Article Text

Abstract
Objective To produce a best evidence synthesis of exercise prescription used when treating shoulder pathology in the overhead athlete.
Design A systematic review of exercises used in overhead athletes including case studies and clinical commentaries.
Data sources MEDLINE, PubMed, SPORTDiscus and CINAHL from database inception through July 8, 2016.
Methods We examined data from randomised controlled trials and prospective cohort (level I–IV evidence) studies that addressed exercise intervention in the rehabilitation of the overhead athlete with shoulder pathology. Case studies and clinical commentaries (level V evidence) were examined to account for expert opinion-based research. Data were combined using best evidence synthesis and graded (A–F) recommendations (Centre for Evidence-Based Medicine).
Results There were 33 unique exercises in six level I–IV studies that met our inclusion criteria. Most exercises were single-plane, upper extremity exercises performed below 90o of elevation. There were 102 unique exercises in 33 level V studies that met our inclusion criteria. These exercises emphasised plyometrics, kinetic chain and sport-specific training.
Conclusions and relevance Overall, evidence for exercise interventions in overhead athletes with shoulder pathology is dominated by expert opinion (grade D). There is great variability between exercise approaches suggested by experts and those investigated in research studies and the overall level of evidence is low. The strongest available evidence (level B) supports the use of single-plane, open chain upper extremity exercises performed below 90° of elevation and closed chain upper extremity exercises. Clinical expert pieces support a more advanced, global treatment approach consistent with the complex, multidimensional nature of sport.
- Shoulder
- sports rehabilitation programmes
- athlete
- exercise rehabilitation
Statistics from Altmetric.com
Introduction
According to the National Collegiate Athletic Association (NCAA) Injury Surveillance System, over a 16-year span, across 15 sports, upper extremity injuries accounted for 18.3% and 21.4% of game and practice injuries, respectively.1 Overhead athletes are at high risk for injury, with up to 30% of intercollegiate overhead athletes suffering a shoulder injury at some point in their athletic career.2 While the literature is dominated by shoulder injuries suffered by the throwing athlete, shoulder pain is the most frequent orthopaedic injury suffered in both men’s and women’s collegiate swimming and diving with a reported prevalence ranging from 34.7% to 66.7%, according to the NCAA injury surveillance programme.3 4
Given the high prevalence of shoulder pathology, overhead athletes are likely to seek treatment from a trained rehabilitation professional with the goal of returning to their respective sport at 100% function. The most common impairments seen in this population include strength deficits and motor control impairments, primarily found at the glenohumeral and/or scapulothoracic joints, resulting from the repetitive overhead demand of the sport, periscapular muscle fatigue, altered neurobiomechanics and subsequent injury.2 While there are a number of studies examining the effectiveness of conservative management for shoulder impingement syndrome (a non-specific term for many shoulder pathologies that cause shoulder pain when the arm is lifted overhead),5–7 the scientific evidence to support any specific exercise protocols for the overhead athlete is uncertain.
For the clinician, integrating the best evidence for practice addressing patient impairments, functional status and participation status required of an overhead athlete is a challenge. Current evidence-based guidelines7–16 for treating shoulder pain are non-specific to the overhead athlete population and are primarily based on populations of older adults, who typically have less rigorous functional and participation demands than overhead athletes. Therefore, the primary objective of this systematic review was to produce a best evidence synthesis of exercise prescription used to treat shoulder pathology in the overhead athlete.
Methods
This systematic review was conducted and reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA)17 using a research question that was informed by PICOS methodology. The PRISMA checklist for this study is available as an online supplemental file (online supplementary appendix A). PICOS is an acronym representing population (overhead athletes), intervention (exercise therapy), comparison (control group, comparison exercise), outcome (pain, strength, return to sport) and study design (randomised controlled trial, cohort study, case series).
Identification and selection of the literature
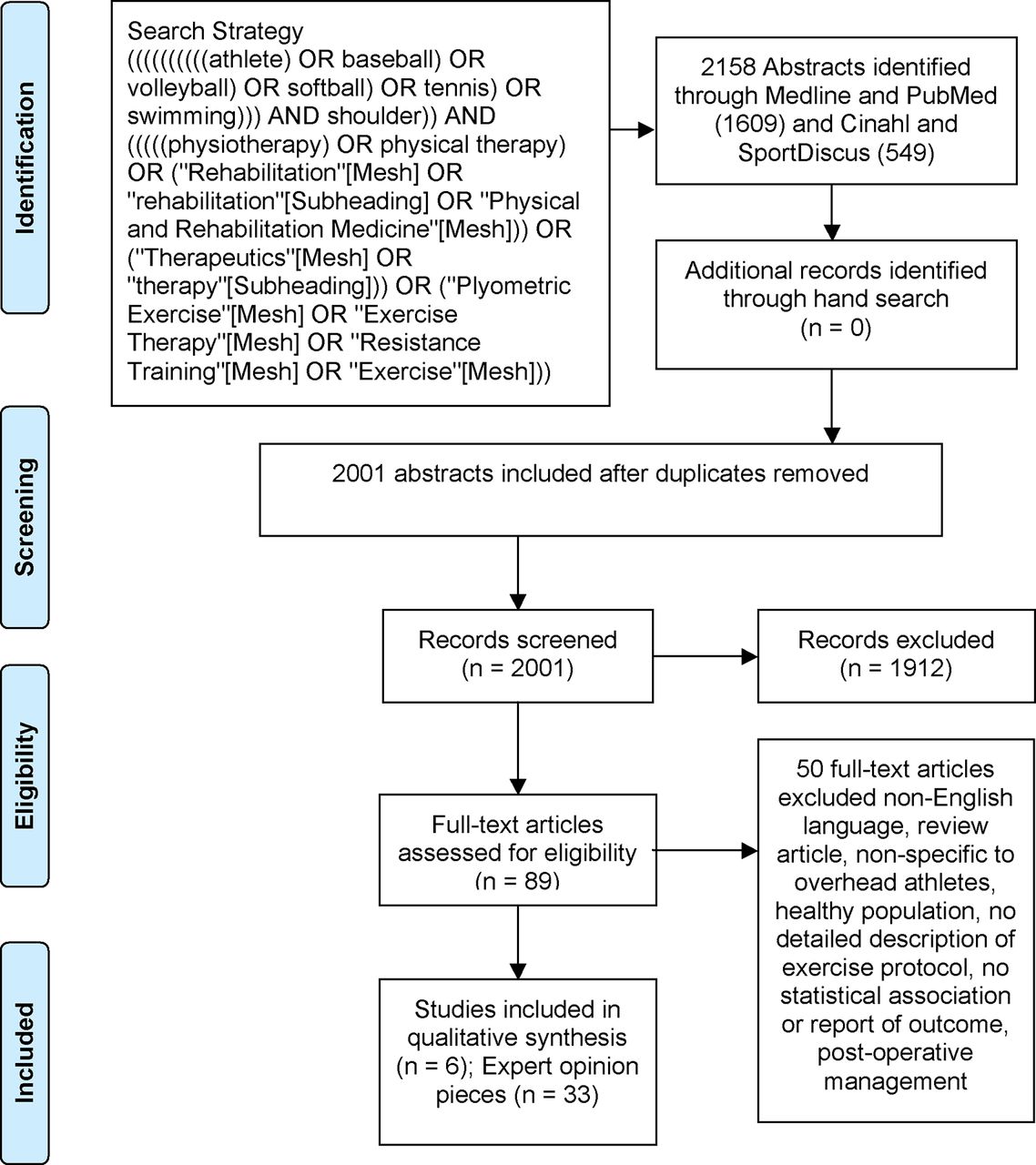
We searched the electronic databases MEDLINE, PubMed, SPORTDiscus and CINAHL from database inception through July 8, 2016. Sport-specific search terms were combined with exercise and rehabilitation search terms using the Boolean operator AND (figure 1). A hand search was also conducted which included the authors’ private collections, the reference lists of previous related systematic reviews, and the reference lists of selected abstracts not included in the original search criteria. Google Scholar was also searched using a combination of the sport name (eg, volleyball) and the term exercise.

{kind=link}
PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analysis) flow diagram of included studies.
Selection criteria
Because we anticipated limited high-quality evidence from randomised clinical trials, we included all study designs in our review. For a clinical trial, cohort study or case series (research-based evidence) to be included, it needed to meet the following criteria: (1) overhead athletic population; (2) population included a shoulder injury or shoulder pain; (3) detailed description of exercise interventions; (4) included an analytical component (ie, the study examined the effectiveness of an intervention on at least one level of impairment (eg, pain, strength, range of motion), function, or participation/return to play); (5) was available in full-text and (6) published in English language. Clinical commentaries, expert opinion, narrative reviews, consensus statements and clinical practice guidelines (expert opinion-based evidence) published by experts in the field of sports medicine were included if they (1) reported on the non-operative management of shoulder pathology in the overhead athlete; (2) had a detailed description of the exercise intervention and (3) identified a specific exercise or approach different from that provided by clinical trials, cohort studies or case series. Experts were defined as having had at least 5 years clinical experience treating overhead athletes as a specialty focus or were identified as a board certified clinical specialist in Orthopaedic or Sports Physical Therapy, or its international equivalent.
Cadaver or non-human studies were excluded. Studies were also excluded if participants had a history of stroke or hemiplegia, the exercise intervention was not described in sufficient detail to be reproduced in a clinical setting (eg, patient positioning, shoulder positioning), a full-text version of the abstract was unable to be located, the association between an exercise intervention and an outcome was not examined (for clinical trials, cohort studies or case series), or the topic of the paper was postoperative management. For the purposes of limiting repetition and over-representation of expert opinion pieces, multiple manuscripts published by the same author were screened for inclusion only if additional, unique exercises were included.
To identify relevant articles, titles and abstracts of all database-captured citations were independently screened by at least two authors (AAW, SLD, DTT) applying the a priori selection criteria. Full-text articles were retrieved if the abstract provided insufficient information to establish eligibility or if the article passed the first eligibility screening. In situations where disagreement concerning whether to include an article occurred, the three authors discussed the issues and came to a consensus. All criteria were again independently applied by two authors (AAW, SLD) to the full text of the articles that passed the first eligibility screening. In case of disagreement, a consensus method was used to discuss and solve the disagreement. In the event that agreement could not be reached, a third author (EJH) served as the deciding vote.
Risk of bias assessment
Risk of bias (for clinical trials, cohort studies and case series) was independently assessed by two reviewers (SLD, DTT) using the modified Downs and Black18 19 checklist for non-randomised studies (online supplementary table 1). The modified Downs and Black checklist is comprised 27 items, each with a yes/no/unable to determine answer option. Ten items related to reporting of overall quality of the study, three items to external validity, seven items to study bias, six items to confounding and selection bias, and one item related to the power of the study. Disagreements among the reviewers were resolved by consensus. The maximum score on the modified Downs and Black checklist was 28. Item 5 had a possible score of 2 if scored ‘yes,’ 1 if scored ‘partially’ and 0 if scored ‘No.’ The total score was the count of all of the criteria that scored ‘yes.’ ‘No’ and ‘unable to determine’ carried a zero score value. For each study, a total quality score was given based on the information provided. Based on risk of bias assessment scores, studies were classified as high quality/low risk of bias (≥20), moderate quality/risk of bias (17–19) or low quality/high risk of bias (≤16).20 Higher modified Downs and Black checklist scores indicate less risk of bias than lower scores. No formal risk of bias assessment was performed for expert opinion pieces. Quality of included expert opinion pieces was based on our definition of expert as previously defined.
Modified Downs and Black checklist (risk of bias assessment) for the six cohort, clinical trial studies
Data extraction
For articles reporting original data, four reviewers (AAW, DTT, SCR and SLD) independently extracted information and data regarding study population, study design, exercise interventions, outcome data (eg, mean change; p value) associated with the intervention, study quality and level of evidence. Any discrepancies were resolved during a consensus meeting. Three reviewers (AAW, DTT and SLD) categorised exercises as:
upper extremity exercise ≤90° of elevation
upper extremity exercise >90° of elevation
closed chain upper extremity exercise
unspecified upper extremity exercise
isokinetic exercise
plyometric exercise
kinetic chain/core/lower extremity exercise
sport-specific exercise.
Rather than assuming patient and shoulder-specific positioning, named exercises that failed to identify specific positioning were classified as unspecified. Authors were contacted by email to clarify the shoulder position for exercises classified as unspecified.
For expert opinion pieces (clinical commentaries), data extraction and tabulation of prescribed exercises followed the same format as original data articles, with categorisation of exercises according to phases of exercise progression. Data were extracted from expert opinion pieces on two grounds: (1) the manuscript identified a specific exercise or approach different from that provided by clinical trials, cohort studies or case series; and (2) in instances where multiple manuscripts were identified with the same lead author, data were only extracted from each additional manuscript if a new exercise was introduced.
Best evidence synthesis
We used the 2009 Centre for Evidence-Based Medicine (CEBM)21 levels of evidence for interventions to synthesise the data (http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/) since they allow ranking of evidence to include expert opinion. We modified these criteria so that level I was indicative of evidence from a randomised controlled trial; level II indicated a cohort study; level III indicated a case–control study; level IV a case series; and level V a case study or expert opinion to include clinical commentaries.
Results were dichotomised into exercises from (1) CEBM levels I–IV, and (2) CEBM level V, to allow comparison and comment on research-based recommendations versus more clinically based recommendations. For convenience, all identified shoulder exercises were tabulated and categorised under common clinical phases of progression (open chain below 90° of elevation; open chain above 90° of elevation). Finally, the strength of the entire spectrum of evidence was considered using a modified version of the CEBM ‘Grades of Recommendation.’ In our modified version, an A–F grading system was used: A signifies consistent findings in >2 level I studies; B—consistent findings in >2 level II or III studies or ≤2 level I studies; C—findings from >2 level IV studies or ≤2 level II or III studies; D—findings from >2 level V studies; and F—conflicting findings or findings from ≤2 level V studies. Level of evidence was downgraded one level for any study rated as having a moderate or high risk of bias by the Downs and Black criteria due to the greater uncertainty of the clinical applicability of the findings. In this final stage of the synthesis (assigning of A–F grade), exercises categorised as ‘unspecified’ were not included as we could not confidently detail specifics related to how exercises were being performed.
Results
The database search, along with reference checking, yielded a total of 39 studies (3 prospective cohort,22–24 2 randomised cohort,25 26 1 case series27 and 33 expert opinion28–60) for inclusion in the systematic review (figure 1). Fifty studies were excluded as they were non-specific to the overhead athlete population; they failed to provide a detailed, reproducible description of the exercise intervention; they reported on postoperative management; or they failed to report any statistical analysis between the exercise intervention and any outcome measure (for clinical trials, cohort studies and case series).
A detailed summary of the study characteristics is shown in online supplementary appendix B. Of the six research-based studies, three reported on shoulder impingement22 25 27 and three on shoulder pain or inhibition due to pain.23 24 26 Reported sporting events included baseball, volleyball, tennis, canoe polo, swimming, badminton and handball. A total of 191 athletes (118 male, 73 female) were studied. Reported outcomes were primarily at the impairment level with strength changes (including changes in peak torque) reported most commonly followed by subjective pain report. One study27 used a functional outcome measure, the Shoulder Pain and Disability Index. No ‘return to play’ outcomes were reported in any of the included studies. An analysis of the effects of specific exercise components contained within the overall rehabilitation protocol was precluded due to insufficient data.
Downs and Black checklist results for the research-based studies ranged from 12 (42.9%)24 to 19 (67.9%)26 out of a possible 28 (table 1). Three studies were classified as moderate risk of bias25–27 and three studies were classified as high risk of bias.22–24 Three of six included studies were prospective single cohort designs. Two studies25 26 used a randomised design including an experimental versus control group. One study was described as a case series.27 All six included studies had a moderate to high risk of bias. Most methodological shortcomings concerned external validity (items 11, 12 and 13); internal validity study bias (items 14 and 15); and confounding selection bias (items 21, 22, 23, 24, 25 and 26).
Summary of CEBM level I–IV studies
Thirty-three unique exercises were identified among the six research-based studies that met our inclusion criteria for exercise interventions in the overhead athlete (table 2):
Prescribed exercises from higher levels of evidence (CEBM I–IV) included in the systematic review
11/33, 33% of prescribed exercises were single-plane, upper extremity exercise ≤90° of elevation.
3/33, 9% of prescribed exercises were upper extremity exercise >90° of elevation.
6/33, 18% of prescribed exercises were upper extremity exercise, closed chain.
13/33, 39% of prescribed exercises were upper extremity exercise, unspecified.
Summary of CEBM level V studies
We identified 102 unique exercises from expert opinion pieces28–60 (online supplementary table 2):
20/102, 20% of prescribed exercises were single-plane, upper extremity exercise ≤90° of elevation.
8/102, 8% of prescribed exercises were upper extremity exercise >90° of elevation.
10/102, 10% of prescribed exercises were upper extremity exercise, closed chain.
4/102, 8% of prescribed exercises were upper extremity exercise, unspecified.
8/102, 8% of prescribed exercises were isokinetic exercises.
17/102, 17% of prescribed exercises were plyometric exercises.
20/102, 20% of prescribed exercises were kinetic chain/core/lower extremity exercises.
15/102, 15% of prescribed exercises were sport-specific (for basketball, throwing, baseball, tennis and swimming).
Best evidence synthesis of exercise prescription for the overhead athlete based on CEBM ‘Grades of Recommendation’
There is level B evidence to support the use of both open chain upper extremity exercise performed below 90° of elevation and closed chain upper extremity exercises with overhead athletes with shoulder pathology (table 3). This recommendation is consistent across level I–V studies.
Best evidence synthesis in support of exercise prescription for the overhead athlete
There is level C evidence to support the use of open chain upper extremity exercises performed above 90° of elevation with overhead athletes with shoulder pathology. This recommendation is consistent across level I–V studies.
There is level D evidence to support the use of isokinetic exercises of the upper extremity plyometric exercises, kinetic chain/core/lower extremity exercises and sport-specific training with overhead athletes with shoulder pathology (see online supplementary table 2 for examples of specific exercises). This recommendation is supported by level V studies alone.
Discussion
There was limited evidence to support the use of any specific exercise intervention in overhead athletes undergoing rehabilitation for shoulder pathology. Compounding the problem is the fact that the published literature is of moderate quality, at best. Current advice regarding exercise prescription for overhead athletes is reported mostly as clinical commentaries or general topical review articles by field experts without strong research-based evidence. In addition, many studies including overhead athletes and outcome data were excluded because they did not report a detailed description of the rehabilitation protocol used. There is also a preponderance of evidence focused on individual muscle activation patterns while performing specific exercises (eg, forward flexion in side lying for the middle trapezius)61 but these studies are limited because they lack transference of specific exercises as part of a rehabilitation programme to functional outcomes or improvements.
The strongest available evidence (grades B and C) supports the use of single-plane, upper extremity exercises performed below the 90° horizontal (eg, shoulder external rotation in neutral, prone extension) with some incorporation of elastic resistance for exercise prescription in the overhead athlete with shoulder pathology. Expert opinion (level V evidence) included a wider variety of exercises with greater attention to the kinetic chain. Exercises identified by clinical experts had a stronger focus on kinetic chain/core/lower extremity and plyometric exercises, and sport-specific training programmes for basketball, throwers, baseball, tennis and swimming.
There is a gap between clinical practice and research, with clinical experts using more complex exercises that have yet to undergo rigorous research trials to support their use as ‘evidence-based’ interventions. This gap can partially be explained by the idea that explanatory clinical trials typically are designed to capture intervention efficacy under ideal conditions whereas pragmatic trials attempt to understand the benefits under actual clinical conditions. The challenge for the researcher is gaining level I evidence while maintaining focus on how more complex interventions are being delivered in clinical practice.62
One problem with current research-based evidence is that documented existing programmes continue to focus solely on the shoulder without addressing the global demands placed on the trunk and lower extremity prior to return to play. Overhead athletic performance is not isolated to a single event or joint. Maximising force development in the large muscles of the core and legs produces more than 51%–55% of the kinetic energy that is transferred to the hand.63 Overhead throwing motion is a complex activity, involving the shoulder, trunk, spine and lumbo-pelvic-hip complex, that is achieved through the activation of the kinetic chain,63 to allow the sequential transfer of forces and motion. The throwing motion is a fluid, continuous movement that begins with the feet, which provide contact with the ground, maximising the ground reaction force, and creating a stable base for distal arm mobility.63
A blinkered exercise approach (focusing on the shoulder and neglecting the rest of the body) to a complex system-wide activity may be partially responsible for reinjury rates.64 Level V evidence supports incorporating global exercises (eg, lateral lunges with shoulder abduction/external rotation with a resistance band, lateral planks over Theraball) into sport-specific rehabilitation programmes.44 56 However, research-based evidence to substantiate these rehabilitation components is needed for confident transfer into clinical practice. In addition, research-based evidence is needed to support the sensorimotor component (speed, position, plane, load and duration) of current rehabilitation programmes challenging the athlete’s ability to stabilise the system both statically and dynamically while performing their specific athletic event.
Implications for clinical practice
We identified 135 unique exercises from research-based evidence and expert opinion. This catalogue of exercises is meant as a reference resource, not a recipe book, to be used when developing a comprehensive rehabilitation programme. In general, we found grade B evidence in support of exercises we identify primarily as early-phase rehabilitation exercises: single-plane, open chain exercises below 90o of elevation and closed chain exercises. The quality of the evidence started to suffer when we identify exercises as a progression or advanced phase rehabilitation. Only grade C level evidence exists for the incorporation of exercises performed above 90o of elevation in overhead athletes. This is important because function above 90° of shoulder elevation is a key requirement for the overhead athlete. Plyometrics and sport-specific training was supported by expert opinion alone (these exercises have not been assessed in the research-based evidence), which is surprising given that the overhead athlete requires dynamic function that encompasses speed, power and endurance.
The preferred method of exercise progression used by level I–IV evidence was based on progressive overload.25 27 This is a one-size-fits-all approach that does not adequately account for tailoring exercise prescription to the individual, although this approach allows for the standardisation necessary for rigorous research. This is in contrast to the exercise programmes recommended by clinical experts,54 56 which incorporated progressive phases (acute, intermediate, advanced return to sport). Level V evidence considered the complex nature of sport (speed, load, duration) and attempted to address this with complex interventions. However, this makes it more difficult to standardise the intervention.
The disparity between research and clinical practice may encourage newer clinicians who search published literature to either practice in a fashion that does not resemble expert practice or to seek evidence primarily in the form of expert opinion. While we acknowledge the importance of early and accurate activation of isolated musculature (eg, prone shoulder extension), these exercises do not account for the complex functional demands of the overhead athlete. If the clinician only looks to the currently available research-based evidence for exercise therapy to treat the overhead athlete with shoulder pathology, he or she would find him/herself relying on basic exercises used in the early stage of recovery to alleviate impairments, and without guidance regarding progression to functional outcomes including return to sport. Expert clinical reasoning is considered a vital part of evidence-based practice.65–67 By synthesising research-based and expert opinion-based evidence, we provide additional insight into exercises used by practising clinicians that have yet to undergo rigorous research trials to support their use as ‘research-based’ interventions.20 68
Injury and recovery from injury in athletes represents a dynamic system,69 where there are multiple internal and external factors, such that changing one affects all of the others.70 Rehabilitation should address the complex, dynamic and multidimensional aspects of injury and recovery with exercise prescription that is based on athletic movement and performance as well the incorporation of local (joint), regional (trunk and extremity) and global (system-wide and spinal, paraspinal and supraspinal) approaches. In the context of rehabilitation in the overhead athlete, we recommend the use of single-plane exercises below 90o of shoulder elevation in the early phases of rehabilitation, with a graduated progression that addresses the regional (plyometrics) and global (dynamic, triplanar activities) issues that adequately prepare the athlete for return to sport.
Future research priorities
We have identified five key issues to help address the gap between research-based evidence and expert opinion:
High-quality randomised controlled trials are needed for examining the treatment effectiveness of individual exercises used in the overhead athlete.
Individual exercises need to be compared in terms of treatment effectiveness to assist the clinician in selecting the most efficient exercises for their overhead athlete.
Authors must improve the reporting of used interventions so that clinicians are able to replicate these exercises.
Research studies must include more advanced exercises such as plyometrics and kinetic chain exercises to determine the effectiveness of these exercises.
For treatment outcomes, priority must be given to functional outcomes and return to play over impairment level outcomes (pain, strength) to capture the primary interest of the athlete.
Limitations
Of the 39 articles assessed, only six met the criteria as CEBM levels I–IV and there were no studies of level I evidence. Thirty-three of the 39 studies were rated as level V, expert opinion evidence. This limited the strength of recommendations we could make. Of the CEBM level I–IV studies, only one study used a validated self-report functional outcome measure,27 whereas the others primarily reported on outcomes at the impairment level only (pain, strength). None of the included studies reported return to play outcomes. We recognise the risk of publication bias as we only included published literature as well as language bias as we only included articles published in English. Last, we acknowledge that this review is dominated by exercises recommended by clinical experts, which at this time remains grade D evidence.
Summary
There is grade B evidence to support the use of single-plane exercises performed below 90° of shoulder elevation in overhead athletes with shoulder pathology. Advanced exercise prescription (eg, sport-specific training) for overhead athletes with shoulder pathology is supported by grade D evidence.
What is already known
Exercise therapy is an effective treatment approach for individuals with shoulder pathology.
A majority of reported exercises supported by the six level I–IV studies consist of single-plane, upper extremity exercise performed below 90o of shoulder elevation.
Athlete rehabilitation programmes have long been used by sports medicine experts as part of the rehabilitation process for the overhead athlete.
What are the new findings?
There is a mismatch between exercises supported by evidence-based research and exercises recommended by clinical experts when prescribing exercises for the overhead athlete with shoulder pathology.
There are no high-quality randomised controlled trials examining exercise prescription in the overhead athlete.
Grade C evidence exists for the incorporation of upper extremity exercises above 90o of shoulder elevation for overhead athletes.
Grade D (level V) evidence exists for the incorporation of isokinetics, plyometrics, kinetic chain/core/lower extremity, and sport-specific training for the overhead athlete with shoulder pathology.
References
Footnotes
Contributors All named authors assisted with the idea, development, data synthesis and analysis, writing, and revision of the submitted manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.