Article Text

Abstract
Objective (1) Identify differences in hip and pelvic biomechanics in patients with femoroacetabular impingement syndrome (FAIS) compared with controls during everyday activities (eg, walking, squatting); and (2) evaluate the effects of interventions on hip and pelvic biomechanics during everyday activities.
Design Systematic review.
Data sources Medline, CINAHL, EMBASE, Scopus and SPORTDiscus until February 2017.
Methods Primary aim: studies that investigated hip or pelvic kinematics and/or joint torques of everyday activities in patients with FAIS compared with the asymptomatic contralateral limb or a control group. Secondary aim: studies that evaluated effects of conservative or surgical interventions on patients with FAIS using pre-post or controlled clinical trial designs. Biomechanical data must have been collected using three-dimensional motion capture devices. Reporting quality was assessed using the Epidemiological Appraisal Instrument and data were pooled (standardised mean difference (SMD), 95% CI) where populations and primary outcomes were similar.
Results Fourteen studies were included (11 cross-sectional and three pre/post intervention), varying between low and moderate reporting quality. Patients with FAIS walked with a lower: peak hip extension angle (SMD −0.40, 95% CI −0.71 to −0.09), peak internal rotation angle (−0.67, 95% CI −1.19 to −0.16) and external rotation joint torque (−0.71, 95% CI −1.07 to −0.35), and squatted to a lesser depth with no difference in hip flexion range. Pre/post intervention data were limited in number and quality, and to surgical cohorts.
Conclusion This review suggests that patients with FAIS may demonstrate hip biomechanical impairments during walking and squatting, with minimal literature available to comment on other tasks.
Clinical relevance The information presented in the review provides insight into the biomechanical differences associated with FAIS; however, the between-group differences were small to moderate. This information may aid in the development of management strategies for people with the condition.
PROSPEROregistration number CRD42016038677.
- hip
- gait analysis
- walking
- biomechanics
Statistics from Altmetric.com
Introduction
Femoroacetabular impingement syndrome (FAIS) is a motion-related condition with a complex presentation of morphology, symptoms and clinical signs.1 It is associated with the development of labral tears2 3 and an increased risk of hip osteoarthritis (OA).4 Recent recommendations from the Warwick agreement concluded that FAIS has a complex presentation and can only be diagnosed with the presence of assessment findings, symptoms in positions of impingement (flexion and internal rotation) and variances in bony hip morphology.1 Pincer morphology is characterised by overcoverage of the acetabulum, whereas cam morphology is characterised by an increase in bone formation at the femoral head-neck junction.5 The presence of morphological changes without clinical signs and symptoms is not considered to be FAIS,1 and does not dictate that the individual will develop FAIS.6 Cam morphology has been reported in up to 60%–90% of athletic populations.7–10 However, the factors that delineate those who develop symptoms and those who do not are unclear. Since FAIS is a movement-related condition, biomechanical impairments associated with FAIS may play a role in symptom development and persistence, as well as structural joint deterioration.
Biomechanical impairments have been described in patients with FAIS but few syntheses have been performed. A recent systematic review concluded that patients with FAIS had lower range of motion (ROM) into positions of impingement.11 However, the review was based on few available studies and meta-analyses were not conducted to pool study findings. Since the completion of the search strategy in 2013, additional studies investigating the biomechanics during everyday activities in patients with FAIS have been reported.
The best treatment options for those with FAIS are unknown. Arthroscopic surgery is increasingly popular, and intends to treat patients with FAIS by restoring the femoral head-neck offset12 to regain function and relieve symptoms. However, the rates of arthroscopy are increasing despite the lack of supporting evidence.13 The effects of surgical or conservative interventions on biomechanical impairments are not clear. Therefore, the aims of this systematic review were to: (1) identify differences in hip and pelvic biomechanics in patients with FAIS compared with controls during everyday activities (eg, walking and squatting); and (2) evaluate the effects of interventions on hip and pelvic biomechanics during these activities.
Methods
The systematic review protocol was developed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement14 and was registered on the PROSPERO register (http://www.crd.york.ac.uk/PROSPERO/) (2016:CRD42016038677).
Search strategy
A comprehensive search was conducted in Medline, CINAHL, EMBASE, Scopus and SPORTDiscus from the earliest date until February 2017. The search strategy was developed around two concepts with MeSH and keywords (limited to title and abstract) adapted to individual databases (Population: FAIS; keyword examples: ‘femoroacetabular impingement’, ‘cam impingement’, ‘pincer impingement’. Outcome: biomechanics; keywords: ‘kinetics’, ‘kinematics’, ‘biomechanics’) (online supplementary A). Articles were imported into Endnote V.X7 and duplicates removed. Two reviewers (MGK and PRL) independently reviewed the title and abstracts of the Endnote library, and disagreements were resolved by consensus, or a third reviewer (AIS). After title and abstract screening, full-text articles of potentially suitable studies were obtained to determine their eligibility. Reference checking, citation tracking in Scopus and manual searching of ahead-of-print listing in journals of included papers were conducted to ensure all relevant studies were included.
Supplementary file 1
Selection criteria
For the primary aim, studies were eligible if they included participants with FAIS and compared data with healthy controls, or the contralateral asymptomatic limb. For the secondary aim, studies were included if they evaluated the effect of a conservative or surgical intervention on patients with FAIS. This included single group pre-post designs where baseline scores were available for comparison with post-intervention scores. It also included cross-sectional studies where post-intervention scores of one group were compared with outcomes of a group who did not undergo any specific intervention. Included studies must have collected kinematic or joint torque data during activities using three-dimensional motion capture devices. Kinematic data must have been reported as means, peaks or total ROM and joint torque data must have been reported as means, peaks or impulses. Where duplicates of published data existed, the study with the larger sample size was included. Opinion pieces, editorials, narrative reviews, systematic reviews, case studies, book chapters, conference abstracts and studies published in a language other than English were excluded.
Reporting quality
Included studies’ reporting quality was rated using a modified version of the Epidemiological Appraisal Instrument (EAI).15 The EAI is appropriate to assess the reporting quality of observational15 16 and intervention studies.15 Items that were not relevant to observational and pre/post intervention studies were removed. Items were scored as ‘Yes’ (2 points), ‘Partial’ (1 point), ‘No’ (0 point), ‘Unable to Determine’ (0 point) or ‘Not Applicable’. The maximal obtainable score for an observational study was 54, and 66 for a pre/post intervention study. Included studies were given a rating of high, moderate or low reporting quality based on the following criteria: high, >70% score on the EAI; moderate, ≤70% and >50%; and low, ≤50%. Two reviewers (MGK and PRL) independently reviewed the studies against the items and where consensus could not be made, a third reviewer (AIS) independently reviewed the paper.
Data extraction
Information on study design, sample characteristics (eg, age, sex, inclusion criteria), hip and pelvic kinematics, and joint torques were extracted and entered into Excel by one reviewer (MGK) with a random selection of 50% of the extracted data checked by another reviewer (PRL). All kinematic and joint torque data were extracted during stance phase where possible and data that were reported in text as graphs were digitised and extracted using DigitizeIt (DigitizeIt, Braunschweig, Germany). For pre/post intervention studies that included data on asymptomatic controls, the pre-intervention and control data were extracted to address the primary outcome, whereas the pre/post intervention data were extracted for the secondary outcome. Where included studies reported subsets of data from a smaller sample of additionally published work, the data from the larger sample were taken. However, if the larger sample had incomplete data, the study with the smaller, but complete data set was used for meta-analysis. If necessary, authors were contacted for further information to confirm eligibility and facilitate accurate data extraction.
Data analysis
Extracted data on hip and pelvic kinematics, and joint torques were grouped according to planes of motion for all included studies. Torque data that were reported as internal moments were multiplied by −1 and reported as external moments for summary and analysis. Standardised mean differences (SMD) and 95% CIs were calculated for all variables analysed in the FAIS versus control population by dividing the difference between groups by the pooled SD. Where multiple studies were available, data were pooled in a meta-analysis using a random effects model (Review Manager V.5.3). To maintain sufficient clinical homogeneity for data pooling, studies were grouped according to population (eg, cam-only FAIS) and outcome (eg, peak hip extension). Cohen’s criteria were used to interpret pooled SMD with a large effect defined as ≥0.8, moderate >0.5 and <0.8, and a small effect defined as ≤0.5 and ≥0.20.17 Statistical heterogeneity was evaluated from pooled data using the I2 statistic, where a value of 25%, 50% or 75% was considered low, moderate or high level heterogeneity, respectively.18 In the event that data were unable to be pooled in a meta-analysis, a qualitative synthesis was conducted by reporting the SMD and 95% CI, along with the reporting quality. Where data were estimated from graphs of included studies, sensitivity analyses were conducted with the estimated data removed.
Subgroup analyses were conducted on data reported for patients with cam-only FAIS. Specifically, subgroups were defined as cam-only FAIS when the study’s eligibility criteria included symptomatic patients with cam morphology and excluded those with combined (defined as an individual with both cam and pincer morphology in the same hip) or pincer-only morphology. A random effects model was used to pool the SMD and 95% CI to determine the effect. Due to the limited pre/post intervention data, only qualitative analyses were conducted.
Definitions of levels of evidence were adapted from van Tulder et al 19 and consistent with those used in previous reviews with similar included study types.20–22 Allocation of levels of evidence were based on the reporting quality and defined as: (1) strong if the pooled data were statistically homogenous (P>0.05) and obtained from three or more studies of which two were classed as high quality; (2) moderate if the pooled data were obtained from three or more studies, which were statistically heterogeneous (P<0.05), and one of the studies was classed as high quality; or data pooled from multiple moderate/low quality, statistically homogenous studies; (3) limited if the data obtained were from one high-quality study; or two homogenous moderate/low quality studies; or multiple statistically heterogeneous moderate/low quality studies; (4) insufficient if the data were obtained from one moderate/low-quality study; (5) conflicting if the pooled data were not statistically significant and from multiple statistically heterogeneous studies with inconsistent findings.
Results
Search strategy and reporting quality
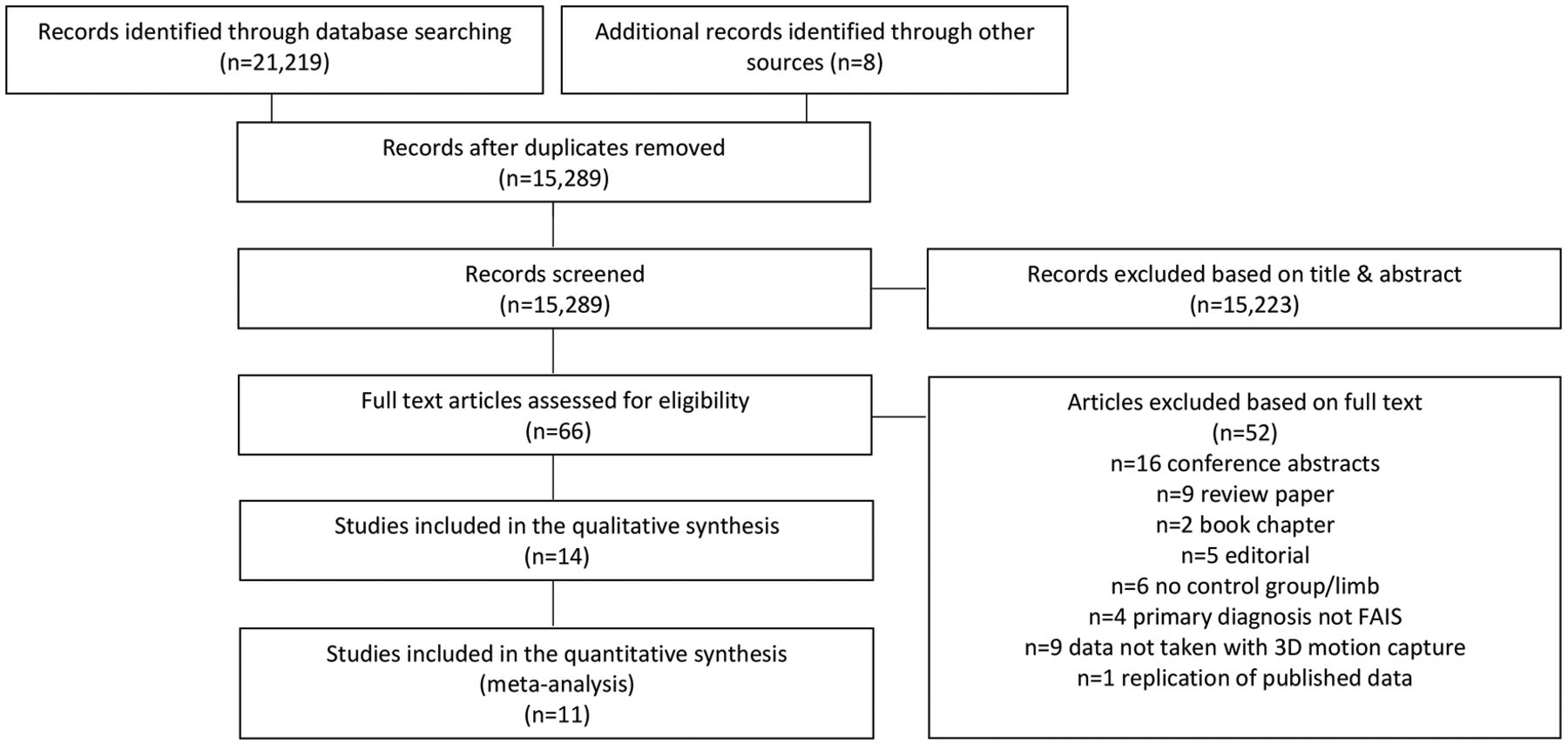
The search strategy identified 21 227 articles for evaluation (figure 1). Following the removal of duplicates, 15 289 articles were evaluated for inclusion. Title and abstract screening excluded 15 223 and 66 full-text articles were assessed for eligibility with 14 meeting the inclusion/exclusion criteria. Of the 14 included studies, 11 were cross-sectional and three were pre/post intervention studies. All studies investigated the biomechanics associated with the primary diagnosis of FAIS. Two intervention studies included control and pre-intervention data and were therefore included in both aims. One study23 presented some data that were a replication of a larger sample24; where the larger sample presented incomplete data, the smaller more complete data set was taken for the meta-analysis.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) study selection flow chart. FAIS, femoroacetabular impingement syndrome.
A total of 215 symptomatic patients (158 men, 57 women; mean age range 24.7–40.1 years) with the primary diagnosis of FAIS, as well as 236 controls (158 men, 78 women; 27.1–43.2 years) were included in the review (table 1 and 2). Seven of the 14 studies only included participants with cam-type FAIS (n=86, 56 men) and seven studies included a variety of cam, pincer and combined type FAIS. FAIS was diagnosed through X-ray, MRI or CT with alpha angle inclusion ranging from >50° to >60° for cam morphology and centre edge angle (CEA) inclusion ranging from >35° to >39° or a positive crossover sign for pincer morphology. No studies investigated the effects of conservative interventions and three case series studies evaluated the effects of surgical interventions on kinematics and joint torques.
Summary of included cross-sectional studies
Summary of included intervention studies
Comparisons in biomechanics between FAIS and controls were described during walking,12 23–29 squatting,28 30–32 drop landing,28 ascending stairs12 33 and sit-to-stand.34 Comparisons of pre/post intervention biomechanics were described during walking,12 23 squatting35 and ascending stairs.12 Reporting quality score per item ranged from 0.82 to 1.37 with zero high, nine moderate and five low-quality studies (online supplementary B). All included studies reported their aims/hypothesis, participant characteristics, used standardised motion capture methods and adjusted for covariates where applicable. No included studies blinded observers or outlined assessment period.
Supplementary file 2
Findings
Walking sagittal plane hip kinematics: FAIS versus controls
Pooled data of sagittal plane kinematics showed moderate evidence of a small effect for lower peak hip extension angle (SMD −0.40, 95% CI −0.71 to −0.09; heterogeneity I2=0%, P=0.60)12 24 25 27 28 and moderate evidence of a moderate effect for total sagittal plane ROM (−0.51, 95% CI −0.93 to −0.08; I2=0%, P=0.66)12 26 28 but no difference (−0.19, 95% CI −0.47 to 0.08; I2=0%, P=0.46) in peak hip flexion angle12 24–28 (figure 2A) during stance in patients with FAIS compared with controls (figure 2A).

(A) Meta-analysis of sagittal plane hip kinematics. (B) Meta-analysis of frontal plane hip kinematics. (C) Meta-analysis of transverse plane hip kinematics. (D) Meta-analysis of external joint torques; during walking. FAIS, femoroacetabular impingement syndrome; ROM, range of motion.
Two additional studies reported data on total ROM during a full walking cycle (ie, stance and swing phase),23 25 pooled data provided limited evidence of a large effect that patients with FAIS walked with less total sagittal plane ROM compared with controls (−0.98, 95% CI −1.57 to −0.40; I2=0%, P=0.43) (figure 2A).
Walking frontal plane hip kinematics: FAIS versus controls
Pooled data showed moderate evidence of no difference in peak hip adduction angle (−0.06, 95% CI −0.43 to 0.31; I2=27%, P=0.24)12 24 25 27 28 and peak hip abduction angle during stance (−0.29, 95% CI −0.77 to 0.20; I2=57%, P=0.07)12 24 26 27 (figure 2B). Total frontal plane ROM in stance was pooled from four studies, with moderate evidence (−0.31, 95% CI −0.84 to 0.23; I2=50%, P=0.11) of no difference between FAIS and control groups12 25 26 28 (figure 2B).
Qualitative synthesis of unpooled studies
One moderate quality study25 investigated peak hip abduction angle in swing phase, with insufficient evidence of no between-group differences (SMD −0.55, 95% CI −1.29 to 0.20) (table 3). One low-quality study23 reported data on frontal plane ROM in a full walking cycle. This review found insufficient evidence that patients with FAIS walked with less total frontal plane ROM compared with controls (−1.22, 95% CI −2.13 to −0.31) (table 3).
Hip kinematics, FAIS versus controls
Walking transverse plane hip kinematics: FAIS versus controls
Pooled transverse plane kinematics demonstrated moderate evidence of a moderate effect for lower peak hip internal rotation angle (−0.67, 95% CI −1.19 to −0.16; I2=47%, P=0.15)12 25 27 (figure 2C) but no difference in peak hip external rotation angle (0.14, 95% CI –0.18 to 0.46; I2=0%, P=0.41)12 26–28 and total transverse plane ROM (−0.14, 95% CI −0.73 to 0.45; I2=46%, P=0.16)12 26 28 during stance in patients with FAIS compared with controls (figure 2C). Total transverse plane ROM in a full walking cycle was reported in two studies, with pooled data showing limited evidence of no difference between groups (−0.08, 95% CI −0.63 to 0.47; I2=0%, P=0.65)23 25 (figure 2C).
Qualitative synthesis of unpooled studies
Two studies, with similar samples,23 24 reported peak hip internal and external rotation angles in a full walking cycle. The study with the larger sample reported no difference in peak internal and external rotation angles.24 Diamond et al 25 found no between-group differences (0.02, 95% CI −0.71 to 0.75) in peak hip external rotation angle in swing (table 3).
Walking pelvic kinematics: FAIS versus controls
Due to the variability in collection and inconsistencies of reporting pelvic kinematics, qualitative synthesis was performed on information regarding pelvic kinematics.
Sagittal plane pelvic kinematics: FAIS versus controls
One low-quality26 study and one moderate-quality12 study described limited evidence of no difference in peak anterior pelvic tilt angle during stance (0.16, 95% CI −0.78 to 0.46; 0.12, 95% CI −0.55 to 0.80, respectively) (table 4).One low-quality study26 found that patients with FAIS had a greater sagittal plane pelvic ROM in stance (0.85, 95% CI 0.20 to 1.50) and one moderate-quality study24 found no difference in total sagittal ROM during a full walking cycle (table 4).
Pelvic kinematics, FAIS versus controls
Frontal plane pelvic kinematics: FAIS versus controls
Frontal pelvic obliquity did not differ for pelvic drop (−0.31, 95% CI −0.93 to 0.3226; −0.48, 95% CI −1.20 to 0.2324) in one low-quality26 study and one moderate24-quality study or pelvic hike (rise) (−0.29, 95% CI −1.00 to 0.43) (table 4) in one moderate-quality study during stance phase.24 One low-quality study26 found no difference in total ROM in stance (−0.33, 95% CI −0.95 to 0.30) (table 4), whereas Kennedy et al 24 reported that patients with FAIS walked with less total pelvic frontal plane ROM during a complete walking cycle.
Transverse plane pelvic kinematics: FAIS versus controls
Transverse plane pelvic kinematics was evaluated by one low-qulity26 and two moderate-quality studies,12 24 and no studies reported any differences between groups. Specifically, no differences were reported for peak pelvic internal rotation angle in stance (−0.54, 95% CI −1.17 to 0.09)26 (table 4), peak internal and external rotation angles during a full walking cycle,24 total transverse plane ROM (−0.02, 95% CI −0.64 to 0.60; 0.20, 95% CI −0.47 to 0.88)12 26 (table 4) and total transverse plane ROM during a full walking cycle.24
Walking joint torques: FAIS versus controls
Five included studies reported joint torque information on FAIS versus controls. One additional moderate-quality study reported no between-group differences, but provided no data.24
Pooled data from five studies23 25 27–29 demonstrated moderate evidence of a moderate effect size for lower peak external rotation joint torque (−0.71, 95% CI −1.07 to −0.35; I2=0%, P=0.82) (figure 2D) in patients with FAIS compared with controls. There was moderate evidence of no difference in peak hip torques for flexion (−0.19, 95% CI −0.54 to 0.16; I2=21%, P=0.28), extension (−0.25, 95% CI −0.55 to 0.06; I2=0%, P=0.80), abduction (−0.04, 95% CI −0.39 to 0.31; I2=0%, P=0.53), adduction (−0.33, 95% CI −0.71 to 0.05; I2=0%, P=0.37) and internal rotation (−0.25, 95% CI −0.62 to 0.13; I2=0%, P=0.73) (figure 2D). Additionally, one moderate-quality29 study showed insufficient evidence that patients with FAIS had a greater peak hip flexion torque impulse (0.89, 95% CI 0.25 to 1.52) and no difference in extension torque impulse (−0.49, 95% CI −1.11 to 0.12) (table 5).
External joint torques, FAIS versus controls
Subgroup analysis: walking kinematics and joint torques: cam only versus controls
Subgroup analysis of joint kinematics and external joint torques in cam-only populations demonstrated limited evidence of no difference in peak hip extension angle (−0.53, 95% CI −1.12 to 0.06; I2=0%, P=0.82), and insufficient evidence of no difference in sagittal plane ROM (−0.45, 95% CI −1.48 to 0.58) compared with controls in the stance phase of walking (online supplementary C). Peak hip internal rotation in stance was unable to be subgrouped due to lack of data and no additional subgroup analyses differed from the reported results of the review.
Supplementary file 3
Sensitivity analysis: removal of data estimated from graphs
Sensitivity analyses were conducted where manually extracted data from published graphs were removed from the meta-analyses. Four sensitivity analyses were conducted with no noticeable changes in the reported results (online supplementary D).
Supplementary file 4
Squat kinematics: FAIS versus controls
Squatting kinematics was investigated in four studies.28 30–32 One study controlled squat height to a maximum depth of 25% of body height,28 two studies controlled squat height to a maximum depth of 1/3 tibial tuberosity height30 31 and one allowed maximum depth to be full range.32 Pooled data of reported squat depths showed moderated evidence of a large effect that FAIS participants squatted to a lesser depth than controls (SMD 0.92, 95% CI 0.46 to 1.38; I2=0%, P=0.77) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Meta-analysis of squat depth, FAIS versus controls. FAIS, femoroacetabular impingement syndrome.
Due to the variability in outcomes reported, kinematic squat variables were qualitatively synthesised. Hip kinematics were investigated by three medium-quality studies28 30 31 with no differences observed in all outcomes investigated. Specifically, no difference in peak hip angles in all three planes at maximum squat depth31; no difference in peak hip flexion, abduction and internal rotation angle between patients with FAIS and controls (flexion −0.62, 95% CI −1.36 to 0.11; abduction −0.01, 95% CI −0.73 to 0.70; internal rotation −0.65, 95% CI −1.39 to 0.09),30 (flexion 0.02, 95% CI −0.99 to 1.03; abduction −1.04, 95% CI −2.14 to 0.06; internal rotation −0.57, 95% CI −1.61 to 0.47)28; and no difference in total ROM in all planes (sagittal 0.58, 95% CI −0.46 to 1.63; frontal −0.26, 95% CI −1.28 to 0.76; transverse −1.06, 95% CI −2.17 to 0.04)28 (table 3).
Two medium-quality studies30 31 demonstrated no difference in pelvic tilt at maximum squat depth (0.73, 95% CI −0.01 to 1.4830; 0.70, 95% CI −0.11 to 1.50)31 (table 4). Total sagittal plane pelvic ROM was investigated in two moderate-quality studies31 32 with conflicting results. Lamontagne et al 31 found patients with FAIS squatted with less total sagittal plane pelvic ROM (−1.18, 95% CI −2.04 to −0.33) whereas Ng et al 32 found no between-group differences (−0.68, 95% CI −1.40 to 0.05) (table 4).
Squat joint torques: FAIS versus controls
Qualitative synthesis of unpooled studies
Squat hip joint torques were investigated in two moderate-quality studies. Kumar et al 28 found that patients with FAIS squatted with less peak hip external rotation torque (SMD −0.13, 95% CI −0.21 to −0.05) but no difference in peak hip flexion (0.19, 95% CI −0.83 to 1.21), peak hip abduction (0.00, 95% CI −1.01 to 1.01) or peak internal rotation (−0.34, 95% CI −1.37 to 0.69) (table 5) joint torque. Bagwell et al 30 found a lower mean hip flexion torque (−0.79, 95% CI −1.53 to −0.04), but no difference in mean hip abduction torque (0.20, 95% CI −0.51 to 0.92) and mean hip internal rotation torque (0.10, 95% CI −0.62 to 0.81) in patients with FAIS compared with controls.
Drop landing kinematics and joint torques: FAIS versus controls
Drop landing kinematics and joint torques were investigated in one moderate quality study,28 finding insufficient evidence of no difference in all hip kinematics and joint torque outcomes (table 3 and 5).
Stairs kinematics and joint torques: FAIS versus controls
Qualitative synthesis of unpooled studies
Stair ascent kinematics was investigated in one medium-quality12 study and one low-quality33 study with conflicting results. Hammond et al 33 found no difference in hip kinematics (table 3) whereas Rylander et al 12 found patients with FAIS demonstrated a smaller peak hip extension angle (−0.83, 95% CI −1.54 to −0.13), total hip sagittal plane ROM (−1.23, 95% CI −1.97 to −0.49) and peak hip internal rotation angle (−0.90, 95% CI −1.61 to −0.19) (table 3) compared with controls. Rylander et al 12 also found that patients with FAIS had greater total pelvic rotation ROM (0.95, 95% CI 0.24 to 1.67) and anterior pelvic tilt (1.23, 95% CI 0.49 to 1.97) (table 4) compared with controls. One low-quality study33 investigated hip joint torques during stair ascent. The results show insufficient evidence that patients with FAIS ascend stairs with a greater peak hip flexion joint torque (0.92, 95% CI 0.26 to 1.57) and no difference in peak hip extension and peak hip adduction torque (table 5).
Sit-to-stand joint torques: FAIS versus controls
Secondary outcome preintervention versus postintervention
Qualitative synthesis of unpooled studies
Three included studies (one moderate12 and two low quality23 35) investigated the effects of arthroscopic surgery on kinematics and joint torques in walking,12 23 squatting35 and ascending stairs12 (table 2). One study reported insufficient evidence of improvements in sagittal plane hip ROM, peak hip flexion angle, peak hip internal rotation angle and hip transverse plane ROM during stance phase of walking, following arthroscopic surgery.12 Another reported insufficient evidence of no differences during a full walking cycle following surgery.23 During a stair ascent, Rylander et al 12 found there was insufficient evidence of no change in hip and pelvic kinematics following arthroscopic surgery. During squatting, the postoperative participants with FAIS squatted to a lower depth with no difference in peak hip flexion angle.35
Discussion
Movement patterns of patients with FAIS were different from controls. Specifically, patients with FAIS had lower peak hip extension, total sagittal plane ROM and peak hip internal rotation during stance phase of walking and squatted to a lesser depth, with no difference in hip flexion range. The pooled results of hip kinematic differences during walking build on the results of the previous review,11 but few conclusions can be made for the other tasks, and for pelvic kinematics. These represent areas of future research.
Reduced hip extension towards terminal stance is consistent with findings in early-stage hip OA,36 end-stage hip OA37 and following total hip replacement.38 Reduced hip extension may be a strategy to reduce load on the anterior hip during walking.39 However, this behaviour has also been hypothesised to be maladaptive, decreasing the stimulus to anterior hip musculature, which can negatively affect hip stability over time.40 41 At this time, the implications of lower peak hip extension angle during walking are not known.
Patients with FAIS produced lower peak external rotation torque, and lower peak hip internal rotation angles during walking compared with controls. These adaptations may represent a strategy to avoid positions of internal rotation, which are often reported to be painful in patients with FAIS.5 As external moments are offset by internal moments of the antagonistic muscle groups/movements, a lower peak external rotation joint torque may decrease the demand on the internal rotators to minimise pain/discomfort.27
The effect size was small for lower peak hip extension angle (−0.40), moderate for lower peak hip internal rotation angle (−0.67) and moderate for lower peak hip external rotation torque (−0.71). The clinical implications of these differences and the long-term effects of alterations in biomechanics on joint health and long-term outcomes in patients with FAIS are relatively unknown, as no studies have evaluated these outcomes over time. Longitudinal studies into whether these differences in walking are associated with symptom or disease progression are needed to understand if such impairments may benefit from targeted management strategies, or whether they are protective movement patterns. Such information would enhance our understanding of the association between FAIS and OA.
Participants with FAIS did not squat as deep as controls, despite no difference in peak hip flexion angle. Reduced squat depth, but no difference in peak hip flexion angle may reflect poor motor programming, pain or fear of the task. Before recommendations can be made, greater investigations into the barriers to squat depth need to be explored. Since squatting type movements are required during everyday activities, patients with FAIS may benefit from skill retraining as a component of conservative management strategies.
There were insufficient studies to draw conclusions for clinical practice on tasks such as stair ascent, sit-to-stand and drop landing tasks. We recommend that further research be conducted into these and more complex activities to provide better insight into movement strategies associated with FAIS and whether targeting these differences could provide benefit in management strategies.
Over recent times there has been a rapid rise in the rates of arthroscopic surgery for FAIS.13 However, only three included studies evaluated the effects of surgical interventions on lower limb biomechanics during walking, squatting and ascending stairs. The conflicting results for the effect of surgery during walking may be due to surgical technique used (arthroscopic12 vs open/combined23), FAIS type (cam, pincer, combined cohort12 vs cam23) or follow-up time (12 months12 vs 10–32 months23). The results of the review indicate that surgical interventions may have no effect on hip kinematics during ascending stairs and squatting tasks. Further research, determining the effects of surgical intervention on biomechanics, is required to draw clinical conclusions. More stringent reporting of postoperative rehabilitation protocols is also required to better interpret results and draw recommendations. The review demonstrates the absence of studies evaluating the effect of exercise or physiotherapy on biomechanics in patients with FAIS, which should be addressed in future studies.
Limitations
There are limitations present in the included studies and in this review that require acknowledgement. The review only included studies published in the English language, potentially missing important information from studies published in other languages. Full data extraction was only completed by one author (MGK), with a random sample of 50% of the data extracted checked by the second author (PRL). Risk of bias assessment could not be performed with the reporting appraisal tool used for this study. Instead, cut-off scores for high, moderate and low reporting quality were defined. It is possible that studies with good reporting scores also have a high risk of bias. For example, all of the included studies scored ‘zero’ for outlining assessment period and blinding observers, resulting in a risk of potential detection bias. Additionally, all studies scored ‘zero’ for their generalisability of the results to relevant populations, decreasing the confidence in the external validity of the data presented. All of the included studies were case series or case–control, cross-sectional studies of low to moderate reporting quality and were included in the review regardless of their assessment, limiting the confidence in the findings of the review.42 Additionally, due to the differing units in joint torque data, and the kinematic models used, absolute differences were not determined at this time, and thus SMDs were used to calculate between-group differences in the outcomes of the included studies. The SMD provides an indication of the magnitude of the between-group difference enabling an interpretation of the pooled analyses beyond statistical significance.
There were differences in the kinematic models used in the included studies with six using a modified Helen Hayes marker set,23 24 27 31 32 35seven using a segmented model12 25 28–30 33 34 and an Oxford foot model with plug-in gait.26 Sagittal plane kinematics is the most reliable output for three-dimensional motion capture models (with the exception of pelvic tilt), followed by frontal and then transverse plane.43 Minimal detectable changes for three-dimensional motion capture analysis should be population specific44 and have yet to be quantified in patients with FAIS. Additionally, SE of measurement (SEM) should be quantified on a per-model basis, only one included study provided SEM values associated with their analysis.26 Due to under-reporting of data, temporal parameters of walking were not included in this review. There is an association between walking speed and hip joint kinematics and joint torques,45 which would need to be considered in future studies.
A variety of diagnostic criteria were used for the radiographic definition of FAIS with minimal alpha angles ranging from 50° to 60° and CEA from 35° to 39°. This inconsistency may have created variability in the included study results and altered the likelihood of between-group effects. The studies included in the review do not allow for the determination of cause or effect. Whether biomechanical variations occur early and cause FAIS, or FAIS causes these biomechanical variations, is unknown.
The majority of participants included were recruited from orthopaedic clinics, and hence may reflect more severe presentations than those in athletic teams or presenting to health or medical practitioner clinics. Future research should be conducted on athletic populations and involve sport-specific movements, such as running and cutting, to determine if more complex, higher impact activities present a problem for patients with FAIS. Women are also under-represented in the samples. Future studies could evaluate the association between FAIS and biomechanics in women, as smaller alpha angles and greater hip anteversion have been observed in women with hip and groin pain compared with men.46
Conclusion
The systematic review identified 11 cross-sectional and three pre-post intervention studies of low to moderate reporting quality. Based on pooled data of 11 studies, we found patients with FAIS exhibit alterations in hip movement strategies in activities such as walking and squatting, with insufficient evidence to draw significant clinical conclusions in tasks such as stair ascent, sit-to-stand and drop landings. The review found small to moderate alterations in hip movement strategies such as lower peak hip extension, peak internal rotation angle and peak external rotation joint torque during walking as well as a reduced squat depth in patients with FAIS compared with controls.
What is already known?
Femoroacetabular impingement syndrome (FAIS) is associated with decreased quality of life and persistent symptoms, and is a risk factor for the development of hip osteoarthritis. Synthesised information on movement strategies in patients with FAIS is limited.
What are the new findings?
There is moderate evidence that people with FAIS walk with a lower peak hip extension angle, peak hip internal rotation angle and external rotation joint torque, with no difference in peak hip flexion angle in stance.
There is moderate evidence that people with FAIS are unable to squat as deep as controls; however, this is not due to a difference in hip flexion range of motion.
References
Footnotes
Contributors All authors contributed to the planning, collection, analysis and writing of this manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.