Article Text

Statistics from Altmetric.com
This journal aims to promote, publish and promulgate high-quality, innovative research. As laudable as this is, it is not enough. Unless this research culminates in practical and cost-effective interventions capable of attracting the political and social support required to allow effective implementation, it will not prevent harm or save lives.1
The Public Health Model has been proposed as a framework to promote the progression of sports medicine research towards real-world application.2 ,3 In this four-stage model, research progresses in a stepwise manner from problem identification to adoption of effective interventions:4
-
Stage 1: establishing the magnitude of the problem;
-
Stage 2: identifying risk factors;
-
Stage 3: developing effective interventions;
-
Stage 4: ensuring widespread adoption and use.
Unfortunately, most sports injury research does not result in adequate dissemination or widespread use of effective interventions.5 ,6 The problem is not unique to sports medicine. In a review of 1210 articles published in 12 leading public health and health promotion journals, Oldenburg et al7 found that 63% of publications were descriptive (Stages 1 and 2), 11% were concerned with method development and 16% were intervention-based (Stage 3), and only 5% were concerned with institutionalisation or policy implementation research, with less than 1% containing diffusion research (Stage 4).
While researchers have generated considerable knowledge from surveillance, risk factor identification and efficacy and effectiveness studies, this knowledge needs to be adopted by those who can use it to improve sports medicine practice (eg, clinicians, coaches and sporting bodies).1 ,8
Several gaps between injury prevention research and safety promotion practice hamper our efforts:9
-
the efficacy-to-effectiveness gap,
-
the research-to-practice gap,
-
the injury-prevention-to-safety-promotion gap.
These gaps stem from the contrasting approaches that researchers, policy makers, practitioners and the community take to the scientific, practical and social challenges posed by the contextual complexity of injury.9
The efficacy-to-effectiveness gap
There is a scientific problem. The transition from researching what works (ie, efficacy and effectiveness research) to how to make it work (ie, implementation research) is a critical step, but not straightforward.10 The problem emanates from the way researchers approach the problem of contextual complexity. Success at a population level, or effectiveness, is not solely determined by the efficacy of the intervention, it is also influenced by multiple inter-related contextual factors within the target group and in the community. This has led Green11 to conclude, ‘Where did the field get the idea that evidence of an intervention's efficacy from carefully controlled trials could be generalised as ‘best practice’ for widely varied populations and situations?’
Intervening within social systems, while remaining true to scientific principles, is a challenge for researchers. Reductionist science attempts to control the effects of contextual complexity by isolating the different components of a problem and studying each independently. A key assumption is that these determinants are statistically independent. Unfortunately, this assumption does not apply in human social systems where the interdependence of people and their natural, physical and social environment (ie, the capacity of individuals to influence each other, modify their environment and be influenced by their environment) is an essential characteristic of how these social systems work.9 ,12
Sports injury is a complex problem; however, complex is not a synonym for complicated. Complex systems consist of multiple and interdependent causal determinants that have unique scientific properties (eg, non-linear dynamics, self-organisation and phase transitions). Complex systems require a different scientific approach. Innovative health researchers are beginning to demonstrate promising results using the tools of complexity science such as multilevel analysis, network analysis, systems modelling and agent-based modelling.9
The research-to-practice gap
There is an implementation problem. The RE-AIM framework (Reach, Effectiveness, Adoption, Implementation and Maintenance)13 has recently been proposed as a reporting template to encourage sports researchers to document their research in a way that enables practitioners, policy makers and communities to use them effectively.8 ,14 ,15 However, while researchers report individual impacts of interventions, measures of the process of implementation, sustainability and population impact are frequently overlooked.16 In a systematic review of 27 articles of community-based interventions identified in 11 leading health journals, efficacy was reported in 100% and reach in 88% of articles.17 In contrast, implementation was reported in only 59%, adoption in 11% and behavioural maintenance in 30% of articles. No articles reported institutional maintenance. The situation is even worse for sports medicine research.18
The injury-prevention-to-safety-promotion gap
There is a political problem. The dissemination and widespread adoption of sports injury interventions are social objectives that can only be realised in the context of a community and the organisational and political processes that shape sports delivery. Public policy is set by those who can build enough consensus to intervene, not necessarily by proponents of ‘best evidence’.9 Evidence that is compelling for researchers may not be automatically accepted by those with the power to implement an intervention or a policy that improves uptake.19
Closing the gap
Communities are under increasing pressure to adopt evidence-based approaches to injury prevention. However, the accumulated experience from an array of research-to-practice initiatives has shown that practitioners find it difficult to adopt and sustain interventions in the real world that apparently worked in a research setting under ideal scientific conditions.20
When Mercy et al3 first proposed the Public Health Model for injury prevention, they advocated a bottom-up approach that engaged practitioners, policy makers and the community in helping to define the problem (Stage 1), identifying causes (Stage 2) and developing and testing interventions (Stage 3). Contrary to Mercy et al's3 advice, some researchers adopted a top-down approach, believing that Stages 1–3 of the Public Health Model are the province of scientific experts, while Stage 4 (dissemination, implementation and adoption) was the domain of community practitioners who were expected to take efficacious interventions and faithfully apply them to improve practice.21 This science-driven misapplication of the Public Health Model ignores the importance of engaging practitioners, policy makers and the community in the process of designing, researching and implementing effective interventions, falsely assuming that efficacious interventions can be automatically adopted and effectively implemented at a population level.6 ,9 ,16 Researchers who ignore the contextual, implementation and process determinants of intervention success should not be surprised if practitioners and the community are unwilling or unable to adopt evidence-based interventions to prevent sports injury.6 ,9
In the intense discourse between researchers and practitioners it is easy to forget a third group of stakeholders—the community. Sports injury is, after all, their problem! The community's perspective is not only important it is enlightening. The community will often understand the contextual barriers to effective implementation.9 These may be political, social or environmental. They can provide valuable advice regarding best fit, what is feasible, affordable and sustainable in their community. Sports researchers who ignore the community's perspective are destined to fail in the final critical dissemination and widespread adoption phase of the Public Health Model.6
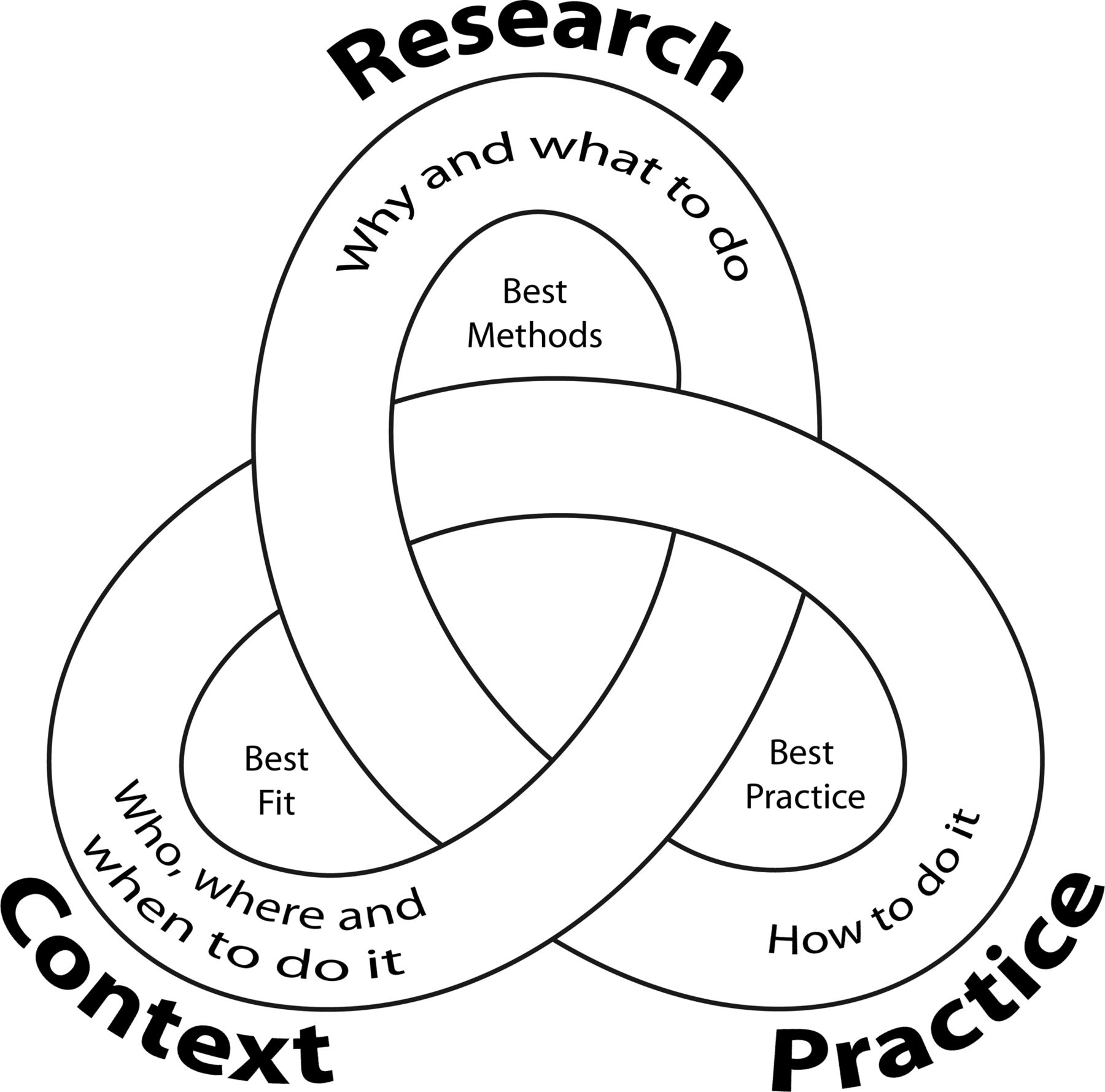
Three complementary types of experts, usually working in tandem, are necessary to design efficacious and effective interventions capable of being disseminated and adopted by the wider community:
-
researchers (ie, content experts),
-
clinicians, practitioners and policy makers (ie, process experts),
-
members of the target community, sports bodies (ie, context experts).
All three are necessary partners to achieve the sports injury prevention benefits we seek (figure 1). Each partner brings expertise that is critical to successful implementation of evidence-based practice. Integrating the expertise of all stakeholders is required to ensure that comprehensive, evidenced-based interventions are also practical and relevant to the real world of sports medicine.
{kind=link}
Integrating expertise to ensure comprehensive, evidence-based interventions that are practical and relevant when applied in the real world.
This problem is often framed as a need for better translation of research evidence into practice.8 ,15 However, there is also a need for better translation of evidence from practice into research.11 Perhaps the real barrier is not a lack of understanding, but a failure to listen! Good communication, good translation and indeed good research are necessarily a dialogue, a multidirectional conversation in which everyone's contribution is valued. If we could find the humility to listen we might be surprised to discover that policy makers, practitioners and the sporting community have valuable expertise that can enhance our research by making it more relevant, more practical and more applicable in the real world.
Conclusion
Sports injuries are largely preventable but discrepancies among researcher, practitioner and community perceptions of injury causation and the potentially feasible solutions for prevention are important barriers to mounting an effective response. It is not enough to understand what should be done but rather to understand what can be done and how it needs to be done. Injury prevention research that does not connect with the practical realities of implementation and adoption, and does not build the consensus needed to ensure effective implementation, will not prevent injury or improve health. From the very beginning, the combined expertise of researchers, practitioners and the target community is required if the application of the Public Health Model is to produce outcomes that will ultimately benefit public health and sports medicine.
References
Footnotes
-
Contributors Each author contributed to conception and design of the review, drafting the article or revising it critically for important intellectual content and final approval of the version to be published. This work does not necessarily represent the official views of the US Centers for Disease Control and Prevention.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.