility. All abstracts reporting original concussion incidence data among children ≤18 years old were selected for full-text review. This initial stage was intentionally liberal; we only discarded abstracts that clearly did not meet the aforementioned criteria. Inter-rater agreement was measured with the κ statistic. Disagreements were resolved by consensus.
The same reviewers then performed a full-text review of articles that met the inclusion criteria and of articles for which there was uncertainty regarding eligibility. Full text articles were retained if they met the inclusion criteria of study design (prospective cohort study), relevant sports identified from the literature (American football, rugby, hockey, lacrosse, soccer/football, basketball, baseball, softball, wrestling, field hockey, track, taekwondo, volleyball and cheerleading), relevant population (males and females ≤18 years old), and outcome (concussion). We chose not to enforce a strict definition of concussion for the purposes of this review, since the definition of concussion has been subject to change over the years. Imposing a limited definition of concussion such as one resulting from direct or blunt trauma to the head may affect the selection of relevant articles. The International Conference on Concussion in Sports includes direct blows to the face, neck, or other body areas that transmit impulsive forces to the head in its definition of concussion.13 Our primary intent was to determine the incidence of concussion in children ≤18 years of age participating in any sporting activities and to assess how the risk varied across sport. We elected to exclude articles that reported prevalent, rather than incident cases of concussion and studies that included chronic traumatic brain injury.
Data extraction and quality assessment
Both reviewers independently extracted data from all studies that fulfilled the inclusion criteria; disagreement was resolved by consensus. Attempts were made to contact authors of studies when data were unclear. The following data were extracted: number of participants, age range, number of concussions, denominator (person time at risk or number of athlete exposures (AEs)), and the incidence rate of concussion. A component approach was used to evaluate study quality and potential threats to validity. We adapted the Newcastle-Ottawa Scale for the assessment of study quality of observational studies.14 Specifically, we assessed how study cohorts were selected and measured, whether study results were stratified by important factors in their analysis (including age and sex), and how the outcome of interest (concussion) was ascertained and measured, including duration of follow-up, whether concussion was defined, how concussion was reported, mechanism of injury reported, and history of concussion reported.
Incidence rates
Determination of time at risk for injuries is reported in several different ways. The two most common denominators reported in the studies included in this review were AEs and player hours. Player hours can be an accurate measure of person time at risk, since it takes into account the actual time spent at risk for sustaining an injury. Although determining the exact time spent at risk is optimal in determining injury rates, this method is difficult or near impossible to use in studies at the high school level or with large central databases.15 An athlete exposure constitutes one player participating in any game or practise, regardless of the amount of time spent playing and therefore at risk of sustaining an injury.15 While this method may overestimate person time at risk and subsequently underestimate the incidence rate of injury, the use of AEs is common and relatively easy to calculate, provided that researchers use reasonable assumptions for the number of games or practices an athlete may be exposed to. For this review, we chose to pool only those studies reporting AEs as this method was the most commonly reported particularly for studies reporting on more than one sport. This allowed us to maximise the number of studies pooled for each sport. We did not pool in the event of single studies reporting on the outcome of interest or if the measure of exposure was in player hours, with the exception of hockey. Converting one form of person time at risk to another proves difficult, without making several assumptions including the number and duration of games and practices and length of playing season for the sport under study.
Data synthesis and analysis
The incidence of concussion along with denominators used to calculate rates was identified in each study. For small rates (when the numerator is small or denominator very large), the calculated lower limit of a CI may fall below 0 based on a Gaussian distribution. To ensure that all 95% CIs were between 0 and 1 the Wilson score interval was calculated using a binomial distribution.16 ,17 This has been shown to be suitable for studies with small sample size and/or extreme probabilities. To obtain a pooled estimate of the incidence of concussion per 1000 AEs, we used DerSimonian and Laird random effects model. Separate random effects models were developed to estimate the sport-specific incidence rates for all sports with two or more unique studies. Gender-specific estimates were also provided where available. Pooling was limited to studies reporting AEs, with the exception of hockey. In an attempt to compare the incidence of concussion in hockey (where three of four studies reported a denominator of player hours) to the incidence of concussion in other sports reported in AEs, we converted player hours to AEs for this sport. To do this, we took the sample size in each study involving hockey and multiplied it by the average number of games and practices in a week (1 game and 1 practice/week) and then by the average number of weeks in a season (20 weeks). Finally, we calculated an overall incidence rate across all sports. This was done by initially pooling within sport and then taking each sport-specific estimate and pooling these together with a random effects model. To visualise the incidence rates and corresponding 95% CIs within and across sports, we generated a forest plot for all sports with two or more unique studies. The Q and I2 statistics were also calculated to assess for heterogeneity with the underlying expectation that there would be substantial heterogeneity both within and across sports. All analyses were performed using STATA 12.0 (Statacorp, College Station, Texas, USA). For all statistical tests, p<0.05 was considered statistically significant.
Results
Identification of studies
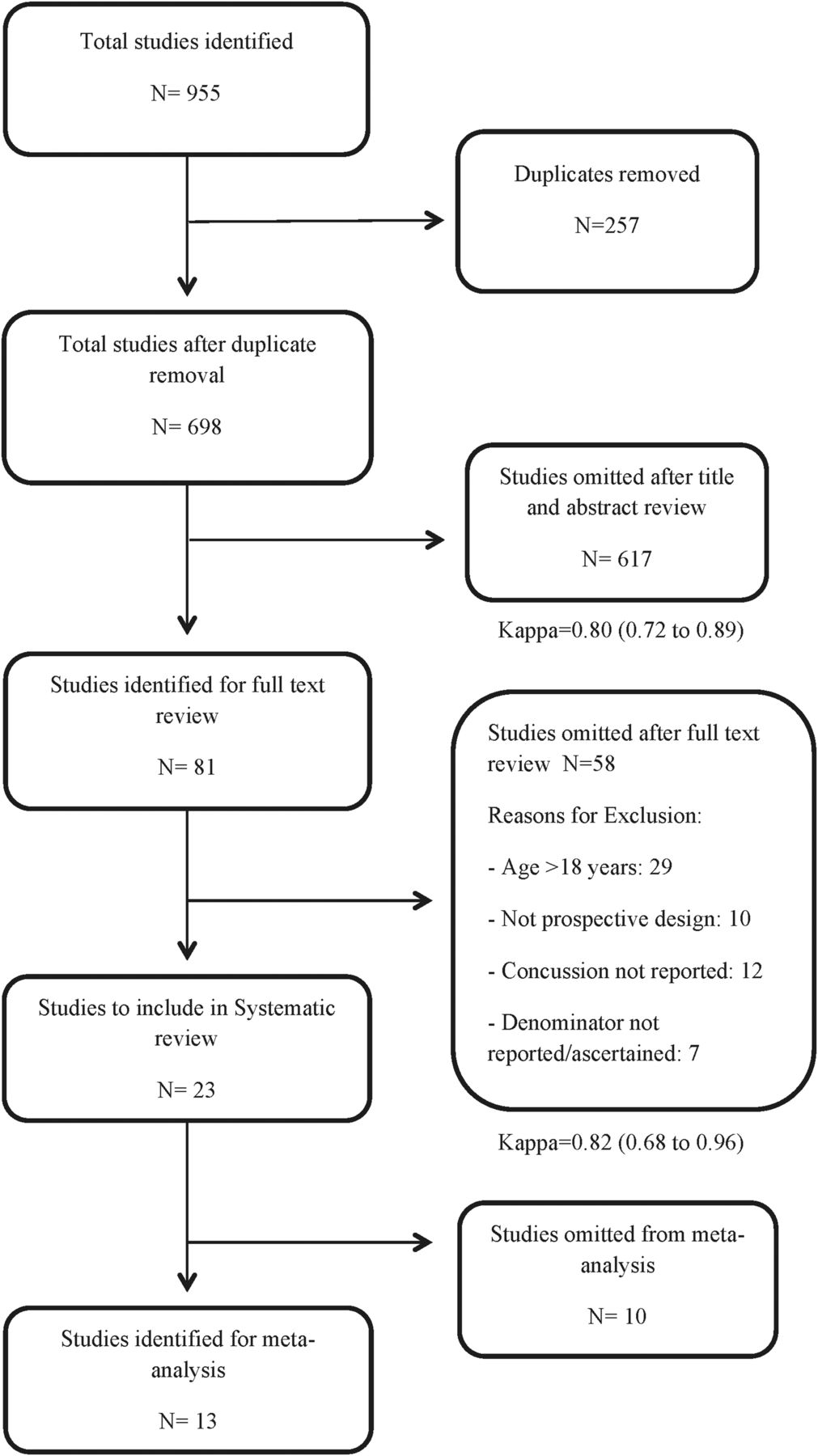
The progress through stages of the systematic review is outlined in figure 1. Our initial search yielded 698 unique citations. After an initial screen, 81 met criteria for full-text review (κ=0.80 95% CI 0.72 to 0.89). On review, an additional 58 were excluded (κ=0.82 95% CI 0.68 to 0.92), resulting in 23 studies available for the present review. When duplicate reporting of the same cohort of participants was identified, we selected the original article reporting on the incidence of concussion. In one study the female specific concussion incidence was reported previously and only the male incidence of concussion was used.18 Reasons for exclusion were: (1) age greater than 18 years of age or studies of college athletes (that contained participants 18 years of age or younger) but the incidence of concussion for those 18 years of age or less could not be determined, (2) study was not a prospective design, (3) the number of concussions was not reported, (4) the denominator used to calculate rates was not reported or could not be determined from available data. As such, 23 studies reporting on the incidence of concussion in youth sports were used for the present review.18–40 Of these, 13 were included in the meta-analysis.21–24 ,27 ,29–33 ,37 ,38 ,39 No unpublished or ongoing studies were identified.
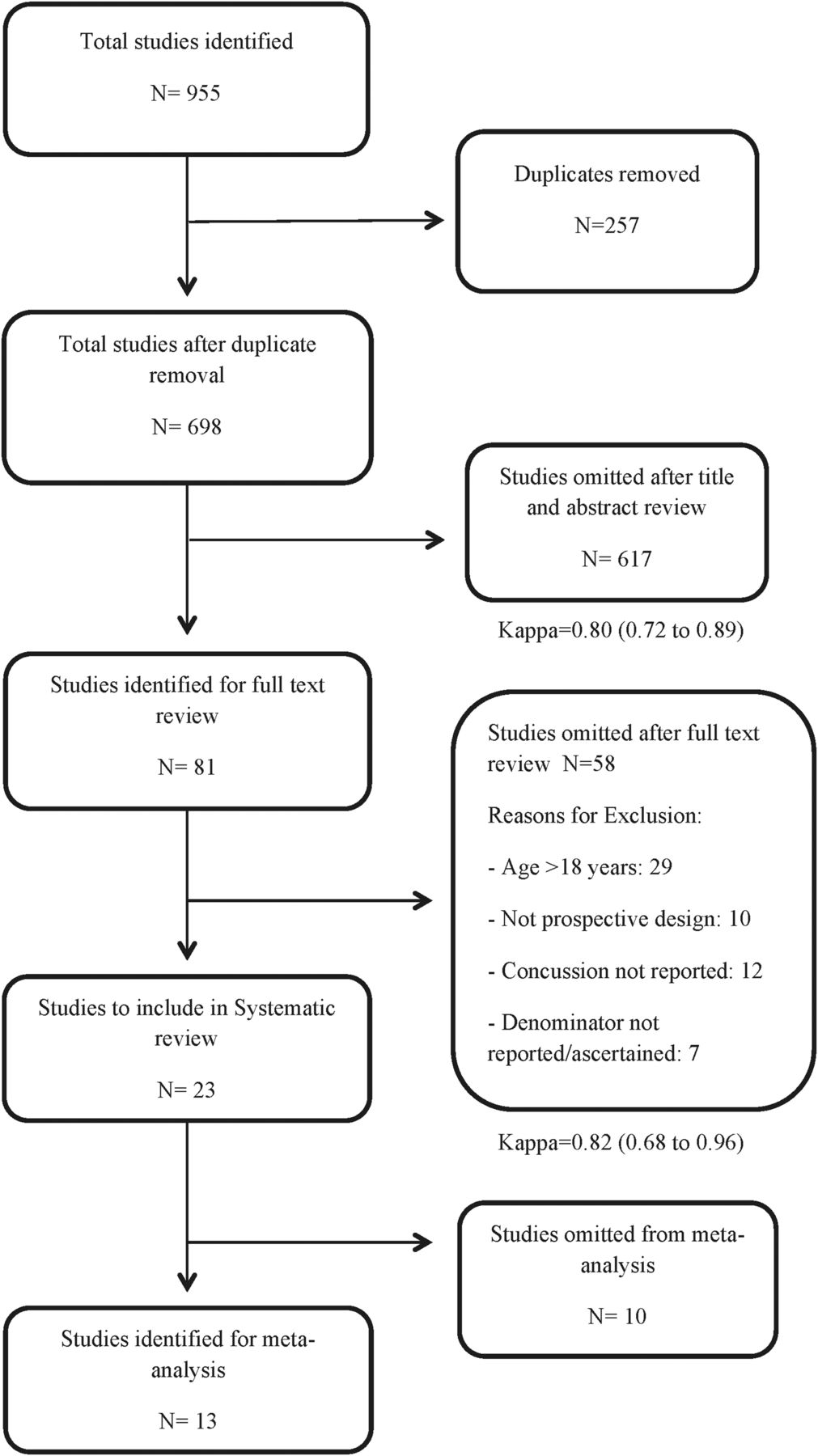
Study flow diagram.
Details of included studies
Online supplementary table S1 shows details of the studies that met our inclusion criteria. The publication dates ranged from 1992 to 2013, with the number of sports per study ranging from 1 to 9. In total, 14 sports were identified. These include American football (n=9), rugby (n=4), hockey (n=4), lacrosse (n=3), soccer/football (n=4), basketball (n=6), baseball (n=4), softball (n=4), wrestling (n=4), field hockey (n=2), Australian Rules Football (n=1), taekwondo (n=1), volleyball (n=2) and cheerleading (n=2). Sixteen of the 23 studies were based in the USA. Only 12 of the 23 studies reported an age range (range 6–18 years). Seven of the 23 studies did not report the total number of participants included (range 145–15 802 participants). Not all studies reported data on all outcomes of interest. Two of the 23 studies did not report the total denominator by sport and in these studies we recalculated the denominator using the number of concussions reported and the incidence per 1000 AE. Furthermore, not all studies reported the same denominator used to calculate rates. Twelve of the 23 studies reported AEs as the denominator, 8 studies reported player hours, 1 study reported team games, 1 study reported player games and 1 study reported the number of athletes as the denominator.
Study quality
The quality of the studies varied (see online supplementary table S2). With respect to cohort selection, all 23 studies appear to have a representative exposed cohort. However, only 15 studies (65%) provided adequate information and stratification by important factors such as age or sex. Thus it is difficult to assess the generalisability of the study findings or comment on differential risk by age and sex across the various sports identified. With respect to the quality of outcome measures, 11 of the 23 studies (48%) reported a definition of concussion. Sixteen studies involved a team trainer reporting the number of concussions while five studies were able to obtain physician diagnoses of concussion. All 23 studies reported the duration of follow-up, but ranged from 1 to 11 seasons. Given this range, the limited number of studies per sport, and the varying level of contact that occurs across the identified sports, it is difficult to determine if differential follow-up time had an effect on the overall and sport-specific concussion estimates. Further, only 6 of 23 studies (26%) acquired information on history of potential concussion which may influence the risk of subsequent concussion. Given the variability in study quality and the number of sports identified in the review, no attempts were made to quantify the effect of these different constituents of study quality on concussion rates.
Incidence of concussion
Of the 23 studies included in this systematic review, the incidence of concussion varied greatly between sports. The lowest incidence of concussion was observed in sports with less physical contact (including basketball and cheerleading), while sports with a high degree of physical contact had the highest estimated incidence. These included rugby, American football and hockey. The highest incidence of concussion was reported in taekwondo. However, this was based on a single study using a sample of three tournaments and estimated a concussion incidence of 5.0 (95% CI 3.6 to 6.8)/1000 AE. Estimated incidence of concussion varied by the method used to measure exposure. In general, the incidence of concussion was lower in studies reporting player hours compared to AEs.
For a number of sports included in this review, there was only one estimate of concussion risk, including taekwondo and Australian rugby. Pooling of incidence rates was limited to those studies reporting in AEs and included sports with two or more unique studies. The pooled incidence of concussion per 1000 AEs across 12 sports in 13 studies using a random effects model was 0.23 (95% CI 0.19 to 0.28) (figure 2). There was significant heterogeneity in this pooled between-sport estimate (Q statistic: p<0.001). The incidence of concussion per 1000 AEs among the 12 sports included in the meta-analysis ranged from 0.03 in volleyball to 4.18 in rugby (see online supplementary table S3, figure 2). The top three sports with the highest incidence rates per 1000 AEs were rugby, hockey and American football at 4.18 (95% CI 2.50 to 5.86), 1.20 (95% CI 1.00 to 1.31) and 0.53 (95% CI 0.40 to 0.67), respectively. The lowest incidence rates per 1000 AEs occurred in volleyball, baseball and cheerleading at 0.03 (95% CI 0.00 to 0.05), 0.06 (95% CI 0.04 to 0.08) and 0.07 (95% CI 0.04 to 0.09), respectively. Within sports, 3 of the 12 indicated significant heterogeneity as defined by the Q statistic. These were American football (Q statistic: p<0.001), soccer/football (Q statistic: p<0.009) and wrestling (Q statistic <0.001). While gender-specific incidence rates were reported for a number of sports, only soccer/football, basketball and lacrosse reported both male and female incidence rates. Within these sports, the incidence of concussion was higher in males for lacrosse at 0.29 (95% CI 0.26 to 0.32) vs 0.17 (95% CI 0.15 to 0.20) for females while concussion rates were higher in females for soccer/football at 0.27 (95% CI 0.24 to 0.30) vs 0.19 (95% CI 0.16 to 0.21) compared to men and basketball at 0.17 (95% CI 0.15 to 0.19) vs 0.10 (95% CI 0.08 to 0.11) for men.

{kind=link}
{kind=link}
Forest plot of the pooled sport-specific concussion incidence rates for sports with 2 or more unique studies (random effects model).
Discussion
In this systematic review and meta-analysis of the incidence of concussion in children and adolescents aged ≤18 years, we determined pooled incidence rates of concussion per 1000 AEs for 12 different sports. The overall incidence of concussion across these sports was 0.23/1000 AE. The sports with the highest incidence rate of concussion were rugby, hockey and American football at 4.18/1000 AE, 1.20/1000 AE and 0.53/1000 AE, respectively. The sports with the lowest incidence of concussion were volleyball, baseball and cheerleading at 0.03/1000 AE, 0.06/1000 AE and 0.07/1000 AE, respectively.
Children and adolescents overwhelmingly participate in sports more often than adults, thus they incur the majority of sports-related concussions.2 ,41 It is estimated that concussions represent 8.9% of all high school athletic injuries, compared to 5.8% of collegiate athletic injuries.2 ,42 Furthermore, a number of studies have shown the rate of concussion in high school athletes is higher than that of older athletes.43–45 To complicate the issue, the incidence of concussion in youth and college athletes is likely to be underestimated.46 Under-reporting in these populations can occur due to failure to report symptoms out of fear of losing playing time and a lack of recognition by the coaches, trainers and athletes themselves.2 ,47 Furthermore, a number of studies have demonstrated that many athletes lack knowledge about what a concussion is and therefore may not report symptoms or seek care.2 ,48–50
The results of the present systematic review and meta-analysis are important to a number of different knowledge users. Youth athletes and their families can use this information to educate themselves regarding the level of risk of sustaining a concussion given participation in a particular sport. It is common knowledge that participation in sports such as rugby, American football and hockey can result in a concussion; however, this review has also demonstrated that sports such as volleyball, baseball and cheerleading carry an inherent risk of concussion as well, albeit the risk of sustaining a concussion is much lower in these sports compared to ones involving a high frequency of physical contact. Understanding the baseline risk of sustaining a concussion in a particular sport may help raise athlete, parent and coach awareness and improve concussion reporting.
Public health officials can use this information to address injury prevention strategies for those sports that carry a high risk of concussion. While the evidence that the use of protective equipment such as helmets can protect against a concussion is inconclusive, research has demonstrated that mouth guards are ineffective at reducing the severity of concussion.51 ,52 Thus, other strategies such as rule changes to reduce head injury incidence may be acceptable.13 However, these initiatives may need to be balanced against the need to preserve the nature of the game in question.13
For healthcare providers this information may be useful in guiding informed decision-making regarding appropriate medical care staffing and sport-specific safety. The National Athletic Trainers Association has estimated that only 42% of high schools have access to a certified athletic trainer.2 ,53 As such, many youth games are staffed by volunteer coaches and officials.5 The attendance of trained medical personnel at youth sporting events is rare, leaving the recognition and initial management of concussion to individuals with little or no training.2 ,54 Because of this, reduced identification of concussions may be more likely in youth sports compared with adult sports.2 Perhaps sports that carry the greatest risk of concussion should not be held unless staffed with trained medical personnel. Feasibility is an issue with potential increases in costs and resources, including the potential for reimbursement of trained professionals to attend all events. Few studies on sport related concussion have been done in youth athletes, thus clinicians may find themselves using guidelines and recommendations that pertain to adults. The youth athlete is more susceptible to concussion and takes more time to recover, thus it is important for clinicians to familiarise themselves with youth concussion management guidelines.13
Limitations
This review should be interpreted in light of its limitations. First, we found significant heterogeneity in the overall concussion estimate across all 12 sports. This heterogeneity was expected as incidence rates across different sports will vary due to differences in the level of contact within each sport, the level of competition within each sport under study, the age range of the athletes participating and differences in protective equipment used. Furthermore, gender can be considered as an important source of heterogeneity as females have a potentially greater risk of sustaining a concussion due to possible biomechanical differences such as reduced head and neck mass compared to males and females exhibit greater angular acceleration of the head and neck.55 For the few sports with gender-specific information, the incidence of concussion was greater in females participating in soccer/football and basketball, while males had greater rates of concussion in lacrosse. Second, by converting the incidence rate of concussion in hockey from player hours to AEs with an estimated two exposures per week, we reduced the original denominator and subsequently may have overestimated the incidence of concussion in hockey. Increasing the denominator by raising the practice and game estimate per week may slightly reduce the incidence rate observed for hockey to be more in line with those observed in American football. However, this would not change the overall findings of this review where rugby, hockey and American football carry the greatest risk of concussion. Third, three of the four studies reporting concussion incidence for hockey were conducted by the same research group (Emery et al). Given the potential for overlap across study cohorts, the generalisability of estimated incidence rates for this sport may be reduced. Fourth, sources of heterogeneity and the influence of study quality were not explored due to several important methodological issues in the studies reviewed and lack of available data. Characteristics such as the age range were not reported in several of the studies. Furthermore, several studies failed to identify whether concussions occurred during games or practices, the level of competition within each sport under study and whether participants reported a history of concussion. Finally, while there is significant heterogeneity within and across sports, we were underpowered to adequately explore sources of heterogeneity in this review given the limited number of studies available for each sport.
Future research
Additional work is necessary to delineate gender and age differences among children and adolescent concussion rates, as well as more sport specific studies to improve our knowledge of the differential risk that appears to exist across different youth sports. Furthermore, studies that focus on translating information regarding concussion education, awareness and identifying signs and symptoms in the youth athlete should be considered. Studies that prospectively examine risk factors for concussion in youth athletes are needed to develop preventative strategies. There is also a need to evaluate the efficacy of such preventative strategies as well as rehabilitation strategies following a concussion.
In conclusion, this systematic review and meta-analysis provides valuable insight into the incidence rates of concussion across 12 youth sports. These incidence rates may serve as the current sport specific baseline risk of concussion and can be used as a referent for those studies attempting to compare the incidence of concussion or reduce the risk of concussion in youth sport. Given the current concerns regarding the susceptibility and recovery from concussion in younger athletes, the focus of research on youth athletes is required. The ability to treat and mitigate the effects of a concussion once one has occurred is negligible. Therefore, it is vital that parents, coaches, healthcare providers and athletes understand the level of risk of sustaining a concussion given participation in a particular sport and educate themselves in the detection and assessment of concussion, as well as safe return to play principles.
What are the findings?
Research on sports-related concussion specific to children and adolescents is limited.
This systematic review and meta-analysis provide a summary of the current knowledge regarding incident concussion rates in youth athletes across 12 different sports.
The results show striking differences in concussion rates and can serve as the current sport-specific baseline risk of concussion among youth athletes.
How might it impact on clinical practice in the future?
Public health officials can use this information to address injury prevention strategies for those sports that carry a high risk of concussion.
For healthcare providers this information may be useful in guiding informed decision-making regarding appropriate medical care staffing and sport-specific safety.
Given that youth athletes are more susceptible to concussion and take more time to recover, it is important for clinicians to familiarise themselves with youth concussion management guidelines.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online table 1
- Data supplement 3 - Online table 2
- Data supplement 4 - Online table 3
Footnotes
Contributors All authors conceived the study and developed the protocol. KP and TP conducted the search, abstracted the data for analysis, and performed the statistical analysis. KP, TP and PER wrote the first draft of the manuscript. All authors had access to the data, critically reviewed the manuscript for important intellectual content, and approved the final version of the manuscript. All authors will act as study guarantors for the paper.
Funding WAG is supported by a Canada Research Chair in Health Services Research and by a Senior Health Scholar Award from Alberta Innovates—Health Solutions. None of the funding agencies played an active role in the preparation, review or editing of this manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Statistical code and data sets available from the corresponding author at peronksl@ucalgary.ca