Article Text

Abstract
Despite thoracic outlet syndrome (TOS) being first described early in the 19th century, the subsequent literature seems limited, focusing on case reports and investigations providing little assistance in the management of equivocal presentations. Best practice clinical management, with little evidence base, poses great challenges for clinicians in deciding how to manage TOS, when to operate and which procedure should be undertaken. Furthermore, the implications of TOS and its surgical effects are poorly documented, with little evidence in the literature as to the impact of surgical intervention on athletes and their physiology or function. This paper describes a clinical example of TOS highlighting salient issues and examining the evidence to guide clinical management at each stage, in the case of a 26-year-old professional football player who suffered an acute onset of unilateral right shoulder to bicep pain associated with tingling in the hand. Clinicians managing similar cases in the future will have a reference point to assist their diagnosis, management and promote much needed research to further our understanding of this difficult syndrome.
- Shoulder injuries
- Orthopaedics
- Neurology
- Muscle injury and inflammation
- Soccer
Statistics from Altmetric.com
Introduction
Thoracic outlet syndrome (TOS) is a challenging condition to diagnose and treat, and this may be reflected by the number of terms used to describe the collection of symptoms caused by compression at the thoracic outlet.1 There are two openings in the thoracic cavity; the superior outlet is known as the superior thoracic aperture and anatomically as the thoracic inlet. Interestingly, in clinical use, it is referred to as the thoracic outlet.2 Although there is disagreement as to what the specific composition of the ‘thoracic outlet’ involves, for clinical purposes it suffices to be described as an anatomical space created by the first rib, the clavicle, the subclavius muscle, the costoclavicular ligament and the anterior scalene muscle.3 The scalene hiatus is formed by the space between the anterior and middle scalene muscles through which pass the brachial plexus and subclavian artery.
Accordingly, there is a plethora of nomenclature used to describe specific subtypes of TOS reflecting the nature of compression at the thoracic outlet. The National Library of Medicine's controlled vocabulary thesaurus (Medical Subject Headings, or MeSH) lists 14 terms under ‘Thoracic Outlet Syndrome’. The extra descriptors relate to different terms used to describe the anatomical location (as in the example of ‘aperture’), the cause of the compression or the symptomatic effect of compression. Essentially, there are three recognised methods of classifying TOS4–7:
-
By event
-
Trauma
-
Repetitive stress
-
Postural abnormalities
-
-
By affected structure
-
Neurogenic TOS (NTOS)—compression of the brachial plexus nerves. This is the most common, comprising over 90% of all TOS cases.8
-
Arterial TOS (ATOS)—compression of the subclavian artery
-
Venous TOS (VTOS)—compression of the subclavian vein
-
-
By cause of compression
-
Scalenus anticus—compression on the neurovascular bundle by muscle growth/inflammation
-
Cervical rib syndrome—compression as a result of an accessory rib
-
TOS can have debilitating consequences for patients and can seriously diminish their quality of life. A recent article written by a patient, published in the BMJ, highlighted the difficulty in diagnosis, management and prognosis associated with some cases, as well as the effect it can have on patients’ lives.9
Evidence in the literature focuses on specific cases of TOS and its investigations, resulting in a lack of clarity on how to make evidence-based clinical management decisions. In addition, the implications of TOS and any surgery undertaken are not well understood. A 2010 Cochrane review highlights the paucity of available high-level data to guide the management of TOS in general, compounded by the lack of an agreed set of diagnostic criteria.1 As a result, there are very little data that can be extrapolated to guide management in the athletic community, and few opportunities to conduct randomised trials and high-level studies in the athletic subgroup. The aim of this paper is to describe a case of TOS in a professional athlete, discussing the evidence base for clinical decisions, teasing out key relevant clinical decision-making elements, while demonstrating knowledge gaps and limitations. Clinicians managing similar cases in the future will have a reference point to assist their diagnosis and management and promote much needed research to further our understanding.
Presentation
A 26-year-old footballer suffered an acute episode of right upper limb pain following routine training exercises. Four days later, he recalls waking ‘in agony’ with sharp, intense pain, feeling as though he had ‘tore (his) bicep’. The pain passed down the anterior aspect of his arm and was tender to palpation over the medial bicep. Throughout the day, the pain intensified until it was graded at 9/10 on the visual analogue scale with movement. At rest, it was 5/10 and described as ‘a dull ache’. This resulted in a significant restriction in function; abduction was limited to 30°, hindering daily tasks and his ability to train and compete.
An initial episode of sudden onset mild right arm pain 4 years previously was recalled, which started on waking and resulted in a constant ache lasting for 2 days. He was able to continue training by self medicating with non-steroidal anti-inflammatories. Medical advice was not sought as the pain was mild and resolved quickly. No other discerning features were recalled and the athlete had largely forgotten this episode.
On examination, pain was noticeably exacerbated by abduction and external rotation of the shoulder. There was a thickened supraclavicular fossa and a distinctly flat clavicle. Abduction at and beyond 30° exacerbated severe pain, both actively and passively. There was no muscle wasting. The pain would settle when the clavicle was pushed forward. Tapping the supraclavicular fossa was Tinel's positive with shooting pain down to the same hand. Furthermore, the right radial pulse was lost when the arm was abducted overhead (Adson's test).
Unfortunately, the symptoms associated with TOS are varied, vague and non-specific. There appears to be a lack of objective diagnostic criteria.10 There is described in the literature a collection of symptoms considered to be ‘true NTOS’ and these include weakness in the thenar, hypothenar and interossei with or without atrophy, as well as ulnar and medial antebrachial cutaneous hypaesthesia of the ipsilateral arm. This was described by Gilliatt et al in 1970 and has specific diagnostic criteria secondary to a cervical rib or band and is known as the Gilliatt-Sumner hand11 ,12; its management is proposed to be operative.11
The general symptoms of TOS still vary depending on the compressed structures. Neurogenic compression can include: pain, paraesthesia, numbness, tingling and weakness. Symptoms tend to be present for long periods of time before complications arise.6 ,8 Indeed, it is possible to have a tight thoracic outlet but without overt symptoms.13 The impact of NTOS can significantly reduce the quality of life. Physical Component Score surveys, indicators for functional health and well-being, had scores that seemed akin to those with chronic heart failure and worse than those with ATOS or VTOS.14
Differential diagnosis
Multiple differential diagnoses must be considered when reviewing a case with this presentation, all of which may cause unilateral, upper limb muscular pain exacerbated by movement.
Shoulder and rotator cuff: There may have been a mechanical problem and injury to the shoulder and rotator cuff. However, given the unusual presentation, unremarkable shoulder provocation tests and that the pain was described as burning and intense, associated with specific movements, a neurogenic cause was considered.
Cervical spine injury: There was a significant training history, so it was possible that the patient may have suffered a neck injury; however, the onset was acute; there was no history of trauma and the cervical spine movements were unremarkable. Plain radiographs were normal and the symptoms did not correlate with a spinal injury; an MRI scan of the shoulder and C-spine confirmed no abnormalities.
Neuralgic amyotrophy (NA): Typically described as an entity beginning with pain around the shoulder and upper arm, NA is characterised by episodic acute onset of pain and multifocal paresis, but the symptoms can vary widely.15 Over days or weeks, the pain can increase and muscle weakness and atrophy can develop.16–18 Reports show a slight preponderance of men over women, and age of onset in the early to mid 40s.17 ,19 ,20 The unusual demographic, lack of hypaesthesia and muscle wasting, countered the presence of NA, but these can be later signs of NA.16
Thoracic outlet syndrome
The symptoms correlated with TOS. The nature of the pain pointed to the existence of a mechanical cause. The relief provided when pushing the clavicle forward is likely to be a result of the thoracic outlet being opened, relieving impingement on the brachial plexus. The exclusion of other potential differential diagnoses supported this conclusion.
A lack of ischaemia or vascular symptoms excluded the presence of ATOS or VTOS, although vascular symptoms can occur in NTOS as a consequence to overactive sympathetic nervous fibres in C8–T1 being affected in the thoracic outlet.8 The value of Adson's test in diagnosing TOS is also limited, as it has been found to have a false-positive rate of 42%, is higher in individuals with carpal tunnel syndrome,21 and has been found to be negative in most cases of NTOS.8
Clinical appearances and provocation tests were suggestive of a dynamic transient and mechanical restriction of the nerves, which was supported by the presence of a flat clavicle, which is a risk factor for TOS.22 Neural tension testing suggested that the median nerve was the most affected.
Investigations
X-rays are useful to exclude the presence of cervical ribs and in the initial assessment of cervical spine abnormalities.
MRI
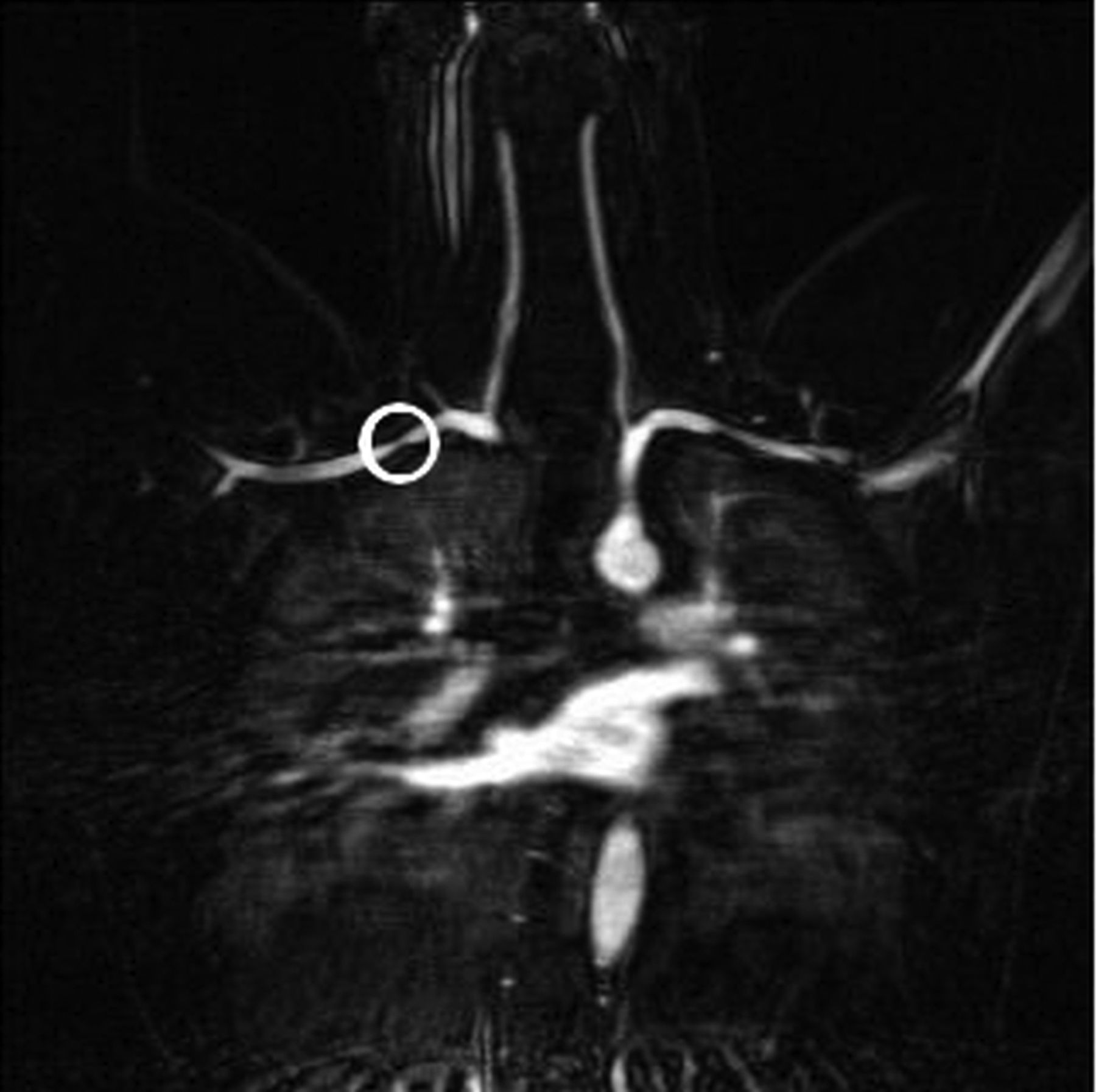
An MR angiogram (MRA), with the arm flexed and abducted to 90°, was performed (figures 1 and 2) which clearly revealed a constriction of the thoracic outlet and ‘apple core’ compression on the subclavian artery from above and below.

MRI scan of the thoracic outlet showing compression of the subclavian artery.

{kind=link}
{kind=link}
MRI scan of the thoracic outlet showing compression of the subclavian artery.
Positional MRI scans have been found to be very useful in identifying TOS and the impact on the neurovascular bundle.23–25 A paper in 2012 reviewing enhanced three-dimensional MRA with provocative manoeuvres has been shown to be efficacious in identifying stenosis in patients with symptoms of vascular TOS26 ,27 and those of NTOS, a vascular component that has been excluded in 61% of cases.26 Contrast-enhanced MRA is safer than digital subtraction angiography as it does not pose the same risks of nephrotoxicity or radiation.26 Unfortunately, with an MRA, the lack of dynamism makes it difficult to pinpoint the cause of compression and only shows its presence.
Ultrasound scan
Although known for its ability to identify flow disturbances in blood vessels,28 USs have been used for injecting the scalene muscle for several years.29 Neuromuscular US has been increasing in accuracy and quality, so much so that some have advocated its use in delineating the anatomy in TOS and have suggested using it as an adjunct to MRI scanning.30 Its use as a diagnostic or interventional tool is still being studied.31 Operative decisions can, however, be seen following careful dissection and thoracic outlet compression movements during surgery to determine the precise anatomical cause or causes of compression.
Management
Analgesia
Once the diagnosis of TOS was suspected, expert advice was sought from a peripheral nerve injury clinic. Primarily, analgesics including paracetamol, codeine, Arthrotec and Tramadol were prescribed incrementally, providing limited relief. Tramadol was discontinued due to side effects. Gabapentin use seemed to ease some of the pain, however it is unclear whether this reflected coincidental improvement with rest rather than pharmacologic benefit.
There is no research to guide clinical decisions on the use of analgesics in TOS. One paper referenced that opioid use in patients with NTOS was 29% in their sample of 87.32 The most significant discussion in the literature is the use of scalene blocks in NTOS, although many papers advocate their use as a diagnostic tool or predictor of operative success, rather than for pain management.10 ,14 ,32–36 One article in 2011 discusses the practices of a single clinician, who advises the use of a long-acting opioid in combination with a long-acting non-steroidal anti-inflammatory.37
Investigations supported the diagnosis of NTOS. Following multidisciplinary team discussions with the patient, conservative management was decided. The patient intended to rest for one month but symptoms worsened after two weeks rest, leaving surgery as a more viable option. Most literature describes the conservative route as being the recommended initial form of treatment.10 ,18 ,32 ,38–41
Surgery and rehabilitation
During the operation, a significantly enlarged scalenus anterior muscle was found, with fascial thickening, soft tissue scarring and local inflammation. The arm was mobilised to try and reproduce the positions of pain associated with a compressed thoracic outlet. This enabled the identification of dynamic anatomical impingement areas, which were found to be associated with the scalenus anterior. An intraoperative decision was made to release the posterior third of the scalenus anterior insertion, and perform a fasciotomy with release of adhesions. The first rib was left intact.
A diagnosis of TOS as a consequence of anatomy and enlarged anterior scalene was made.
Following a brief period of rehabilitation and mobilisation, the patient remains pain free and returned to full training and top-flight football within 6 weeks.
Interestingly, this case documents the experiences of a professional footballer, which for a predominantly lower limb sport is perhaps unusual. Of note, there have been two recent high-profile cases in premier league footballers of TOS causing thrombosis. Gary Cahill42 and Scott Sinclair43 were both reported in the media to have required urgent surgery and removal of a first rib.
The literature mainly documents the outcome of this treatment in non-athletes. The surgical option is available for TOS refractory to conservative management and sooner in emergency cases associated with thrombus; where an acute thrombus is not responding to thrombolysis, urgent surgery seems to improve outcomes.44 Generally, first rib removal surgery for TOS has shown promise and good results for patients.32 ,45 Quality of life has also been documented as having been improved and maintained at surgical follow-up.32
There have been several reported cases of professional athletes with TOS, although they are from sports requiring upper body strength, such as baseball and swimming. In one case, a competitive swimmer was found to have unilateral atrophy and weakness of the intrinsic muscles. Surgery was undertaken, during which the lower trunk was found to be compressed by a hypertrophied scalenus anticus containing a fibrous band. The muscle was sectioned and the lower trunk was neurolysed. This swimmer was advised to abandon competitive swimming.46 This paper also discusses eight other young athletes with varying neurology and vascular findings as a consequence of TOS. Of these, three were baseball pitchers, two swimmers and one an oarsman. The remaining two were adolescents suffering from TOS symptoms while participating in school sports activities and found to have cervical ribs. All cases apart from the swimmers responded well to conservative management. The two swimmers were also found to have a hypertrophied scalenus anticus and were successfully treated with scalenectomies. A similar case was described in 2007 by de Almeida et al where a competitive swimmer was found to have a true NTOS. This case was treated surgically, excising a fibrous band in the thoracic outlet and leaving the first rib and the scalenus anticus (which was not hypertrophied) intact. This case, however, did gradually improve function.47 This paper discussed a series of seven swimmers with similar symptoms and surgeries. Of these, six had surgery, five of whom improved as a result. Three had hypertrophied scalenus anticus and scalenectomies, two had first rib removal and one had excision of a fibrous band. Most recently, another competitive swimmer was found to have a tight thoracic outlet with a subclavian thrombus that was treated with first rib resection. Unfortunately, there were some complications with an injury to the long thoracic nerve resulting in a winged scapula. It took 5 months to regain function in the upper limb before being able to ‘participate in all desired activities with no restrictions’.48 No follow-up data or outcomes for any of the cases were reported or discussed.
Similarly, another case of a baseball player with symptoms of TOS was diagnosed by MRI, showing a hypertrophied subclavius muscle and obstruction of the subclavian vein. Surgery was performed, the first rib was resected and a vein graft applied as a thrombus was found.27 Another college baseball player was found to have similar symptoms, except that he was treated conservatively. Initially, he was diagnosed by arteriography, highlighting hypertrophy of the scalene and pectoralis minor muscles. After 6 months of conservative treatment, he returned to a similar level of activity without pain.49
Conclusion
Most patients who suffer TOSs have an anatomical predisposition. An association with the brachial plexus and compression or friction on the nerves passing through the thoracic outlet will occur if there are any causes for a tighter outlet. In severe cases, impingement can occur at low functional levels, and we speculate that it is possible that these individuals self-select by participating in sports that avoid provocative overhead arm movements or do not become athletes at all, which may represent a ‘subclinical’ TOS. Similarly, some people will develop hand paraesthesia when sleeping with their arm above the head and avoid provocation by adopting alternative sleep positions. However, in athletes, especially where the use of the arms and scalene muscle hypertrophy are likely to be greater, they may be at an increased risk of TOS, with smaller anatomical variations putting them at risk of compression. Surgery seems to play an important role in resistant cases.
It is important to consider differential diagnoses and the limited evidence base when managing athletes with TOS, noting that immediate surgery is usually recommended for emergencies and associated arterial thrombus. Initially, we would recommend conservative management and monitoring for at least 1 month, regularly assessing for symptomatic improvement with rest. If symptoms improve and a return to activity is possible, then conservative treatment should be maintained. However, if there are no benefits, deterioration or an inability to return to sport (or normal and routine daily activities), then surgery should be promptly considered, reducing the risk of long-term neural damage and potential arterial thrombosis. It seems prudent to opt for exploratory and dynamic surgery, when possible, to identify the specific cause of the thoracic outlet compression in cases where diagnosis is unclear and treatment is not urgent, before electing to remove ribs. Careful dissection and mobilisation of the arm is necessary to identify the specific anatomical cause, or causes, of impingement, resecting only those structures. Unfortunately, there remains little evidence regarding the athletic consequences of first rib removal or other surgical interventions.
The challenges associated with researching rare conditions in professional sport can lead to confusion and difficulties for clinicians and patients seeking to make best practice management decisions. Prolonged periods of reduced activity and rest associated with conservative management pose many challenges to the athletes, clinicians, coaches and employers. More research is needed to assess the management options for TOS in athletes as significant knowledge gaps remain and the implications of surgery on livelihood and the quality of life can be significant for professional and recreational athletes. Similarly, more research is required into the functional and performance effects of rib resection in the general population and athletic community. The outcomes of these studies are needed to help guide sport and exercise medicine physicians, team physicians, surgeons and patients in the management of this difficult syndrome.
It will be important to catalogue and monitor these challenging cases to develop further knowledge and inform clinical management decisions, enabling us to better advise and inform our athletes on the advantages and disadvantages of management decisions.
What is already known on this topic
-
Thoracic outlet syndrome (TOS) management in most cases can be managed conservatively with good success. More stubborn cases of TOS respond to surgical intervention, especially in the cases of known anatomical variations (eg, cervical rib).
-
Unfortunately, there are two groups of patients for which management and planning are unclear: some cases of chronic or persistent TOS with no anatomical cause that do not respond to classical treatment, and cases involving athletes. The consequences for athletes in terms of physiological outcomes, route to surgery and best indications for surgery or conservative management are largely unknown and anecdotal.
What this study adds
-
This paper organises and consolidates the management decisions for thoracic outlet syndrome in athletes analysing the evidence available and reviewing the literature on each key management decision encountered.
What are the new findings?
-
A structured evidence review for key clinical management decisions is proposed.
-
Research gaps are identified and clinical relevance for athletes is discussed.
How might it impact on clinical practice in the near future?
-
This paper will help guide clinicians managing thoracic outlet syndrome.
Acknowledgments
The authors would like to thank the athlete for agreeing to publish his case and images, and for spending time talking to the team in the hope that his case will help others in a similar situation.
References
Footnotes
-
Contributors RW and AR coordinated the treatment programme, and HT was the main author of the manuscript. MS was involved in the management of the patient and contributed to appropriate sections of the manuscript. All authors contributed in the feedback and editing process.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.