Article Text

Abstract
Introduction Stem cells have emerged as a new treatment option for tendon disorders. We systematically reviewed the current evidence for stem cell therapy in tendon disorders.
Methods Randomised and non-randomised controlled trials, cohort studies and case series with a minimum of 5 cases were searched in MEDLINE, CENTRAL, EMBASE, CINAHL, PEDro and SPORTDiscus. In addition, we searched grey literature databases and trial registers. Only human studies were included and no time or language restrictions were applied to our search. All references of included trials were checked for possibly eligible trials. Risk of bias assessment was performed using the Cochrane risk of bias tool for controlled trials and the Newcastle-Ottawa scale for case series. Levels of evidence were assigned according to the Oxford levels of evidence.
Results 4 published and three unpublished/pending trials were found with a total of 79 patients. No unpublished data were available. Two trials evaluated bone marrow-derived stem cells in rotator cuff repair surgery and found lower retear rates compared with historical controls or the literature. One trial used allogenic adipose-derived stem cells to treat lateral epicondylar tendinopathy. Improved Mayo Elbow Performance Index, Visual Analogue Pain scale and ultrasound findings after 1-year follow-up compared with baseline were found. Bone marrow-derived stem cell-treated patellar tendinopathy showed improved International Knee Documentation Committee, Knee injury and Osteoarthritis Outcome Score subscales and Tegner scores after 5-year follow-up. One trial reported adverse events and found them to be mild (eg, swelling, effusion). All trials were at high risk of bias and only level 4 evidence was available.
Conclusions No evidence (level 4) was found for the therapeutic use of stem cells for tendon disorders. The use of stem cell therapy for tendon disorders in clinical practice is currently not advised.
- Tendon
- Cellular
- Review
Statistics from Altmetric.com
Introduction
Tendon disorders, in particular tendinopathy, is a frequently seen condition in athletes and in the general population.1–3 It is defined by localised swelling, pain and functional limitations of the affected tendon.4 Several therapies, such as eccentric exercises,5 non-steroidal anti-inflammatory drugs,6 shockwave therapy,7–9 corticosteroids,10 platelet-rich plasma11 ,12 and surgery6 have been used as treatments for tendinopathy, with variable levels of evidence and success. Despite some good results for some of these therapies,5 recalcitrant cases remain.
More recently, stem cells have entered the field of tendon disorder treatment. Several reviews have addressed the current evidence of cell therapy in tendinopathy and found that mostly small or large animal studies were available.13–18 Although in animal studies, there have been positive results in favour of stem cell treatment, clinical trials have been scarce and have shown only ‘encouraging results’.13–18
The current model of chronic tendon disorders is based on a continuum of degeneration and failed healing19–21 with a yet unclear role of inflammatory cells.20 ,22–24 This model is mainly supported by histological findings with necrotic and apoptotic tenocytes, neovascularisation and collagen disarray.19 ,20 Within this model, the proposed mechanism of repair through stem cell use is twofold; first through these cells’ differentiating capabilities into new tenocytes they are proposed to generate new tendon tissue.13 ,18 Second, the paracrine effects of stem cells modulate the local immune response and stimulate repair in the surrounding cells by the production of growth factors and cytokines.12 ,25–28
As more and more clinics arise that use stem cell treatments for a variety of conditions, including orthopaedic soft tissue disorders such as tendon disorders,29 and with the increasing number of trials being published on this topic, we felt it was necessary to review the current evidence. Our aim was therefore to systematically review the efficacy of stem cell therapy for pain and functional outcomes in the treatment of tendon disorders in humans.
Methods
We systematically searched for trials that investigated the effect of stem cell therapy of any kind in tendon disorders. Randomised and non-randomised controlled trials, cohort studies and case series with a minimum of five cases were searched. Complete selection criteria are reported in box 1.
Inclusion and exclusion criteria
Inclusion criteria
Published and non-published human studies, randomised and non-randomised. Case series with ≥5 cases.
Patients with tendon disorders diagnosed based on history and physical examination or imaging.
Stem cells of any origin were used as treatment, minimal proof of stem cell presence was needed (eg, automated cell analysis, surface marker analysis, culturing, etc).
In case of controlled trials, the effect must be compared with another treatment modality, placebo or no intervention.
Had to report at least one of the following outcomes: time to recovery (or play), recurrences, patient-reported outcomes (PROMs), pain scales, adverse events.
Exclusion criteria
Participants with tendinopathies and other concomitant injuries which were not separately assessed.
Search methods
With the help of a research librarian, a sensitive search strategy for multiple databases was developed by one author (MW) (see online supplementary appendix 1).
supplementary appendix
Using this strategy, one author (MW) searched all databases from the databases’ inception up to June 2016. We did not impose any restrictions on our search. We searched the following electronic databases: MEDLINE-PubMed, CENTRAL, EMBASE, CINAHL, PEDro and SPORTDiscus. Furthermore, possible unpublished and ongoing trials were searched in OpenGrey; the British Library Inside; Web of Science and BIOSIS Previews and several international and national trial registers: the ISRCTN registry (http://www.controlled-trials.com), the WHO trial register (apps.who.int/trialsearch), EU clinical trial register (http://www.clinicaltrialsregister.eu); ClinicalTrials.gov and the Dutch trial register (http://www.trialregisters.nl). After inclusion of a trial, all references were hand searched for possible additional studies.
Study selection
After deletion of duplicates, two reviewers (HP and MW) independently scanned titles and abstracts of all identified studies. Full-text reports were obtained for potentially relevant studies. Both reviewers then independently applied the selection criteria (see box 1). In case of disagreement between reviewers, consensus was sought, and in case of persistent disagreement, a third party (MHM) was consulted.
Data extraction
Using a standardised data extraction sheet, two authors (HP and MW) independently extracted the following data: study design, study setting, inclusion/exclusion, details of the intervention (such as origin of stem cells used, cell isolation and culturing, dosage, frequency of administration, etc), primary and secondary outcome measures and adverse effects.
In case of disagreement, consensus was reached in a joint session. If no consensus could be reached, a third reviewer (MHM) was consulted.
Risk of bias assessment
Two reviewers (HP and MW) separately appraised the included studies for their quality. For randomised and non-randomised controlled trials, we used Cochrane Risk of Bias tool.30 We appraised each study for the five major domains of bias: selection bias (random allocation and allocation concealment), performance bias (blinding of personnel and blinding of participants), detection bias (blinding of outcome assessment), attrition bias (follow-up adequacy), reporting bias (complete outcome reporting) and other biases. We adopted previously used criteria, formulated by Winters et al,31 to score each domain (see online supplementary appendix 2). Each item was scored as to be at low (+), high (−) or unclear (?) risk of bias. Studies were considered to be at low risk of bias when all domains were scored as low (+) risk of bias, or one item was at high (−) or unclear risk of bias (?). If two domains were scored as high (−) or unclear (?) risk of bias, the study was considered at moderate risk of bias. Finally, when more than two domains were scored as high (−) or unclear (?) risk of bias, the study was regarded as being at high risk of bias.
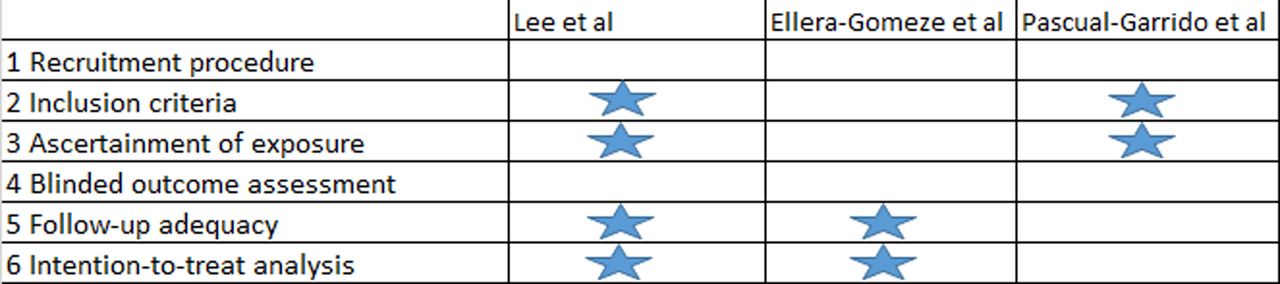
For case series, we used a modified version of the Newcastle-Ottawa quality assessment scale for cohort studies32 (see online supplementary appendix 3). A maximum of six stars could be achieved. No quality subdivision (ie, high, moderate, low risk of bias) was made for case series as these types of study are a priori at high risk of bias and a quality subdivision would not affect its level of evidence.
Data synthesis
We planned a data synthesis for randomised controlled trials (RCTs) (>2), when they were at low risk of bias and were clinically homogenous (ie, identical stem cell type and tendon disorder, cointerventions, mode of injection/transplantation). The mean difference was used for studies that used the same outcome measurement. Standardised mean differences were used for studies that used different outcome measures to estimate treatment effects. A p value <0.05 was considered significant for all analyses. We used a fixed effects model to pool data that were statistically homogenous, or when <5 studies were available for data synthesis. A random effects model was used when statistical heterogeneity was present (heterogeneity was considered present when the X2—test was significant, p<0.1), and when >5 studies were available for data synthesis. We visually inspected the forest plots and the heterogeneity statistic (I2). If heterogeneity was present, and sufficient studies were available (N≥10), we planned a subgroup analysis or meta-regression analysis to explore the sources for heterogeneity.
If data pooling was not possible, we presented our findings by means of a descriptive synthesis using the levels of evidence approach based on the Oxford Centre for Evidence-based Medicine33 (table 1). Systematic reviews were considered level 1 evidence, RCTs at low/moderate risk of bias or observational studies with a dramatic effect were considered level 2 of evidence, non-randomised controlled trials at low risk of bias at level 3 of evidence. Case series were considered as level 4 of evidence impact. Level 5 evidence was considered only when no studies were available and only mechanism-based reasoning was available. Studies were downgraded when they were at high risk of bias with the lowest level for studies being level 4.
Oxford Centre for Evidence-based Medicine 2011 Levels of Evidence for interventions33
We did not prospectively register the protocol for our systematic review. However, the full protocol is available by email, from the corresponding author (HP).
Results
Study selection
A total of 1043 articles were identified during our searches. After removal of duplicates, 684 singular articles were found. After title and abstract selection seven articles34–40 were selected for full-text evaluation (figure 1). Two trials37 ,39 were excluded because we were unable to determine whether stem cells had actually been injected as no analyses were performed to investigate whether stem cells were actually present. One article was excluded40 because it was mostly in vitro and had no data of interest. One article38 because it concomitantly injected platelet-rich plasma and included patients with osteoarthritis. Three articles34–36 met the inclusion criteria. Hand searching revealed no additional articles. One additional article41 was identified by hand searching previously published reviews evaluating stem cell use in tendon disorders.

Selection process.
Four possibly unpublished studies42–45 were identified but after contacting the principal investigators, no data were made available. One unpublished trial42 was found to be published36 and had already been included in the results. Two unpublished trials43 ,45 were finalised at the time of writing the manuscript (June 2016). The final unpublished trial44 was mentioned to be recruiting, but this could not be verified with the author.
Study characteristics
The characteristics of the included studies are summarised in table 2. One matched non-randomised study35 and three case series were included for review.34 ,36 ,41
Study characteristics
A total of 79 patients were treated with two types of stem cells. The mean ages of the patients ranged from 24 to 61 years and the percentage of women ranged between 50% and 64%. Two studies34 ,35 evaluated the use of bone marrow-derived stem cells as an additive treatment for rotator cuff repair. One study36 investigated the use of allogenic adipose-derived stem cells in lateral epicondylar tendinopathy. The last study41 investigated the use of bone marrow-derived stem cells in patellar tendinopathy.
Harvesting methods were homogenous across the bone marrow-derived trials with collection occurring from the anterior iliac crest.34 ,35 ,41 After harvesting, the bone marrow aspirate was concentrated using a variety of techniques and then injected in the patient.34 ,35 ,41 None of these trials performed culturing or cell typing. One trial35 confirmed the presence of stem cells by counting the number of colony-forming fibroblasts in the samples. One trial34 counted the number of CD34 positive and mononuclear cells in its samples using flow cytometry. The last trial41 used uncharacterised nucleated cells obtained from bone marrow aspirations.
The remaining study36 harvested allogenic adipose-derived stem cells from healthy donors’ subcutaneous fat tissue. After aspiration, the lipoaspirate was purified and tested for viral, bacterial or fungal contamination. Culturing of the stromal vascular fraction was performed but the characterisation of stem cells was unclear. Before the cells were released for injection, a viable cell count was performed and purity of the cell line was assessed (80% viable cells and <1% CD45 positive cells as minimal criteria for release). Patients were injected locally using a double system syringe with fibrin clot to ensure local entrapment within a fibrin matrix.
Risk of bias
Three studies34 ,36 ,41 were assessed using the Newcastle-Ottawa scale and one35 using the Cochrane Risk of bias tool. The motivation for the assessors’ judgements can be found in online supplementary appendix 4.
The study by Hernigou et al 35 was found to be at high risk of bias (figure 2). All domains were at high or unclear risk of bias. Owing to this high risk of bias the study was downgraded to level 4 evidence.

Risk of bias assessment using Cochrane risk of bias tool.
The number of stars awarded for case series ranged between two and four (figure 3). No quality subdivision was made. All studies lacked blinded outcome assessment and were unclear about the recruitment procedure.

{kind=link}
{kind=link}
{kind=link}
Risk of bias assessment using Newcastle-Ottawa scale for cohort studies.
Tendon disorder types and outcomes
Lateral epicondylar tendinopathy
One study36 investigated the use of allogenic adipose-derived stem cells in 12 patients with lateral epicondylar tendinopathy. There were statistically significant positive results compared with baseline at all time points (6, 12, 26 and 52 weeks postinjection) for Visual Analogue Scale (VAS) scores (p<0.001), Mayo Elbow Performance Index (MEPI) (p<0.001) and ultrasound evaluation (p<0.001 for longitudinal and transverse axes) (table 3).
Study outcomes
Patellar tendinopathy
One study41 reported the use of bone marrow-derived stem cells in eight cases of patellar tendinopathy. There were statistically significant improvements after an average 5-year (range 3–6) period for Tegner Activity Scale score (2–8, p=0.006), International Knee Documentation Committee (IKDC) (36–69, p=0.047) and for Knee injury and Osteo arthritis Outcome Score (KOOS) subdomains symptoms (44–71, p=0.0086), activities in daily living (63–90, p=0.0086) and sports (24–63, p=0.0078) (table 3). No statistical improvement were observed for Lysholm score (33–53, p=0.1043), KOOS pain (47–63, p=0.2399), KOOS quality of life (50–71, p=0.0825) and SF-12 mental and physical domains (p=0.5589 and p=0.438, respectively). On ultrasound evaluation, trends towards improvement were seen but these were not statistically evaluated.
Rotator cuff repair
Bone marrow-derived stem cells were injected at the tendon–bone junction of arthroscopic rotator cuff repairs in two studies.34 ,35 Combined, these two studies34 ,35 evaluated the results of 59 patients with stem cell injections. Both studies reported a reduced number of reruptures over time (table 3) compared either with historically selected controls35 (6 vs 25 in favour of stem cell injection, p<0.005) or compared with the literature.34 One study34 reported improvement of mean University of California at Los Angeles shoulder rating scale scores (12 SD 3.0 preoperative vs 31 SD 3.2, 12 months postoperative), but no statistical analysis was performed. The latter study35 did not report any functional or other outcomes besides reruptures. Stem cell-treated patients with and without reruptures were compared and a dose–response analysis found significantly less bone marrow mononuclear cells per cubic centimetre (1500+1200 vs 4200+1900, p<0.01) and less progenitor cells (14 000+9000 vs 54 000+23 000, p<0.01) in the grafts of patients with a rerupture.
Adverse events
Adverse events were reported in one trial.36 No serious adverse events were reported. Mild swelling was seen in 50% of the participants within 48 hours postinjection which spontaneously subsided within 2 weeks. Two participants had ultrasonic evidence of joint effusion after 2 weeks. One case of delayed joint pain (7 weeks postinjection) was reported, which subsided with rest and analgesics. No immunologic reactions were found based on CD4+ and CD8+ T cell ratio.
Summary
Four trials at high risk of bias (level 4 of evidence) were identified during this review. One case series36 evaluated adipose-derived stem cells in lateral epicondylar tendinopathy and found improvements in VAS, MEPI and ultrasound evaluations, when compared with baseline. One case series41 was available evaluating bone marrow-derived stem cells in patellar tendinopathy. It found improved Tegner, IKDC and KOOS subdomains compared with baseline but failed to find improvements in Lysholm, SF-12 and other KOOS subdomains. One case series34 and one non-RCT35 were found evaluating bone marrow-derived stem cells in rotator cuff repair surgery. Historical controls were used in one trial35 and reported a reduced retear rate. The other trial34 reported lower retear rates compared with the literature and improved UCLA scores compared with baseline. One trial36 reported adverse events. None of these adverse events were of grave nature.
Discussion
We performed a systematic review to evaluate the body of evidence for the use of stem cells in tendon disorders. A total of four trials were found,34–36 ,41 only one35 of which used a control group. Three unpublished trials43–45 were identified, two43 ,45 of which have been finalised. The use of stem cells was tested in patellar tendinopathy, lateral epicondylar tendinopathy and rotator cuff tears. Bone marrow-derived and allogenic adipose-derived stem cells were used. All trials were rated as level 4 evidence, making only level 4 evidence available for the efficacy of stem cell use in tendon disorders.
In lateral epicondylar tendinopathy, patellar tendinopathy and rotator cuff repairs improved healing evaluated through imaging modalities such as MRI or ultrasound, functional outcomes and pain scores were found compared with baseline. Reruptures of repaired rotator cuffs treated with stem cell injections per-operatively, were reduced when compared with the literature or historically selected controls. Safety was poorly reported as only one trial36 reported adverse events but found them to be generally of mild nature such as transient pain, swelling or effusion.
Risk of bias in the identified trials
All trials were at high risk of bias and had major methodological limitations. First, only one trial included a control group35 though it should be noted that this was a historically controlled study, consequently, no randomisation could be performed. Neither patients, personnel or outcome assessors were blinded to group allocation. This allowed for a high risk of selection, performance and detection bias. All other trials34 ,36 ,41 lacked a control group, allowing for alternative explanations of their positive results (eg, natural course, confounding, placebo). Lateral epicondylar tendinopathy, for example, is a benign condition, usually resolving within 12–18 months.9 ,46 It is possible that the ultrasound findings in the trial by Lee et al 36 are a result of natural healing. Ellera Gomez et al 34 compared the low retear rates with the literature, however, rerupture rates vary greatly between studies.47 ,48 Given the small number of patients in this study, and a 0% rerupture rate within 12 months, this may still lie within the normal distribution of probability.
The placebo effect might account for the positive results of Pascual-Garrido et al.41 The inclusion of non-adult participants (ie, <18 years) in this trial41 may also limit the generalisability of the study’s findings to the adult population. We question the ethical soundness of highly experimental stem cell therapy in minors. Also, a high risk of selection and attrition bias seems to be present in this study; only patients who were able to complete the 2-year follow-up were included in the report.
Overall, due to high risk of bias across studies, all trials were assessed as level 4 evidence. Therefore, these results should be interpreted with great caution.
Stem cells have been used in medicine in attempts to treat a variety of conditions.49–54 Their use in tendinopathy is relatively new and this review critically examined the body of evidence in humans. It is now clear that the evidence to date is very poor with only highly biased trials reporting on the efficacy of stem cell treatment. Previous reviews14–16 which included veterinary studies, have reported more trends towards efficacy but, as is the case with this review, all concluded that there is almost no evidence for stem cell therapy in the treatment of tendon disorders in humans. Three ongoing trials43–45 were found and we hope to review their results once they are published. Despite the fact that these trials may influence our results, we felt it was necessary to publish this result now considering the growing interest in this subject and the growing number of stem cell clinics.29
Theoretical rationale for the use of stem cells to treat tendon disorders
Mesenchymal stem cells (MSCs) are defined as self-renewing and multipotent cells capable of differentiating into multiple cell types, including osteocytes, chondrocytes, adipocytes, hepatocytes, myocytes and cardiomyocytes.55 MSCs were originally isolated from the bone marrow stroma but have also been identified also in other tissues, such as fat, epidermis and umbilical cord blood.56 ,57 The International Society for Cellular Therapy released a position statement in 200658 outlining the minimal criteria for defining MSCs: adherence to plastic, the presence of CD73, CD90 and CD105 antigen markers, absence of CD11b, CD14, CD19, CD34, CD45, CD79α and HLA class II and the ability to differentiate in vitro.
The mechanisms by which stem cells are proposed to repair injured tendons can be considered twofold. First, stem cells are proposed to differentiate into tenocytes and restart the healing process by differentiating into tenocytes.18 ,59 ,60 However, the fate of stem cells after injection is not well studied in tendon injury and research suggests that few cells remain in situ after implantation.14–16 ,25 ,61 Therefore, it is questionable whether there are enough cells to be of value for tendon repair. Second, the paracrine effect of stem cells is hypothesised to be beneficial for tissue repair.14 ,62 ,63 Several reviews25 ,63–67 have summarised the number of growth factors and cytokines that are secreted by MSCs and how these factors influence, often in animal models, the repair mechanisms of injured tendons. It should be noted that other injection therapies with growth factors, such as platelet-rich plasma, have mostly failed to demonstrate their efficacy within tendon disorder treatment.11 ,12 ,68
Safety and quality of stem cell preparations
The MSCs used in the reviewed trials have not been found to be associated with malignancy.69 ,70 However, safety concerns remain an important issue for clinicians.62 Of the included trials, only one36 reported adverse events, finding only mild adverse events within a 1-year follow-up. The remaining trials34 ,35 ,41 failed to report adverse events allowing for potentially dangerous side effects to have gone unnoticed.
Although all trials34–36 ,41 documented the mean number of injected stem cells, the ways of analysing the numbers and cell types varied across the studies. As mentioned earlier, specific criteria are available.58 Of the included studies, only one trial36 partially fulfilled these criteria. Ellera Gomes et al 34 used CD34 and mononuclear cell analysis, which is more specific for haematopoietic progenitor cells rather than bone marrow MSCs.55 ,58 The use of colony-forming unit counting by Hernigou et al 35 is a method that seems incomplete without surface marker analysis.71 Considering the above, the methods used by Pascual-Garrido et al 41 also seem inadequate to properly confirm adequate stem cell numbers.
In three studies,34 ,35 ,41 stem cells concentrates were used and culturing was never performed. The mean number of injected cells varied widely with up to a factor of 1000 in difference generally favouring culturing. Two studies35 ,36 analysed whether dosage played a role in the healing process. Lee et al 36 found no differences between 106 or 107 cells, Hernigou et al 35 found significantly lower number of stem cells and progenitor cells in patients with graft failures. The other two studies34 ,41 did not perform dosage analyses.
One concern with uncultured stem cell concentrates as used in the identified trials34 ,35 ,41 is the presence of multiple cell types.62 As to date there is no consensus62 ,72 regarding whether this non-cultured concentrating method is equally effective as the use of cultured stem cell implantation or injection, we cannot judge whether this is an important factor influencing the outcomes. Furthermore, we could not evaluate whether cell dose may play a role in possible therapeutic efficacy due to the heterogeneity in cell numbers, types of tendon disorders and the low number of participants.
Limitations
We excluded two trials37 ,39 that used bone marrow aspirates, and we discovered two other trials73 ,74 that made attempts to investigate stem cell efficacy in tendon disorders. All these trials were excluded because no analysis was performed to confirm the presence of potential stem cells in the intervention. We therefore believe their exclusion is justified, as inclusion would have created even more heterogeneity in this review. Furthermore, publication bias could not be investigated due to the small number of trials. This might mean that overly positive results are presented in our review. However, we aimed to control for publication bias as much as possible. We searched several grey literature databases and multiple trial registers to find all relevant existing studies investigating stem cell therapy in tendon disorders. Even though no protocol for this review was registered, we wrote and followed an a priori protocol which is freely available through the corresponding author (HP). Despite these limitations, we believe that this review provides the clinician with a good overview of the current evidence for using stem cells to treat of tendon disorders.
Future directions
As illustrated by this review, we are currently still a long way from being able to endorse, based on high-quality evidence, the addition of stem cells to the arsenal of possible treatments for tendon disorders. Many gaps in our knowledge about the efficacy, safety, administration route, timing of administration, dosage and consideration of mechanical stimulation13 ,60 ,75 are evident when reviewing the available literature. Future research has many questions to answer but more importantly, we believe that sound scientific investigations should be performed. As we illustrated with our risk of bias assessment, the current evidence is tainted with methodological flaws that allow for high risks of biased results. In the future, stem cell therapies should be tested RCTs, with appropriate characterisation of the cells, proper randomisation procedures and allocation concealment. Considering the results of currently available treatments like eccentric exercises,5 ,6 we believe it to be important to compare the possible efficacy of stem cell treatments with these currently accepted treatment modalities. Furthermore, studies should incorporate blinding of participants, personnel and outcome assessors. Adverse events should be recorded and reported in all cases. Finally, sample sizes should be large enough to find clinically relevant differences.
The above discussed shortcomings and concerns are in congruence with the findings of the recently published position statement of the Australasian College of Sports Physicians.62 On the efficacy of stem cell treatment for tendinopathy they stated that there is a lack of evidence, which is a statement we believe to still hold true despite the availability of human trials. Furthermore, the concerns about long-term safety and poor research is one we share alike.
Conclusion
There is no evidence to support the use of stem cell therapy in tendon disorders. Overall, only level 4 evidence was found for the effectiveness of stem cells, and this is insufficient to recommend the use of stem cells of any kind in the treatment of any kind of tendon disorder. All studies are at high risk of bias and results must be replicated through good practice research before more general clinical implementation can be recommended.
What are the findings?
The current level of evidence for stem cell use in tendon disorders is extremely poor.
Only case reports or poorly designed trials are available.
The results from the identified trials are at high risk of bias.
How might it impact on clinical practice in the future?
The use of stem cell therapy for tendon disorders in clinical practice is not suitable outside of an appropriate ethics approved clinical trial.
Patients seeking stem cell treatment for their tendon disorders can now be made aware of the lack of evidence and potential dangers.
In cases where stem cells are used, safety must be monitored and reported by the investigator.
Acknowledgments
The authors would like to thank Roos Steenhuis, research librarian, Onze Lieve Vrouwe Gasthuis West, Amsterdam, for her work in formulating their search.
References
Footnotes
Funding The Dutch National Olympic Committee.
Disclaimer The Dutch National Olympic Committee had no influence in the performance or publication of this review.
Competing interests HP and MW received a grant from the Dutch National Olympic Committee for the realisation of this review. HP reports receiving grants from the Dutch National Olympic Committee and the Sports Physician group, Department of Sports Medicine, OLVG West, Amsterdam, outside the submitted work.
Provenance and peer review Not commissioned; externally peer reviewed.