Article Text

Abstract
Objective Exercise training has been shown to have beneficial effects on liver function in adults overweight or with fatty liver disease. To establish which exercise programme characteristics were likely to elicit optimal improvements.
Design Systematic review and meta-analysis of randomised, controlled trials.
Data sources PubMed, CINAHL and Cochrane controlled trials registry searched (1966 to 2 October 2015).
Eligibility criteria for selecting studies Exercise intervention, with or without dietary intervention, versus usual care in adults undertaking, exercise training, who were overweight, obese or exhibited fatty liver disease (non-alcoholic fatty liver disease or non-alcoholic steatohepatitis).
Results We included 21 randomised controlled trials, totalling 1530 participants. Exercise intervention studies with total exercise programme workload >10 000 kcal produced significant improvements in intrahepatic fat, −3.46% (95% CI −5.20% to −1.73%), p<0.0001, I2=73%; effect size (standardised mean difference, SMD) −1.77 (−3.11 to −0.42), p=0.01, I2=77%. When data from only exercise studies were pooled, there was a reduction in fasting free fatty acids (FFAs) −74.15 µmol/L (95% CI −118.47 to −29.84), p=0.001, I2=67% with a large effect size (SMD) −0.94 (−1.36 to −0.52), p<0.0001, I2=0%. When data from only exercise studies were pooled, there was a significant reduction in insulin MD −1.88 UL (95% CI −3.43 to −0.34), p=0.02, I2=31%. The liver enzymes, alanine aminotransferase, aspartate aminotransferase and γ-glutamyl transpeptidase, were not significantly altered with exercise.
Conclusions Exercise training reduces intrahepatic fat and FFAs while increasing cardiorespiratory fitness. An aggregate exercise programme energy expenditure (>10 000 kcal) may be required to promote reductions in intrahepatic fat.
- Evidence based review
- Liver
- Meta-analysis
- Prevention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Central obesity is linked to raised serum liver enzymes and future risk of developing insulin resistance.1 Fatty liver disease (FLD) and non-alcoholic fatty liver disease (NAFLD) are also associated with increased serum levels of liver enzymes.2 FLD may be diagnosed through liver function tests and imaging, such as MRI or ultrasound of the liver, to detect excess intrahepatic fat. Exercise can greatly assist in reducing obesity and FLD, mainly by improving weight loss through dietary changes and exercise and reducing alcohol consumption.3
Obesity and FLD are risk factors for diabetes and cardiovascular disease. The prevalence of FLD varies greatly from a 10% to 35% prevalence rate in the USA with ∼2–5% of patients with non-alcoholic steatohepatitis (NASH),4 the more severe form of NAFLD.
A 2012 systematic review by Thoma et al5 examined the effects of diet and exercise on liver function, but although data pooling was not performed, the authors concluded that dietary-induced weight loss may offer greater liver health benefits than exercise. A 2012 systematic review, of randomised and non-randomised controlled studies in obese and FLD populations, by Keating et al examined intrahepatic liver fat content and alanine aminotransferase (ALT). The pooled analysis reported that the former, but not the latter, was reduced with exercise training of 4–26 weeks duration.6 A number of new studies, including two studies with >100 participants,7 ,8 have been published after Keating et al's analysis. Moreover, Keating et al pooled data from different modalities of exercise (aerobic and resistance) and did not adjust for the great variation in exercise programme durations (1–12 months), frequency (2–7 sessions weekly) and intensity. There are now sufficient randomised controlled trials available to conduct analyses of several additional outcome measures and to adjust for variation in exercise programme characteristics to identify those that are most beneficial in patients with obesity and FLD. Furthermore, liver enzymes may not be sensitive enough to be the only measure of liver function or liver fat,9 so new studies mean other markers can be examined.
The primary aim of this work was to conduct a systematic review and meta-analyses to establish the effect of exercise training on surrogate markers of liver function in adults who were overweight or exhibited FLD. The secondary aim was to establish if there is an exercise programme volume more likely to elicit optimal improvements in related health outcome measures.
Materials and methods
Search strategy
Potential studies were identified by conducting a systematic search using PubMed, http://www.ncbi.nlm.nih.gov/pubmed (1966 to 2 October 2015); the PubMed search strategy can be seen in supplementary files. CINAHL and the Cochrane controlled trials registry were also searched (1966 to 2 October 2015). The search strategy included the key concepts of overweight, obese, FLD, NAFLD, NASH, lifestyle therapy, physical training and exercise training. These were combined with a sensitive search strategy to identify randomised controlled trials (see online supplementary figure S1). Titles and abstracts were screened by NAS and GD, and full-text articles were downloaded for those meeting inclusion criteria. Reference lists of papers found were also scrutinised for new references. All identified papers were assessed independently by two reviewers (GD and NAS); a third reviewer (JRM) was consulted to resolve disputes. Searches of published papers were also conducted up until 2 October 2015.
Supplemental material
Inclusions
Randomised controlled trials of progressive aerobic, resistance or combined exercise training in adults (>18 years) who were overweight or obese or exhibited FLD (NAFLD or NASH) were included. The definition of obese/overweight was made by the individual studies, but this was verified by checking baseline data. Combined exercise training was defined as interventions that used both aerobic and resistance training simultaneously. We included studies comparing two types of exercise (eg, aerobic vs resistance) or exercise versus usual care. Included studies employed three sessions or more of exercise, in order to differentiate from acute exercise effects. Studies involving dietary control or intervention groups were included only if the diet was the same between exercise and control groups allowing the independent effects of exercise to be examined. There were no language restrictions.
Exclusions
Animal studies, review papers and non-randomised controlled trials were excluded. Studies with unmatched intervention versus control group participants were excluded. We also excluded studies of healthy, normal body mass participants as liver function was likely to be normal. Authors were contacted to provide missing data or to clarify if data were duplicated in multiple publications. Incomplete data, or data from an already included study, were excluded. Studies using interventions other than exercise (eg, electroacupuncture, ultrasound) were excluded.
Data extraction
Data on outcome measures were archived in a database; data were extracted by NAS and verified by GD; JRM was consulted if discrepancies occurred. The outcome measures were: change in intrahepatic fat (percentage change), ALT, aspartate aminotransferase (AST), γ-glutamyl transpeptidase (GGT), free fatty acids (FFAs), body mass and body mass index (BMI), insulin, total cholesterol and peak VO2 (table 1). We calculated energy expended by establishing oxygen consumption at the training intensity and using 5 kcal/L of oxygen consumed, thus establishing kcals expended per minute. We then multiplied kcals/min by session duration (min) and then multiplied this by total number of sessions to calculate aggregate energy expenditure for each exercise programme, this is an approach we have used previously.10 ,11 ,12 We also conducted analysis of effects on interhepatic fat (IHF) only in exercise programmes that expended an aggregate of >10 000 kcal.
List of outcome measures and other data extracted from included studies
Data synthesis
The meta package in R V.3.2.1 was used to complete the meta-analysis and generate forest plots (Schwarzer G. Meta: General Package for Meta-Analysis, in R package. 2015) (Team RC. A language and environment for statistical computing. R Foundation for Statistical Computing. 2015: Vienna, Austria). Pooled data are presented as mean differences (MDs) and as the effect size Hedges' g, that is, standardised mean differences (SMDs) with 95% CI for intervals with a significant MD. We chose a random-effects model as we anticipated considerable heterogeneity. A minimum of three studies was required for meta-analysis to be undertaken. Multivariate meta-analysis (using the metafor package)13 with a random intercept for study was used for studies that compared more than one intervention group with a control.
Meta-analyses were completed for continuous data by using the change in the mean and SD of outcome measures. It is an accepted practice to only use postintervention data for meta-analysis, but this method assumes that random allocation of participants always creates intervention groups matched at baseline for age, disease severity, etc. Change in postintervention mean was calculated by subtracting baseline from postintervention values. Data required were either (1) 95% CI data for pre–post intervention change for each group or when this was unavailable; (2) actual p values for pre–post intervention change for each group or if only the level of statistical significance was available; (3) we used default p values, for example, p<0.05 becomes p=0.049, p<0.01 becomes p=0.0099 and p=not significant becomes p=0.05.
Effect sizes are interpreted in the usual way14 with an effect size of 0.2 defined as small, 0.5 defined as moderate and 0.8 or higher defined as large.
Analyses
Where sufficient studies were included, meta-analysis was performed for the following groups (1) aerobic versus resistance training studies, (2) exercise only versus control studies and (3) exercise plus diet versus diet control studies.
Several subanalyses were conducted as follows:
In order to avoid considerable heterogeneity,15 we only presented forest plots when I2 heterogeneity was <75%. In the exercise-only interventions, we conducted meta-analyses for:
FFAs, GGT, BMI, insulin and total cholesterol.
Sensitivity analysis
Heterogeneity
Heterogeneity was quantified using the I2 test,16 as it does not inherently depend on the number of studies considered. The I2 statistic and corresponding 95% CI were presented, to gauge the degree of heterogeneity present in sample.16 ,17 I2 values range from 0% (homogeneity) to 100% (greater heterogeneity); a CI that does not include 0% indicates that the hypothesis of homogeneity is rejected, and an inference of heterogeneity is merited.16
Meta-analysis and forest plots are presented only for those studies in which the heterogeneity (as measured by I2) was <75%. Heterogeneity beyond this level was deemed too heterogeneous15 to be sensibly pooled, and while interest was in trying to identify factors responsible for the heterogeneity, none of the subsets contained the recommended minimum number of studies (10) to allow this.
Publication bias
Egger bias tests (when at least 10 studies were included) and funnel plots18 were provided to assess the risk of publication bias (see online supplementary files).
Risk of bias assessment
Study quality was assessed by using the TESTEX scale19—the Tool for the assEssment of Study qualiTy and reporting in EXercise—a study quality and reporting assessment tool, designed specifically for use in exercise training studies. The main point of difference in TESTEX is that there are accommodations for: activity monitoring in control groups to measure crossover to exercise by sedentary control patients; assessment of the existence and method of activity monitoring in exercise intervention and sedentary controls; assessment of whether the relative exercise intensity remained constant and therefore potentially avoided de-training as participants initially adapt to new exercise programmes; assessment of whether periodic evidence-based adjustment of exercise intensity is reported exercise volume and exercise expenditure. Information on all exercise characteristics (intensity, duration, frequency and mode) is provided to calculate exercise volume and exercise energy expenditure.
This tool is a 15-point scale (5 points for study quality and 10 points for reporting) and addresses previously unmentioned quality assessment criteria specific to exercise training studies. Two reviewers (NAS and GD) conducted the risk of bias assessment; JRM was consulted if discrepancies occurred.
Results
Studies included in the review
Our initial search identified 53 manuscripts, hand searching of reference lists of included studies and key articles such as related reviews and the latest editions of relevant journals yielded a further 3 manuscripts. Out of 56 studies, 6 were excluded at first inspection as duplicates, 17 were not controlled trials of exercise therapy, 2 were excluded as they had participants <18 years, 2 were excluded as they were not randomised trials, 6 used unmatched interventions or comparator groups and 2 were counselling interventions encouraging exercise participation, leaving 21 included studies for analysis (figure 1).

PRISMA statement.
Description of included studies
Our 21 included randomised controlled trials (25 intervention groups) had an aggregate of 1530 participants, 884 exercise participants and 646 controls. Table 2 summarises included studies.7 ,8 ,20–38 Online supplementary table S1 in the supplementary files summarises the excluded controlled trials.39–50
Included studies—exercise programming details
Thirteen studies used only an exercise intervention and eight studies used both exercise and dietary interventions. Five studies used resistance exercise and 15 used aerobic exercise, and 4 studies also used combined aerobic and resistance exercise. Study duration ranged from 4 to 52 weeks, and training frequency ranged from 2 to 5 times weekly with 20–60 min session duration. Aerobic training intensity ranged from 45% to 85% of peak VO2. Control groups were classified as sedentary, although some used a stretching routine.
Measurement of study outcomes
Of note is that only one of the included studies38 used the gold standard liver biopsy method to assess liver function. Instead of direct assessment of liver function, several studies used plasma concentrations of liver enzyme as surrogate markers of liver function. Moreover, a number of different techniques were used to quantify liver enzymes.
Study quality assessment
Median TESTEX score was assessed as 10 out of 15 by two reviewers (NAS and GD); three studies each scored 7, 8 or 11. Four studies scored 9, five studies scored 10, one study scored 12 and two studies scored 13 (figure 2). Of the TESTEX items, the following were done particularly poorly in general: allocation concealment only 5/21 studies; blinding of assessors 5/21; physical activity monitoring in the control groups to check with sedentary controls crossed over to exercise 10/21; assessment of energy expended during exercise 10/21.

Study quality assessment. Key: total out of 15 points. Legend: #three points possible—one point if adherence >85%, one point if adverse events reported, one point if exercise attendance is reported. *Two points possible—one point if primary outcome is reported, one point if all other outcomes reported. TESTEX, Tool for the assEssment of Study qualiTy and reporting in Exercise.
Summary of change in outcome measures
Only two included studies compared aerobic versus resistance training, as such this training group is not considered further.
Change in intrahepatic fat
Data on IHF were available from nine studies (12 intervention groups) of exercise, with or without dietary intervention. Six study groups showed significant IHF reductions; one study showed a significant increase and five studies showed no change.
Exercise-only studies had high heterogeneity (I2 84.4%, 95% CI 70.1% to 91.4%) and there were too few studies (6) to allow for investigation of the cause of the heterogeneity beyond the following subgroup analysis.
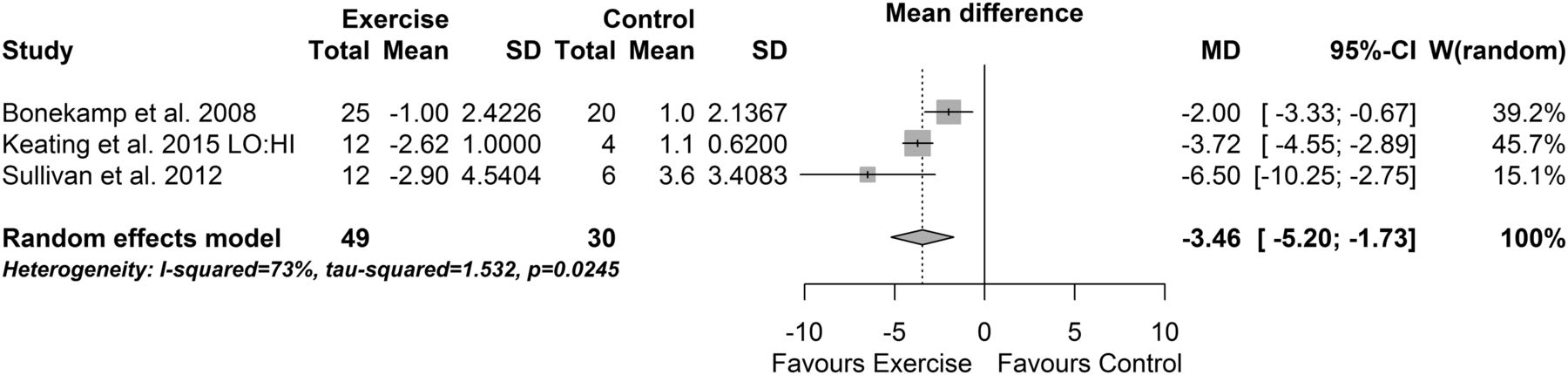
When data from the exercise-only versus control programmes that expended an aggregate of >10 000 kcal were pooled, there was a reduction in IHF (−3.46% (95% CI −5.20% to −1.73%), p<0.0001, I2=73% (95% CI 9% to 92%), figure 3). The effect size was large (SMD −1.77 (−3.11 to −0.42), p=0.01, I2=77%).

Percentage change in intrahepatic fat: exercise programmes >10 000 kcal energy expenditure.
Diet plus exercise studies had no evidence of heterogeneity (I2 0%, 95% CI 0% to 84.2%) and indicated no evidence of a change in IHF between diet and exercise versus diet alone studies (MD 0.87% (95% CI −0.07% to 1.81%), p=0.07 (from a multivariate model)). Effect size (SMD) was small to moderate (0.29, 95% CI (−0.19 to 0.78), p=0.24).
Change in body mass and BMI
Fourteen exercise studies with or without dietary intervention (17 intervention groups) reported change in body mass. Nine groups reported a significant fall in body mass, one group reported a significant rise and seven groups were equivocal.
The exercise-only body mass studies (n=7) exhibited substantial heterogeneity (I2 95.1%, 95% CI 92.6% to 96.8%) even in the multivariate analysis. The small number of studies precluded investigation of the heterogeneity. The diet and exercise studies showed less heterogeneity (I2 71.3%, 95% CI 40.8% to 86.1%) but no evidence of a change in body mass in the multivariate meta-analysis model (MD −2.94 kg, 95% CI (−5.93 to 0.04)); effect size (SMD) was moderate (−0.34, 95% CI (−0.55 to −0.13), p=0.001).
Eleven exercise study groups, with (n=5) or without (n=6) dietary intervention, reported change in BMI, with only four groups reporting a significant improvement, while the other seven groups showed no change.
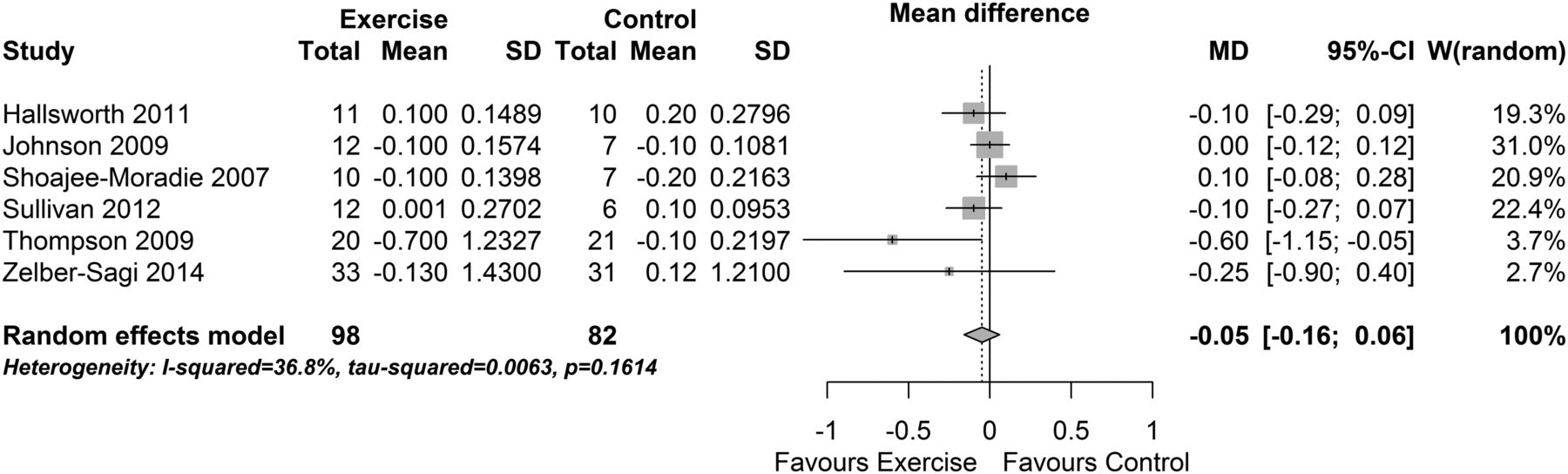
Meta-analysis of the five diet and exercise BMI studies indicated substantial heterogeneity (I2 83% (95% CI 62% to 93%). The small number of studies precluded investigation of the heterogeneity. Meta-analysis of the effect of exercise-only intervention studies on BMI found a no evidence of a change (MD −0.05 kg/m2 (95% CI −0.16 to 0.06), p=0.38, I2=37% (95% CI 0% to 75%), see figure 4). The effect size was small to moderate (SMD −0.26 (−0.56 to 0.04), p=0.09, I2=0%) and also indicated no change in BMI.

Change in body mass index: exercise interventions.
Fasting FFAs
When data from all nine exercise studies with or without dietary intervention (11 intervention groups) were examined, only 5 groups reporting a significant improvement, while the other 6 groups showed no change.
When data from only exercise studies were pooled using a multivariate meta-analysis model, there was a reduction in fasting FFA (−74.15 µmol/L (95% CI −118.47 to −29.84), p=0.001, I2=67% (95% CI 32% to 85%), figure 5). The effect size (SMD) indicated a large change in FFA (−0.94 (−1.36 to −0.52), p<0.0001, I2=0%). The three pooled diet and exercise studies exhibited substantial heterogeneity (I2 88%, 95% CI (65% to 96%)) and were not considered further.
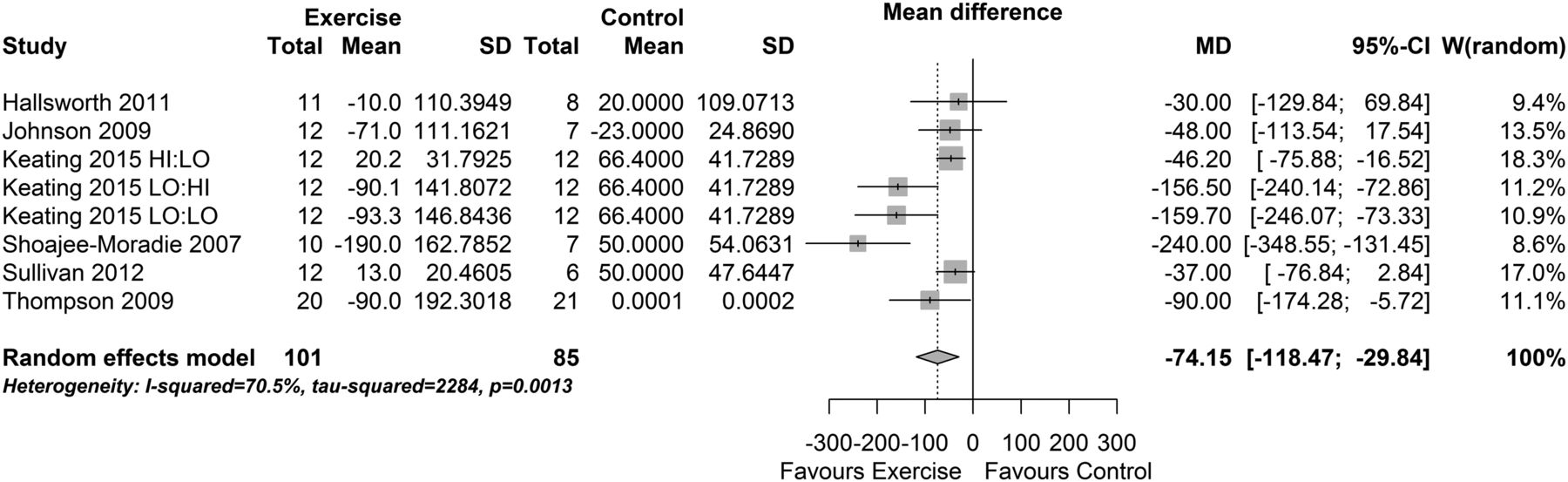
Change in fasting free fatty acids: exercise interventions.
Liver enzymes
Alanine aminotransferase
Examination of data from 16 exercise studies with or without dietary intervention (20 intervention groups) revealed that ALT was not significantly altered in 10 groups and was significantly reduced (improved) in 5 groups and increased in 5 groups.
The nine pooled exercise-only studies exhibited substantial heterogeneity (I2 91%, 95% CI 87% to 94%) and were not considered further. The seven pooled diet and exercise studies exhibited high levels of heterogeneity (I2 73%, 95% CI 45% to 87%) with no evidence of a difference in effect between diet and exercise and diet control groups (MD 0.96 IU/L (95% CI −2.84 to 4.76)). Effect size (SMD) was negligible (0.01, 95% CI (−0.40 to 0.42), p=0.95).
Aspartate aminotransferase
When data from nine exercise studies with or without dietary intervention (12 intervention groups) were examined, there was no change in AST in 6 groups, while 3 groups showed a significant reduction and 3 groups showed a significant increase.
The four pooled exercise-only studies exhibited substantial heterogeneity (I2 88%, 95% CI 77% to 94%) and were not considered further. The five pooled diet and exercise studies exhibited high levels of heterogeneity (I2 61%, 95% CI 5% to 84%) with no evidence of a difference in effect between diet and exercise and diet control groups (MD −0.68 IU/L (95% CI −2.54 to 1.18)). Effect size (SMD) was small (−0.20, 95% CI (−0.73 to 0.34), p=0.47).
γ-Glutamyl transpeptidase
Data from six exercise studies with or without dietary intervention (seven intervention groups) showed there was no significant change in GGT in six groups; only one group showed a significant reduction. Only two diet and exercise studies were included; thus, pooling was not performed for that group.
When data from the four exercise-only studies were pooled using a multivariate meta-analysis model, there was no significant reduction in GGT (MD −3.52 IU/L (95% CI −8.37 to 1.34), p=0.16, I2=71% (95% CI 26% to 89%), see figure 6). The effect size (SMD) was moderate, but the interval suggested no significant effect (−0.30 (−0.69 to 0.09), p=0.13, I2=74%).

Change in γ-glutamyl transpeptidase: exercise interventions.
Peak VO2
Data from eight exercise studies with or without dietary intervention (11 intervention groups) were examined; there was a significant improvement in cardiorespiratory fitness in six groups but not in five groups.
The five pooled exercise-only studies exhibited substantial heterogeneity (I2 86%, 95% CI 75% to 92%) and were not considered further. The three pooled diet and exercise studies exhibited high levels of heterogeneity (I2 68%, 95% CI 8% to 89%) with no evidence of a difference in effect between diet and exercise and diet control groups (MD −0.05 mL O2/kg/min (95% CI −0.22 to 0.12)). Effect size (SMD) was small (0.1430, 95% CI (−0.5377 to 0.8236), p=0.68).
Insulin
Data from 11 exercise studies (12 intervention groups) with or without dietary intervention was analysed; there was a significant insulin reduction in 5 groups but no change in 6 groups, and 1 group showed an increase in insulin.
When data from the four exercise-only studies were pooled, there was a significant reduction in insulin (MD −1.88 IU/L (95% CI −3.43 to −0.34), p=0.02, I2=31% (95% CI 0% to 75%), figure 7). The effect size was moderate but was not significant (SMD −0.47 (−1.07 to 0.13), p=0.13, I2=63%). Pooling the seven diet and exercise studies resulted in substantial heterogeneity (I2 78% (95% CI 57% to 89%)); hence, these results are not considered further.

Change in insulin: exercise interventions.
Total cholesterol
Data from 12 exercise studies (12 intervention groups) with or without dietary intervention were considered; there was a significant total cholesterol reduction in 6 groups but no change in 7 groups.
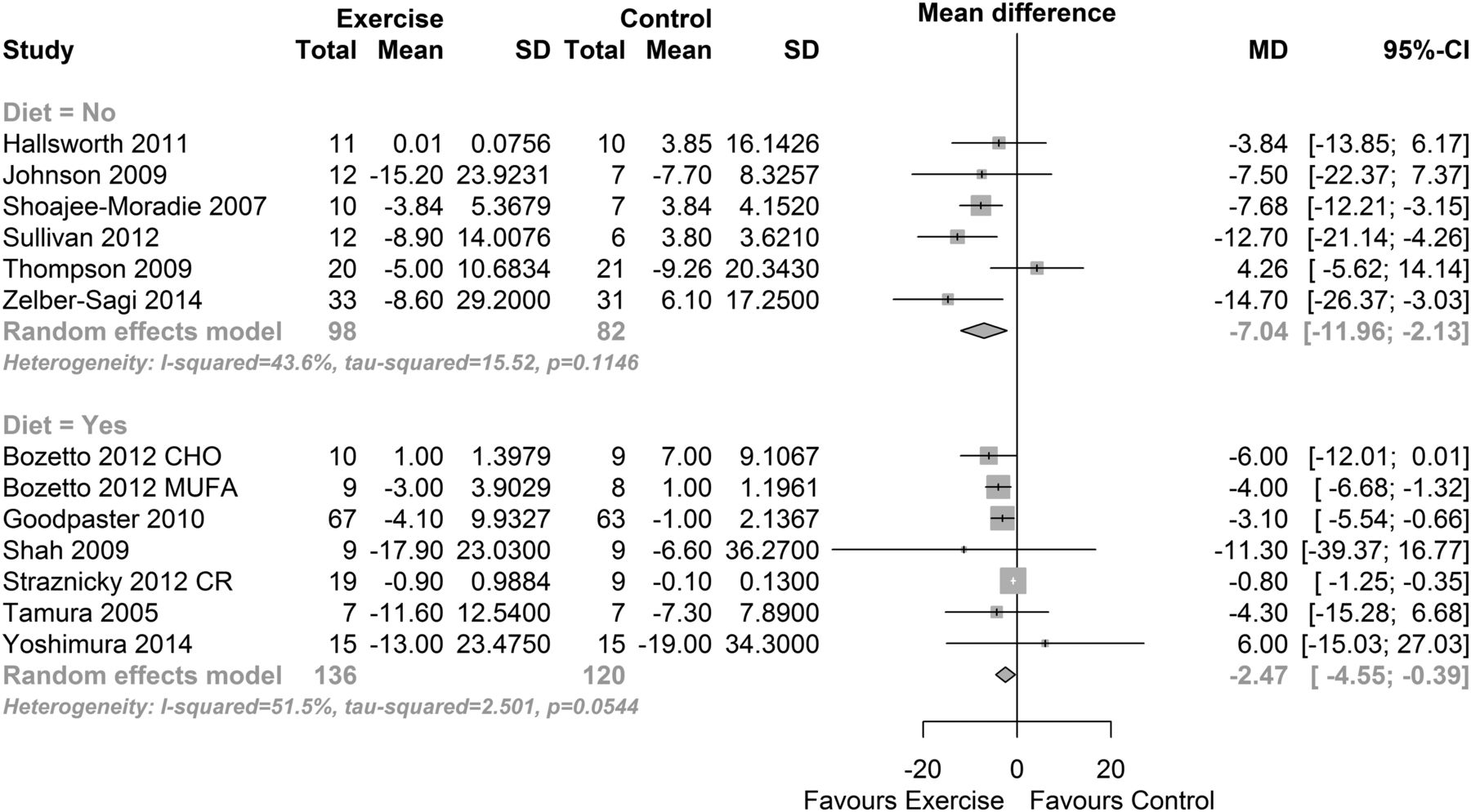
When data from the six exercise-only studies were pooled, there was a significant reduction in total cholesterol (MD −7.04 mg/dL (−11.96 to −2.13), p=0.005, I2=44% (95% CI 0% to 78%), figure 8 (top)). The effect size was moderate (SMD −0.49 (−0.95 to −0.03), p=0.035, I2=50%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in total cholesterol: exercise interventions.
When data from the six diet and exercise studies were pooled using a multivariate meta-analysis model, there was a significant reduction in total cholesterol (MD −2.47 mg/dL (−4.55 to −0.39), p=0.020, I2=44% (95% CI 0% to 78%), figure 8 (bottom)). The effect size was moderate (SMD −0.49 (−0.85 to −0.13), p=0.008, I2=52%).
Risk of bias assessment
The similarity in sample and effect sizes between randomised, controlled trials used in the analysis and those trials that were excluded from analysis suggests selection bias is minimal. The sample sizes are small; however, there is no apparent bias evident in the Egger plots (see online supplementary figures).
Discussion
This work analysed the effects of exercise training, with or without dietary intervention, on intrahepatic fat, body mass, BMI, FFAs, insulin liver enzymes, lipids and cardiorespiratory fitness (peak VO2). Our primary findings show that exercise training, in isolation from dietary intervention, has beneficial effects on some of these aforementioned outcome measures. We were able to establish that intrahepatic fat loss may be optimised by usage of greater total exercise training energy expenditure. It appears that the addition of recently published work has added diversity to the current evidence base and increasingly varied study designs have necessitated a more cautious approach to data pooling and subsequent meta-analysis.
Our work failed to show changes in any of the three primary liver enzymes with exercise training. The number of participants included in these three analyses varied between 797 and 1109, so it is unlikely that these analyses were underpowered. There were, however, several confounding variables in the included studies that may have prevented the isolated effects of exercise to be examined. There were eight studies that, in addition to exercise training, also provided various dietary interventions. Moreover, the exercise training programmes varied greatly between studies with respect to exercise intensity, duration, frequency and modality (eg, aerobic vs resistance training). Whatever the reason for the absence of significant changes, our work confirms the previous findings that liver enzymes have limited sensitivity in detecting early liver disease.9 It appears that liver enzymes are, at best, a blunt tool for assessing change in liver function after exercise training.
Our analysis suggested that intrahepatic fat is reduced with exercise training, in as little as 4 weeks,25 but aerobic exercise programmes of total energy expenditure >10 000 kcal are likely to elicit greater improvements than programmes with lower exercise energy expenditure. Our findings in this respect advance those of Keating et al6 who conducted pooled analyses of all exercise modalities.
In mild FLD, the first choice therapy is lifestyle modification, although medications that decrease insulin resistance, hyperlipidaemia and those that induce weight loss have been shown to improve liver function.51 Our analysis reinforces the fact that even short-term exercise training is effective in reducing intrahepatic fat. These findings suggest that exercise may benefit liver health through a calorie expenditure mechanism, sufficient levels of which are acquired more rapidly with vigorous or high-intensity exercise training. Data from heart failure studies suggest that high-intensity exercise may promote superior health benefits.11
It has been recognised that FFAs are the vehicle by which triacylglycerol is stored in adipose tissue and is transported to its site of usage.52 FFA turnover is rapid with a half-life of 2–4 min.52 In our analysis, three studies using >10 000 kcal total exercise programme energy expenditure appear to elicit greater reductions in intrahepatic fat. High volume exercise energy expenditure provides a variety of benefits related to metabolic disorders; we propose that one clinical benefit directly related to liver function is that high volume aerobic exercise elicits triacylglycerol consummation. Of course other exercise-induced benefits will accrue and primarily affect other organs, besides the liver, such as improved flow-mediated vascular dilation,53 cardiac function,54 peak VO253 ,54 and weight loss which was minimal in our analysis.
Our analyses suggest that it is calorie burning that elicits reductions in liver fat, reduced fat storage, possibly reduced liver enzymes and the sum of all of this is improved glycaemic control. Of perhaps most interest is that the above changes are achieved almost totally independent of body mass changes. To illustrate this, we chose the study of Shoajee-Moradie et al,30 because this work was the only included study to use high-intensity exercise and measure peak VO2, allowing calorie expenditure to be calculated. The exercise participants in Shoajee-Moradie et al's30 study expended 9.8 kcal per minute, or 590 kcal each week, the study only ran for 6 weeks. Exercise participants therefore only expended 3500 kcal during the whole study, equivalent to 0.5 kg of fat. Not surprisingly, Shoajee-Moradie et al30 reported no change in body mass in either exercise or control groups. Nevertheless Johnson et al's25 study reported a similar aggregate exercise programme energy expenditure (3800 kcal) but as it was delivered in a shorter 4-week period, changes in IHF were noted.
Limitations
A major limitation of this work was that considerable heterogeneity meant that data pooling was unjustified in a number of meta-analyses. We systematically attempted to identify reasons for heterogeneity by grouping studies according to similarities in interventions, exercise programmes, patient populations, but we failed to identify definitive conclusions. We were able to reduce heterogeneity somewhat by limiting data pooling to studies that did not use concurrent dietary interventions. Some patients were overweight/obese, while others had definitive liver disease; some of the former may well have also exhibited clinical NAFLD. The likelihood is that the potential for non-clinical NAFLD participants to ‘regress to the mean’ was probably less than in those with diagnosed NAFLD.
As discussed previously, liver enzymes have limited predictive value for liver function, and it is notable that only one of the included studies used the gold standard liver biopsy method to assess liver function. There were studies that, in addition to exercise training, also provided various dietary interventions. The exercise training programmes varied greatly between studies with respect to exercise intensity, duration, frequency and modality (eg, aerobic vs resistance training). The normal distribution of the Egger plots evidenced minimal risk of publication bias.
In the case of the liver enzymes, some heterogeneity may be explained by the naturally occurring interparticipant variation that exists with these enzymes. Measures of lean, and fat, body mass would have shed more light onto the role that body composition plays in improving liver function through exercise. We would like to have conducted subgroup analyses of those with normal and impaired liver function but group level (as opposed to individual patient data) precluded this. We considered programme duration, modality and frequency subanalyses, but the variation in included study data precluded this.
Metaregression between change in liver function and body mass was considered, but change in body mass was not reported in all studies.
The current number of published studies does not allow meta-analyses to compare: aerobic versus resistance exercise, high-intensity versus low-intensity or moderate-intensity exercise, and effects of weekly exercise duration. All of these comparisons may influence change in current guidelines.
The risk of bias assessment identified that allocation concealment to investigators was conducted in less than one-quarter if studies and investigator bias is quite likely. Moreover, assessor blinding was uncommon (only 5 of 21 studies), so this would not mitigate allocation concealment. The lack of physical activity monitoring in 50% of the studies implies that there was likelihood that sedentary controls crossed over to exercise in some studies. The lack of assessment of energy expended during exercise in 10 studies meant that our meta-analyses of aggregate energy expenditure may not be fully representative.
Future studies should aim to at least blind the outcome assessors to the participants' intervention to minimise outcome assessment bias. Future work may also wish to focus on exercise-induced calorie expenditure and the presence or absence of associated weight loss, in order to clarify the mechanism of benefit. Use of gold standard biopsy, rather than reliance on liver enzymes, assessment of liver function is recommended.
Conclusions
Exercise training reduces intrahepatic fat and FFAs while increasing cardiorespiratory fitness. An aggregate exercise programme energy expenditure (>10 000 kcal) may be required to promote reductions in intrahepatic fat.
What are the findings?
Several new published randomised, controlled trials of exercise intervention suggest, for the first time, non-esterified fatty acids are reduced with exercise intervention.
Changes in intrahepatic may be possible, but only in exercise programmes that elicit >10 000 kcal of energy expenditure.
Varied study interventions render it difficult to separate the relative effects of diet and exercise on liver function.
How might it impact on clinical practice in the future?
Imaging, rather than liver enzyme concentrations, should be used to assess liver status.
Preferably 3 months of adherent exercise training, after baseline assessment, should ensue before liver imaging is repeated.
References
Footnotes
Contributors NK is a postdoctoral lecturer who conducted some of the data extraction, study quality assessment and manuscript writing. GD assisted with data searching, extraction, data checking, study quality assessment, and writing and editing of the manuscript. JRM assisted with the literature search, assessment of study quality, and verified the accuracy of the main text and online supplementary files section as well as contributing to writing and editing the main text. PLG verified accuracy of data extraction, conducted analyses especially regarding heterogeneity, provided comprehensive statistical advice for the response to reviewers as well as contributing to the editing of the rebuttal and final revised text and provision of some of the figures. NAS was the team leader, who also assisted with study inclusion/exclusion, data extraction/analysis and writing and editing of the main text and supplementary files.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Supplementary files are available which consists of PubMed search strategy, Funnel plots, table of excluded RCTS.