
Abstract
The purpose of this study was to compare resistance exercise training (RT) to aerobic exercise training (AE) on the clinical risk factors for metabolic syndrome (MetSyn) in physically inactive overweight males (age 27–48 years). Subjects with at least one risk factor for MetSyn performed RT (n = 13, age 35.1 ± 4.7 years, BMI 31.2 ± 2.7 kg/m2) or AE (n = 9, age 37.6 ± 4.9 years, BMI, 31.2 ± 3.2 kg/m2) for 6 months. Training frequency and exercise session duration were equal and by 3 months the subjects exercised 4 day/week for 45 min/session. Blood lipids and glucose, waist circumference, and mean arterial blood pressure (MAP) were measured at 0, 3, and 6 months. A MetSyn z score was calculated for each subject from triglycerides, HDL cholesterol, fasting glucose, waist circumference, and MAP. Statistical significance was set at p ≤ 0.05. No significant differences existed between RT and AE groups at 0 month. AE showed a significant reduction in MetSyn z score from 0 (0.91 ± 3.57) to 6 months (−1.35 ± 2.95), while RT approached significance (p = 0.07) from 0 (0.09 ± 2.62) to 6 months (−1.30 ± 2.22). Triglycerides (mmol/L) significantly decreased in AE from 0 (1.93 ± 0.90) to 6 months (1.41 ± 0.70). Waist circumference (cm) significantly decreased in AE from 0 (106.8 ± 7.3) to 6 months (101.2 ± 6.5), and in RT from 0 (108.4 ± 9.0) to 6 months (105.7 ± 7.0). MAP (mmHg) decreased in RT from 0 (93.8 ± 5.8) to 6 months (87.5 ± 6.1) and in AE from 0 (97.6 ± 7.0) to 6 months (91.3 ± 6.8). With equal training frequency and exercise session duration, both RT and AE training, when paired with energy restriction improve the clinical risk factor profile for MetSyn.
Similar content being viewed by others

Introduction
Metabolic syndrome (MetSyn) is a clustering of disease risk factors including hypertension, decreased HDL cholesterol, elevated triglycerides, abdominal obesity, and insulin resistance (Grundy et al. 2005). Approximately 25% of adults in the United States have metabolic syndrome and the incidence of metabolic syndrome increases with age so that an estimated 43% of adults over 60 years of age have metabolic syndrome (Ford et al. 2002). MetSyn strongly predicts the risk of developing Type 2 diabetes, hypertension and cardiovascular disease (CVD) which remains the leading cause of death in the United States (Minino et al. 2007). A reduction in modifiable risk factors is thought to be the most effective way to prevent the onset of MetSyn and potentially cardiovascular disease (Grundy et al. 2005).
The National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) proposed a simple set of diagnostic criteria for metabolic syndrome based on common clinical measures including waist circumference, blood pressure, triglycerides, HDL cholesterol, and fasting blood glucose (Grundy et al. 2005). Participation in aerobic exercise training can reduce the clinical risk factors associated with MetSyn including lowering resting blood pressure (Fagard 2006), improving blood lipid profiles (Heath et al. 2007), improving glucose metabolism (Potteiger et al. 2003), and altering body composition (Donnelly et al. 2003). Participation in resistance exercise training has been shown to improve the clinical measures of MetSyn including resting blood pressure (Fagard 2006; Kelley 1997), blood lipid profile (Hurley et al. 1988; Yeater et al. 1996), body composition (Campbell et al. 1994; Chilibeck et al. 1996, 1998; Kraemer et al. 2001; Van Etten et al. 1997), and insulin and glucose metabolism (Ibanez et al. 2005; Smutok et al. 1993, 1994; Eriksson et al. 1997; Van Etten et al. 1997; Chilibeck et al. 1996).
Several studies have attempted to compare resistance exercise training and aerobic exercise training on risk factor reduction for CVD (Banz et al. 2003; Smutok et al. 1993), as well as control of blood glucose in patients with Type 1 (Ramalho et al. 2006) and Type 2 diabetes (Sigal et al. 2007; Smutok et al. 1994). Collectively, the results of these studies indicate that both resistance exercise training and aerobic exercise training can improve the cardiovascular disease risk factor profile and certain aspects of metabolic control. A significant limitation of the previous work has been whether the treatment groups have performed the same volume of exercise. It is difficult to compare the two forms of exercise due to limitations in measuring and equating both training intensity and training volume. Intuitively, individuals participating in an exercise program will often perform the exercise sessions based on the amount of time the individual has available for training. In this investigation, we matched training frequency and exercise session duration in an attempt to compare the effect of resistance exercise training and aerobic exercise training, when paired with energy restriction, on MetSyn risk profiles and specific CVD risk factors in previously sedentary males. We hypothesized that resistance exercise training would result in a similar reduction in the risk factors for both MetSyn and CVD compared to aerobic exercise training when both forms of exercise are performed for the same training frequency and exercise session duration and when paired with energy restriction.
Methods
Design
The study was a 6-month randomized intervention to evaluate the effects of either resistance exercise training (RT) or aerobic exercise training (AE) on MetSyn risk factors in physically inactive males. The training programs were matched for training frequency and exercise session duration. Data on body weight and composition, resting blood pressure, blood chemistry profile, and cardiorespiratory fitness were collected at 0 (baseline), 3, and 6 months.
Subjects
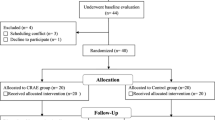
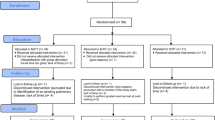
We recruited 35 overweight males for participation in this study of which 22 completed the 3- and 6-month assessments. The 13 subjects who withdrew from the study cited having a lack of time available for participation. All laboratory measures were obtained after the subject signed an informed consent and completed a health history questionnaire in accordance with university guidelines on human experimentation. At the start of the study all subjects were physically inactive, having not participated in more than 15 min of regular exercise per week for at least previous 3 months. All subjects had an initial body mass index between 27.1 and 35.9 kg/m2 with each subject having at least one risk factor for MetSyn. Exclusion criteria were history of coronary heart disease, bone or joint disease, inability to perform laboratory tests or the exercise programs, or any medical condition which would make exercise an unnecessary risk.
Dietary counseling
At the start of the study, subjects filled out 3-day dietary records. The subjects then underwent individualized dietary counseling in which the counselor emphasized lower portion sizes and lower fat choices to reduce dietary intake by 300–600 kcal. No further dietary counseling occurred from that point forward. Subjects also completed 3-day dietary records at 3 and 6 months to determine their total energy intake.
Intervention programs
The RT group participated in an individualized resistance training program (Dolezal and Potteiger 1998). Exercises were employed that allowed training for all the major muscle groups such as parallel squat, leg press, supine bench press or dumbbell chest press, military press or dumbbell shoulder press, lat pull-down, seated rows, leg curls, leg extensions, calf raises, arm curls, and sit-ups. The training program followed typical repetition maximum (RM) resistance training principles for progression in the intensity and volume of exercise in a program. The resistance training protocol utilized a model, where the training loads were changed within each week. The subjects varied their training intensity for the exercises on different days. On the high intensity days, the subjects completed between 5 and 7 repetitions with 100% of their 5–7 RM. On the moderate intensity days, the subjects completed between 8 and 10 repetitions with 80% of their 8–10 RM. The subjects progressed from one set per exercise at the beginning of the study to four sets by the beginning of week 4. Short rest periods of ~1–2 min between sets and exercises were used.
The AE program was designed to elicit a target heart rate of between 65 and 80% of maximal cardiorespiratory fitness as determined from graded exercise testing. Individual adjustments to training intensity were made after 3 months to account for changes in aerobic fitness. The primary mode of exercise was treadmill walking and jogging. Stationary cycling and stationary stair climbing were available to the subjects 1 day per week in an effort to reduce boredom, decrease the chance for overuse or repetitive injuries, and increase exercise adherence.
The exercise sessions for both training groups increased in duration from 20 min at the beginning of the study to 45 min by week 5. The RT group increased the number of sets per exercise in order to meet the required duration of training. Subjects began training by exercising 3 days per week, then progressed to 4 days per week by 3 months, and continued at 4 days per week for the remainder of the study. An exercise specialist supervised each subject with one-on-one training during the exercise sessions. All training sessions were conducted in the university exercise facility.
Body weight and composition
Body weight was assessed on a calibrated electronic scale (Toledo Model 8134) with the subjects in shorts and T-shirts only, having removed all jewelry. The weighing of subjects occurred at ~0600 h after the subject had voided. Body composition was assessed using Lunar DPX-IQ dual energy X-ray absorptiometry (DEXA) (Lunar, Inc., Madison, WI, USA). This technique provided a measure of fat mass, fat-free mass, and percent body fat. Subjects were clothed in shorts and T-shirts and analyzed using the scanning speeds and modes recommended by the manufacturer. The scanner was calibrated according to the guidelines specified by the manufacturer. Circumference measures of the waist, at the level of the umbilicus, were taken in triplicate using a spring loaded tape measure (Gulick II), with the closest two measures averaged for statistical analysis.
Resting blood pressure
After the measurement of body composition, the subjects’ rested for 30 min while resting metabolic rate was measured (data not reported). Blood pressure was then assessed using a mercurial sphygmomanometer and stethoscope. This ensured at least a 30-min period of total inactivity prior to the blood pressure assessment. The subject was positioned supine and the same research technician made the blood pressure measurements. Systolic and diastolic pressures were recorded using the muffling of sound (Korotkoff phase 4) as the diastolic reading. Blood pressure was assessed in duplicate with the values averaged for statistical analysis. Mean arterial pressure (MAP) at rest was calculated as [(systolic blood pressure − diastolic blood pressure) × 0.33] + diastolic blood pressure.
Blood chemistry profile
Blood for fasting glucose, insulin, and lipids was obtained after the measurement of resting blood pressure. Glucose was measured with a glucose oxidase kit (Sigma, St. Louis, MO, USA) and insulin was measured by radioimmunoassay (DPC, CA, USA). Within run coefficients of variation were <2.5 and <3.1 for glucose and insulin, respectively. Insulin resistance was determined by the homeostatic model assessment (Matthews et al. 1985). Total cholesterol and lipoprotein concentrations were measured with an automated analyzer (Olympus AU5200, Melville, NY, USA) using standard enzymatic techniques. The VLDL-C and LCL-C fractions were calculated using the Friedewald formula (Friedewald et al. 1972).
Cardiorespiratory fitness
Maximal oxygen consumption (VO2max) was measured during a graded exercise test on a treadmill ergometer. The modified Bruce protocol was used during testing (American College of Sports Medicine, 2010). Heart rate using a radiotelemetry unit (Polar Instruments) and rating of perceived exertion, using the 15-point Borg scale (Borg 1970), were recorded during the last 30 s of each 3-min stage. Expired air was measured for oxygen and carbon dioxide concentrations at 1 min intervals using a Sensormedics 2900 metabolic measurement cart (Sensormedics Corp., Yorba Linda, CA). This system was calibrated before each test according to the manufacturer’s instructions. A test was considered maximal if the subject achieved any three of the four following criteria: a plateau in oxygen consumption (<2.0 ml/kg/min) with an increase in exercise intensity, respiratory exchange ratio ≥1.10, a maximal heart rate within ±10 beats per minute of age-predicted values, and volitional exhaustion (Duncan et al. 1997). All subjects reached at least three of the four criteria during testing.
Macronutrient intake
Measurements of total energy and macronutrient intake occurred at 0, 3, and 6 months. Twenty-four hour diet log books were obtained using 2 weekdays and 1 weekend day during a 1-week time period. Subjects were instructed in recording brand name, portion size, and method of preparation and ingredients and they were encouraged to bring in labels or packages of foods consumed. Analysis of macronutrient consumption data was completed using the Food Processor® computer program (esha, Salem Oregon).
Statistical analysis
We used the revised NCEP ATP III criteria for MetSyn: (1) increased waist circumference (≥102 cm in men); (2) increased triglycerides (≥150 mg/dl); (3) decreased HDL cholesterol (<40 mg/dl in men); (4) increased blood pressure (≥130 mmHg systolic or ≥85 mmHg diastolic); and (5) increased fasting glucose (≥100 mg/dl) (Grundy et al. 2005). To test for the effects of exercise training on MetSyn, we used a continuous z score rather than a series of dichotomous scores. This concept has been proposed by others as a way to more accurately represent and detect overall metabolic changes for several reasons (Johnson et al. 2007; Wijndaele et al. 2006; Franks et al. 2004). First, the continuous score would be more sensitive to small and large changes that do not change the ATP III criteria. For example, a decrease in triglycerides from 250 to 151 mg/dl would have no effect on the ATP III score, but would be reflected as a non-trivial change in the continuous MetSyn risk factor index. Second, the continuous score would be less sensitive to small changes that occur in the vicinity of the diagnostic criteria for any one variable. For example, a decrease in triglycerides from 152 to 149 mg/dl would have a non-trivial effect on the NCEP ATP III score, but little effect on the continuous MetSyn risk factor index (Johnson et al. 2007).
We calculated a MetSyn z score that reflects a continuous score of the five MetSyn risk factors. The MetSyn z score was calculated from individual subject data, NCEP ATP III criteria, and standard deviations using data from the entire subject cohort at baseline. The equation used was: z score = ([40 − HDL cholesterol]/SD)+([triglycerides − 150]/SD)+([fasting plasma glucose − 100]/SD)+([waist circumference − 102]/SD)+([mean arterial pressure − 100]/SD) (Johnson et al. 2007; Wijndaele et al. 2006; Franks et al. 2004). A frequency count of MetSyn risk factors was also performed at each time point with the average number of MetSyn risk factors determined for each training group.
Descriptive statistics (mean and standard deviations) were calculated for each variable at each of the time points (0, 3, 6 months) in the study. Mixed effects repeated measures analysis of variance (ANOVA) models were fit to assess the effect of treatment group (resistance training, aerobic training) and time (0, 3, 6 months) on mean responses for the measured dependent variables. Statistical significant was accepted with p < 0.05. Planned contrasts were constructed to compare the effects of treatment within time periods and to compare the effect of time within a treatment condition. All contrast comparisons used Bonferroni-adjusted significance levels, maintaining a family-wise error rate of α = 0.05.
Results
Subjects
There were no injuries reported as a result of performing either training program. Of the subjects who completed the study, 13 were in the RT group and 9 were in the AE group. Subjects in the RT group completed 96% of the exercise sessions, while subjects in the AE group completed 93% of the exercise sessions. There were no significant differences in any of the dependent measures between groups prior to beginning of the training programs. Subjects in the RT group were 35.1 ± 4.7 years of age with a height of 182.0 ± 7.0 cm, while those in the AE group were 37.6 ± 4.9 years of age with a height of 181.0 ± 9.0 cm.
Dietary intake
The AE group reported a caloric intake of 2,950 ± 686 kcal at 0 months, 1,880 ± 511 kcal at 3 months, and 1,990 ± 493 kcal at 6 months. The RT group reported a caloric intake of 2,869 ± 795 kcal at 0 month, 2,139 ± 524 kcal at 3 months, and 2,150 ± 545 kcal at 6 months. The self-reported total energy intake was significantly lower at 3 and 6 months compared to baseline in both groups. There were no significant differences between the two groups at any measurement time.
Metabolic syndrome risk factors
The MetSyn z scores and variables that comprise the z score are shown in Table 1. The MetSyn z score decreased in both RT and AE with the 6-month value significantly different from baseline in AE and approaching significance in RT (p ≤ 0.07). There were no significant differences between the two training groups at any time point. The average number of MetSyn risk factors was not significantly different between groups at any time point and there was no change in either group in response to the training program. HDL cholesterol significantly decreased in RT from 0 to 3 months and then was unchanged at 6 months; there were no changes in the AE group. There was a significant decrease in triglycerides from 3 to 6 months in RT and at 3 and 6 months compared to 0 month for the AE training group. There was no change in fasting blood glucose after AE or RT. Waist circumference was significantly reduced at 3 and 6 months compared to 0 month in RT. Waist circumference significantly decreased throughout the 6 months of training in AE with 3 months significantly different from 0 month and 6 months significantly different from both 0 and 3 months. MAP was significantly reduced from 0 months at both 3 and 6 months in RT. For AE, MAP was significantly lower at 6 months compared to 0 and 3 months. There was a significant difference between the RT and AE training groups in MAP at 3 months of training. No other significant between group differences were observed.
Body mass and composition
Data for body mass and composition measurements are shown in Table 2. A significant reduction in body mass was observed throughout the 6 months of training for AE with 3 months lower than 0 and 6 months lower than both 0 and 3 months. There were no significant changes in body mass in the RT group. Both groups demonstrated a significant reduction in body fat % in response to the training program, with the values observed at 6 months of training significantly lower than those recorded at 0 and 3 months. Fat-free mass increased in the RT with 0 months significantly different from 3 and 6 months. There was no change in fat-free mass in the AE group and there were no differences between the groups. Fat mass was significantly lower at 6 months compared to 0 months in the RT group. For the AE group, fat mass was significantly decreased after 3 and 6 months.
Cardiorespiratory fitness and blood pressure
Data for cardiorespiratory fitness and blood pressure are shown in Table 3. Maximal oxygen consumption (L/min) increased during training for the AE group approaching statistical significance (p = 0.07). There were no significant changes in VO2max for the RT training group. Significant reductions in systolic blood pressure were observed following training in both groups. For the RT group, there was approximately a 3.7% decrease in systolic blood pressure from 0 month. Systolic blood pressure was significantly lower after 3 (4.5% decrease) and 6 months (7.1% decrease) of training in the AE group. Diastolic blood pressure was significantly reduced in the RT group from 0 to 3 months (7.1% decrease) with the 6 months value (8.5% decrease) also significantly different from 0 month. Diastolic blood pressure did not significantly change in the AE group.
Blood chemistry profile
The results for the additional blood chemistry measurements are illustrated in Table 4. There were significant reductions in fasting insulin concentration with the 6 months values lower than 0 months for both RT and AE. There was a significant improvement in insulin sensitivity as measured by HOMA at 6 months compared to 0 month and 3 months for both the RT and AE training groups. There were no differences between groups for fasting insulin HOMA at any measurement time. No significant between groups or within group time effects were observed in the blood lipid measures of total cholesterol, LDL, and VLDL.
Discussion
The major findings of this investigation indicate that 6 months of RT or AE training performed at similar daily exercise durations and weekly training frequencies, when paired with dietary energy restriction, can improve the MetSyn and CVD risk profile in sedentary overweight middle aged men. Specifically, we demonstrated that (1) both RT and AE training reduced the risk for MetSyn as determined through a cumulative z score; (2) both training methods altered waist circumference, MAP, body composition and insulin sensitivity; and (3) only AE improved cardiovascular fitness and triglyceride levels.
Several investigations have attempted to compare RT and AE on MetSyn and CVD risk factors such as resting blood pressure, blood lipid profiles, insulin sensitivity, cardiorespiratory fitness, and body composition (Ramalho et al. 2006; Banz et al. 2003; Sigal et al. 2007; Smutok et al. 1993, 1994; Johnson et al. 2007). However, rarely have the two training modes been equal in the total amount of work performed (Ramalho et al. 2006). This is likely due to the difficulties in equating training intensity and volume and the total amount of work performed between the two forms of exercise. With this in mind, we attempted to compare RT and AE by matching weekly training frequency and daily exercise session duration for the two groups over a 6-month period. While this method does not minimize the limitations of comparing the two types of exercise with respect to exercise intensity and training volume, it does provide practical information to anyone using exercise to reduce MetSyn risk factors and CVD. Overall, the data from this study indicate that MetSyn and CVD risk reduction can be achieved by combining dietary energy restriction with either high intensity RT or AE. The remainder of this discussion is designed to provide support for both RT and AE having a positive influence on the specific variables related to MetSyn and CVD.
Metabolic syndrome
The use of the z score to evaluate exercise changes in the risk for MetSyn provides an increased level of sensitivity for reasons described previously (Johnson et al. 2007; Wijndaele et al. 2007). For example, in the current study there was no statistically significant change in the average number of risk factors per subject (Table 1) yet there were statistically significant reductions in several of the individual risk factors for both the RT and AE groups. Collectively, these positive changes resulted in a significant reduction in the risk for MetSyn in the AE group. It could be argued that the reduction in the MetSyn z score for the RT while not statistically significant at the p ≤ 0.05 level is meaningful given the significant decrease in waist circumference and MAP. When this information is viewed in conjunction with the changes in other CVD risk factors, such as a reduction in fat mass and improvement in insulin sensitivity, one can conclude that both RT and AE, when combined with dietary energy restriction, improve the risk factor profile for MetSyn and CVD. The lowering of the z score risk profile for MetSyn by AE is similar to what others have found in at risk patients (Johnson et al. 2007). In addition, we found that AE significantly reduced individual risk factors as others have found previously. These include reducing triglycerides levels (Halbert et al. 1999), waist circumference (Sigal et al. 2007), and MAP (Whelton et al. 2002).
Body mass and composition measures
Excess body fat has been linked to a variety of medical disorders including hypertension, hyperlipidemia, coronary artery disease, insulin resistance, and diabetes mellitus (Barret-Connor, 1985; Blair and Brodney, 1999; Bonora et al. 1997; Faloia et al. 2000; Gillum et al. 1998; Goran and Gower, 1998). Furthermore, abdominal obesity has been specifically linked to the development of Type 2 diabetes mellitus (Bjorntorp, 1988; Després, 1993; Pouliot et al. 1992), elevated blood lipid levels (DiPietro et al. 1999; Pouliot et al. 1992) and heart disease (Lamarche 1998).
The data from the current study indicate that both RT and AE when paired with dietary energy restriction can positively affect body composition by causing significant reductions in body fat % and total fat mass (Table 2). When viewed in conjunction with the waist circumference data, these changes are important for reducing the negative health outcomes associated with increases in intra-abdominal obesity. Previous research comparing RT to AE has provided mixed results regarding changes in body composition. Some studies show reductions in body fat % with AE (Smutok et al. 1993) and RT (Banz et al. 2003) as well as reductions in subcutaneous fat with both modes of exercise (Sigal et al. 2007), including AE paired with energy restriction (Shinkai et al. 1994). Conversely, other investigations showed no change in several body composition measures with either AE or RT (Smutok et al. 1993, 1994; Banz et al. 2003). The lack of differences between the two modes of exercise training in the current study suggest that RT and AE may help lower the risk of MetSyn and CVD by reducing overall levels of body fat and specifically waist circumference levels.
Cardiovascular fitness and resting blood pressure
Low cardiovascular fitness is a more powerful predictor of mortality among men than any other established risk factors (Myers et al. 2002; Kokkinos et al. 2008) and also is a strong predictor of increased risk for CVD (Blair et al. 1996). Therefore, positive changes in VO2max should result in a reduction of risk for both CVD and early mortality (Blair et al. 1996). In the current study improvements in VO2max were observed for the AE group (11.4%), with no change in the RT group. This response is consistent with the previous research when comparing AE and RT on cardiovascular fitness (Smutok et al. 1993, 1994). These results were expected and were likely influenced by a combination of relatively high initial levels of VO2max and an insufficient aerobic training stimulus during the RT sessions.
When chronically elevated as in hypertension, blood pressure is an independent risk factor for coronary artery disease and is associated with many other cardiovascular disorders (Matthews et al. 1990). Several recent meta-analyses have shown that resting blood pressure is reduced in both RT (Kelley 1997; Kelley and Kelley 2000) and AE (Whelton et al. 2002) studies that were short term in nature. The reductions in blood pressure observed in both the RT and AE groups from the current study are consistent with changes observed in other RT and AE studies (Kelley 1997; Kelley and Kelley 2000). This is significant because modest reductions in resting diastolic blood pressure have been associated with reduced risk of stroke and development of coronary heart disease (Collins et al. 1990; MacMahon et al. 1990).
Blood chemistry profile
Abnormal glucose metabolism is associated with an increased risk of many diseases including Type 2 diabetes, coronary artery disease, and stroke (Wing et al. 2007), while improvements in glucose metabolism have been shown to decrease the risk for a variety of disease conditions (Praet and Van Loon 2007). In studies comparing different exercise modes both AE and RT training have been shown to improve glucose metabolism (Smutok et al. 1994; Smutok et al. 1993; Sigal et al. 2007; Eriksson et al. 1998). In the current study, the significant decrease in fasting insulin and insulin resistance for both AE and RT are consistent with prior research and support an improvement in the CVD risk factor profile.
Hyperlipidemia is associated with increased risk for CVD, atherosclerosis, and diabetes mellitus. AE improves blood lipid and lipoprotein levels (Halbert et al. 1999), but the effect of RT on blood lipids is less clear (Halbert et al. 1999). The results from the current study, which employed an exercise protocol combined with dietary restriction, follow closely those of past research with AE and RT causing no changes in total cholesterol, LDL cholesterol, and VLDL cholesterol (Table 4) (Smutok et al. 1993; Banz et al. 2003; Ramalho et al. 2006; Sigal et al. 2007). There were two exceptions, however, in the AE group there was a significant decrease in triglyceride levels and in the RT group there was a significant decrease in the HDL cholesterol levels. Factors such as subject age, initial level of blood lipids, dietary intake, and training intensity and frequency can influence whether AE or RT have a positive impact on blood lipid levels (Halbert et al. 1999).
A potential limitation in this study is the inability to compare the RT and AE groups to determine if training intensity or training volume is equal between the two modes of exercise. Many of the variables assessed in the current study have been shown to be more or less responsive to the intensity and volume of individual training programs and thus there is no way to be sure that both groups worked at the same intensity and completed the same total training volume. We acknowledge this potential limitation but would like to point out the importance of the practical application of the results that individuals at risk for MetSyn can have some flexibility in the choice of exercise activities selected to improve health. A second potential limitation could be the lack of an experimental control group. Numerous investigators have argued that a control group is not always necessary in experimental research, particularly if health could be adversely affected by not participating in a treatment group. We believe that the results from a control group would demonstrate what has occurred in many other investigations; there is no positive change in health related measures if individuals remain sedentary (Smutok et al. 1994, 1993). A final limitation is the lack of a dietary restriction group only that would allow for the determination of the influence of caloric restriction alone on the dependent variables.
Conclusions
When matched for training frequency and exercise session duration, and when paired with dietary energy restriction, both RT and AE improve individual risk factors of the metabolic syndrome with AE significantly improving the MetSyn z score risk profile. Both forms of exercise improved the risk profile for CVD with AE changing triglyceride levels, waist circumference, MAP, body mass, body fat %, fat mass, cardiorespiratory fitness, fasting insulin, and insulin resistance. RT improved the risk profile for CVD by positively affecting waist circumference, mean arterial blood pressure, body fat %, fat mass, fasting insulin, and insulin resistance. Future research should examine different combinations of RE and AE to determine if an optimal AE or RT program that results in an improved risk profile for previously sedentary and overweight individuals could be developed that could lower the amount of time need to improve the risk factor profile.
References
American College of Sports Medicine (2010) ACSM’s Guidelines for Exercise Testing and Prescription, 7th ed edn. Williams and Wilkins, Philadelphia Lippincott
Banz WJ, Maher MA, Thompson WG, Bassett DR, Moore W, Ashraf M et al (2003) Effects of resistance versus aerobic training on coronary artery disease risk factors. Exp Biol Med 228:434–440
Barret-Connor E (1985) Obesity, atherosclerosis, and coronary artery disease. Ann Intern Med 103:1010–1019
Bjorntorp P (1988) Abdominal obesity and the development on non-insulin dependent diabetes mellitus. Diabetes Metab Rev 4:615–622
Blair SN, Brodney S (1999) Effects of physical inactivity and obesity on morbidity and mortality: current evidence and research issues. Med Sci Sports Exerc 31:S646–S662
Blair SN, Kampert JB, Kohl HW, Barlow CE, Macera CA, Paffenbarger RS et al (1996) Influences of cardiorespiratory fitness and other precursors on cardiovascular disease and all-cause mortality in men and women. JAMA 276:205–210
Bonora E, Targher G, Zenere MB, Saggiani F, Alberiche MP, Branzi P et al (1997) Obesity worsens cardiovascular risk profiles independently of hyperinsulinaemia. J Intern Med 241:470
Borg GAV (1970) Perceived exertion as an indicator of somatic stress. Scand J Rehabil Med 2:92–98
Campbell WW, Crim MC, Young MR, Evans WJ (1994) Increased energy requirements and changes in body composition with resistance training in older adults. Am J Clin Nutr 60:167–175
Chilibeck PD, Calder A, Sale DG, Webber CE (1996) Twenty weeks of weight training increases lean tissue mass but not bone mineral mass or density in healthy, active young women. Can J Physiol Pharmacol 74:1180–1185
Chilibeck PD, Calder AW, Sale DG, Webber CE (1998) A comparison of strength and muscle mass increases during resistance training in young women. Eur J Appl Physiol 77:170–175
Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, Eberlein KA et al (1990) Blood pressure, stroke, and coronary heart disease. Part 2, short-term reductions in blood pressure: overview of randomized drug trials in their epidemiological context. Lancet 335:827–838
Després JP (1993) Abdominal obesity as in important component of insulin resistance syndrome. Nutrition 9:452–459
DiPietro L, Katz LD, Nadel ER (1999) Excess abdominal adiposity remains correlated with altered lipid concentrations in healthy older women. Int J Obes 23:432–436
Dolezal BA, Potteiger JA (1998) Concurrent resistance and endurance training influence basal metabolic rate in non-dieting individuals. J Appl Physiol 85:695–700
Donnelly JE, Hill JO, Jacobsen DJ, Potteiger JA, Sullivan D, Johnson T et al (2003) The effects of a 16-month, randomized, controlled exercise trial on body weight and composition in young, overweight men and women. Arch Intern Med 163:1343–1350
Duncan GE, Howley ET, Johnson BN (1997) Applicability of VO2max criteria: discontinuous versus continuous protocols. Med Sci Sports Exerc 29:273–278
Eriksson J, Taimela S, Eriksson K, Parviainen S, Peltonen J, Kujala U (1997) Resistance training in the treatment of non-insulin dependent diabetes mellitus. Int J Sports Med 18:242–246
Eriksson J, Tuominen JA, Valle T, Sundberg S, Sovijarvi A, Lindholm H et al (1998) Aerobic endurance exercise or circuit-type resistance training for individuals with impaired glucose tolerance? Horm Metab Res 30:37–41
Fagard RH (2006) Exercise is good for your blood pressure: effects of endurance training and resistance training. Clin Exp Pharmacol Physiol 33:853–856
Faloia E, Giacchetti G, mantero F (2000) Obesity and hypertension. J Endocrinol Invest 23:54–62
Ford ES, Giles WH, Dietz WH (2002) Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA 287:356–359
Franks PW, Ekelund U, Brage S, Wong M, Wareham N (2004) Does the association of habitual physical activity with the metabolic syndrome differ by level of cardiorespiratory fitness? Diabetes Care 27:1187–1193
Friedewald WT, Levy RI, Frederickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18:499–502
Gillum RF, Mussolino ME, Madans J (1998) Body fat distribution and hypertension incidence in women and men The NHANES 1 epidemiologic follow-up study. Int J Obes 22:127–134
Goran MI, Gower BA (1998) Abdominal obesity and cardiovascular risk in children. Coron Artery Dis 9:483–487
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA et al (2005) Diagnosis and Management of the Metabolic Syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement: Executive Summary. Circulation 112:e285–e290
Halbert JA, Silagy CA, Finucane P, Withers RT, Hamdorf PA (1999) Exercise training and blood lipids in hyperlipidemic and normolipidemic adults: a meta-analysis of randomized, controlled trials. Eur J Clin Nutr 53:514–522
Heath GW, Ehsani AA, Hagberg JM, Hinderliter JM, Goldberg AP (2007) Exercise training improves lipoprotein lipid profiles in patients with coronary artery disease. Am Heart J 105:889–895
Hurley BF, Hagberg JM, Goldberg AP, Seals DR, Ehsani AA, Brennan RE et al (1988) Resistive training can reduce coronary risk factors without altering VO2max or percent body fat. Med Sci Sports Exerc 20:150–154
Ibanez J, Izquierdo M, Arguelles I, Forga L, Larrion JL, Garcia-Unciti M et al (2005) Twice-weekly progressive resistance training decreases abdominal fat and improves insulin sensitivity in older men with Type 2 diabetes. Diabetes Care 28:662–667
Johnson JL, Slentz CA, Houmard JA, Samsa GP, Duscha BD, Aiken LB et al (2007) Exercise training amount and intensity effects on metabolic syndrome (from Studies of a Targeted Risk Reduction Intervention through Defined Exercise). Am J Cardiol 100:1759–1766
Kelley GA (1997) Dynamic resistance exercise and resting blood pressure in adults: a meta-analysis. J Appl Physiol 82:1559–1565
Kelley GA, Kelley KS (2000) Progressive resistance exercise and resting blood pressure. Hypertension 35:838–843
Kokkinos PF, Myers J, Kokkinos JP, Pittaras A, Narayan P, Manolis A et al (2008) Exercise capacity and mortality in black and white men. Circulation 117:614–622
Kraemer WJ, Keuning M, Ratames NA, Volek JS, McCormick M, Bush JA et al (2001) Resistance training combined with bench-step aerobics enhances women’s health profile. Med Sci Sports Exerc 33:259–269
Lamarche B (1998) Abdominal obesity and its metabolic compliances: implications for the risk of ischaemic heart disease. Coron Artery Dis 9:473–481
MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J et al (1990) Blood pressure, stroke, and coronary heart disease. Part 1, prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 335:765–774
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC (1985) Homeostasis model assessment: insulin resistance and B-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28:412–419
Matthews JNS, Altman DG, Campbell MJ, Royston P (1990) Analysis of serial measurements in medical research. Br Med J 300:230–235
Minino AM, Heron MP, Murphy SL et al (2007) Deaths: Final Data for 2004 (Rep. No. 55-19). US Department of Health and Human Services
Myers JN, Prakash M, Froelicher VF, Do D, Partington S, Atwood JE (2002) Exercise capacity and mortality among men referred for exercise testing. N Engl J Med 346:793–801
Potteiger JA, Jacobsen DJ, Donnelly JE, Hill JO (2003) Glucose and insulin responses following 16 months of exercise: The Midwest Exercise Trial (MET). Metabolism 52:1175–1181
Pouliot MC, Després JP, Nadeau A, Moorjani S, Prud’homme S, Lupien PJ et al (1992) Visceral obesity in men: associations with glucose tolerance, plasma insulin, and lipoprotein levels. Diabetes 41:826–834
Praet SFE, Van Loon LJC (2007) Optimizing the therapeutic benefits of exercise in Type 2 diabetes. J Appl Physiol 103:1113–1120
Ramalho AC, de Lourdes Lima M, Nunes F, Cambui Z, Barbosa C, Andrade A et al (2006) The effect of resistance versus aerobic training on metabolic control in patients with type-1 diabetes mellitus. Diabetes Res Clin Pract 72:271–276
Shinkai S, Watanabe S, Kurokawa Y, Torii J, Asai H, Shephard RJ (1994) Effects of 12 weeks of aerobic exercise plus dietary restriction on body composition, resting energy expenditure and aerobic fitness in mildly obese middle-aged women. Eur J Appl Physiol 68:258–265
Sigal RJ, Kenny GP, Boule NG, Wells GA, Prud’homme D, Fortier M et al (2007) Effects of aerobic training, resistance training, or both on glycemic control in Type 2 diabetes. Ann Intern Med 147:357–369
Smutok MA, Reece C, Kokkinos PF, Farmer C, Dawson P, Shulman R et al (1993) Aerobic versus strength training for risk factor intervention in middle-aged men at high risk for coronary heart disease. Metabolism 42:177–184
Smutok MA, Reece C, Kokkinos PF, Farmer CM, Dawson PK, DeVane J et al (1994) Effects of exercise training modality on glucose tolerance in men with abnormal glucose regulation. Int J Sports Med 15:283–289
Van Etten LA, Westerterp KR, Verstappen FTJ, Boon BJB, Saris WHM (1997) Effect of an 18-wk weight-training program on energy expenditure and physical activity. J Appl Physiol 82:298–304
Whelton SP, Chin A, Xin X, He J (2002) Effect of aerobic exercise on blood pressure: a meta-analysis of randomized, controlled trials. Ann Intern Med 136:493–503
Wijndaele K, Beunen G, Duvigneaud N, Matton L, Duquet W, Thomis M et al (2006) A continuous metabolic syndrome risk score: utility for epidemiological analyses. Diabetes Care 29:2329
Wijndaele K, Duvigneaud N, Matton L, Duquet W, Delecluse C, Thomis M et al (2007) Sedentary behaviour, physical activity and a continuous metabolic syndrome risk score in adults. Eur J Clin Nutr 63:421–429
Wing RR, Jakicic JM, Neiberg R, Lang W, Blair SN, Cooper L et al (2007) Fitness, fatness, and cardiovascular risk factors in Type 2 diabetes: look AHEAD study. Med Sci Sports Exerc 39:2107–2116
Yeater R, Reed C, Ullrich I, Morise A, Borsch M (1996) Resistance trained athletes using or not using anabolic steroids compared to runners: effects on cardiorespiratory variables, body composition, and plasma lipids. Br J Sports Med 30:11–14
Acknowledgments
This research was supported by The American Heart Association (AHA 9951116Z).
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by Susan A. Ward.
Rights and permissions
About this article
Cite this article
Potteiger, J.A., Claytor, R.P., Hulver, M.W. et al. Resistance exercise and aerobic exercise when paired with dietary energy restriction both reduce the clinical components of metabolic syndrome in previously physically inactive males. Eur J Appl Physiol 112, 2035–2044 (2012). https://doi.org/10.1007/s00421-011-2174-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-011-2174-y