Article Text

Abstract
Objective—To improve understanding of processes leading to injury and assess more specifically the degree of intentionality.
Methods—A new paradigm was developed that characterizes the act of inflicting injury (self, other, not inflicted) and the motive. Motives are determined for the act of injury and for the outcome. To test this, 986 cases of adolescent injuries in seven hospitals were reviewed. Three investigators independently classified all cases using the new paradigm and three used standard definitions of intent. Inter-rater reliability was measured.
Results—Of injuries inflicted by others, 61% were intentional using the standard classification. In the new paradigm 67% were intended acts and 59% involved intentional motive for outcome. Altogether 87% of sports injuries were coded as unintentional acts compared with 96% using standard methods. Using standard classification there was 93% agreement between paired raters, with an average κ of 0.86. In the new paradigm questions on intentionality of act, outcome, and infliction of act, the agreement was 89%, 91%, 88%, with a κ of 0.79, 0.80, 0.76, respectively.
Conclusions—This paradigm defines a spectrum of injury intent, enhances understanding of the causal sequence of injury, and has important implications for research and prevention.
- intentionality
- violence
- injury coding
Statistics from Altmetric.com
Injury intent “identifies whether the injury occurred as a result of an inadvertent or a volitional act”.1 Intentional injury has been defined as “maltreatment...caused by an action or omission [meant] to cause harm to the victim”2 or “done deliberately”.3 Understanding the circumstances surrounding an injury event, and whether it involved intent, is crucial for designing interventions. Our study objectives were (1) to improve our understanding of the processes leading to injury by better classifying whether the injuries were inflicted; (2) to create a coding system to assess more specifically the degree of intentionality; and (3) to compare the determination of intent using this paradigm with currently used methods for coding intent.
E codes categorize cause of injury as intentional (self inflicted or assault/homicide), unintentional (accidental), or undetermined. There is a much greater degree of specificity of codes for unintentional injury compared with undetermined or intentional injuries. “Accidental” unintentional codes include 150 three digit categories (E800-949) while intentional codes include only 30 three digit categories (suicide and self inflicted injury, E950-959, homicide and injury purposely inflicted by other persons, E960-969, and injury resulting from operations of war, E990-999). (Undetermined intent includes 10 three digit categories, E980-989.)
For some injuries there exist specific unintentional codes, but no specific codes for the same injury if intentional or of unclear intent. For example, there are specific unintentional injury codes for sports injuries, but no specific codes for sports injuries involving intent or undetermined intent. Unintentional motor vehicle accidents include codes E810-825, with 16 different codes each with fourth digit subdivisions. It was not until the 1995 revision of International Classification of Diseases (ICD-9-CM) that intentional vehicular assault received a single code (E968.5). Unintentional injuries of being struck against or by objects or persons include five different codes but being struck with undetermined intent has no unique code. The most appropriate code would be “injury by other and unspecified means, undetermined whether accidentally or purposefully inflicted”, E988.8. In summary, in most instances, E codes are much more descriptive and useful for unintentional injuries than for injuries involving intentional or undetermined intent.
In addition, E code rules have changed over the years. Previously, if intent was unclear in morbidity coding, the default was to code as “accidental” or unintentional. Effective 1 October 1996, however, morbidity coding guidelines state that the undetermined category be used if intent is not known (“if the cause...is questionable, probable or suspected...”).4 Consequently, there may be misclassification in coding intentionality. The problem of misclassification and uneven specificity in E codes of unintentional, intentional, and undetermined causes makes the assessment of intent difficult.
Categorizing injuries as intentional or unintentional also has limitations because a single injury may involve several possible motives. Consider, for example, an injury resulting from getting elbowed while playing basketball. This injury involves two people and is inflicted by transfer of energy from one person to another. The injury may be completely unintentional. Alternatively, the other person may have intentionally thrown an elbow in anger, but it was not intended that the outcome result in a fractured jaw. Finally, the act and the outcome (the fractured jaw) may have both been intended. Understanding the difference among these circumstances can have importance for prevention. Protective gear may be an appropriate intervention for all three scenarios; however, the latter two scenarios might also involve interventions emphasizing rules and accepted behavior or conflict mediation. The current E code structure cannot differentiate these three scenarios.
The National Center for Health Statistics reports injury mortality as unintentional or intentional based on E codes. Some existing surveillance systems have classified morbidity as intentional or unintentional depending on the abstractor's judgment. Thus there are clear limitations to current categorization of intent. To more fully understand the processes resulting in injury, we developed a new paradigm of intentionality that recognizes its complexities and gradations.
Methods
The new paradigm assumes that the act of inflicting injury is separate from the motive for inflicting injury; and hypothesizes that: (1) intentional or unintentional motive may differ for the act of injury and for the outcome and (2) intentional motives in the act of inflicting injury may have a larger role in injury than currently described.
This paradigm characterizes the person or persons involved in the act. The injury may or may not be inflicted. If inflicted, it may be inflicted by self (the victim) or by other. An interpersonal inflicted act is defined as the active transfer of energy from one person to another. A self inflicted act is defined as the active transfer of energy from self to self where the victim was active in the act of injury and/or cognizant of a risk of injury. Intentional or unintentional motives are determined separately for the act of injury and the injury outcome. For example, in the case of an angry person punching the wall, the act of punching was intentional but the outcome (a boxer's fracture) presumably was not what was intended. The sequence of events leading to an act and resulting in an outcome demonstrate the possible points of primary, secondary, and tertiary prevention.
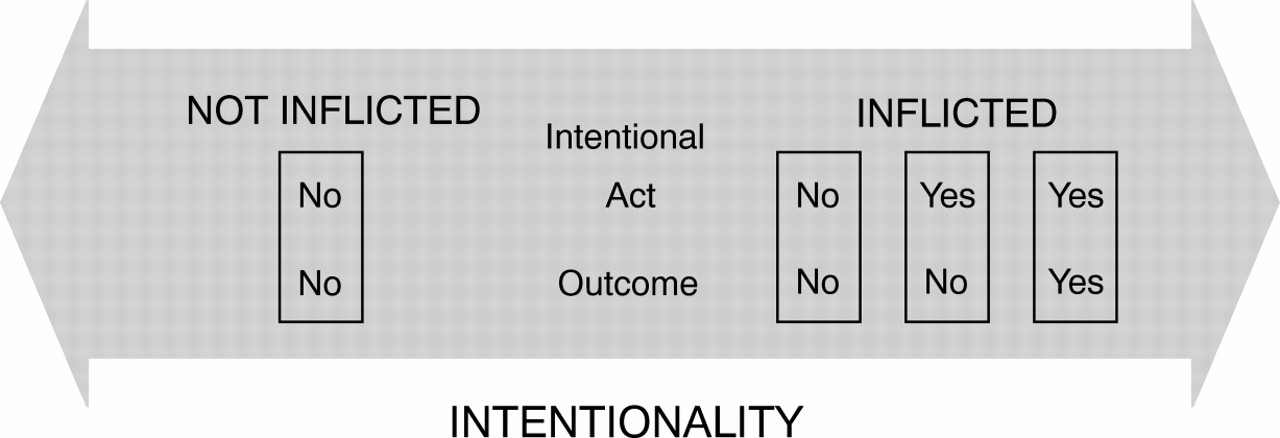
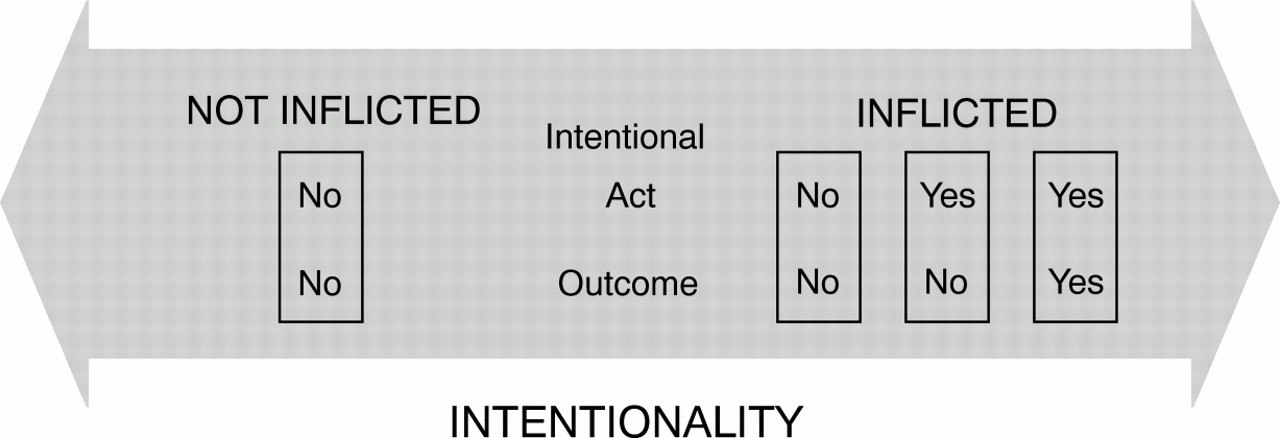
Our proposed model recognizes a spectrum of intentionality. It includes three characteristics of the injury; whether the act was inflicted and the person(s) involved, the motives leading to injury, and the motives for the outcome. The various configurations of these characteristics define the spectrum of intentionality (fig 1).
{kind=link}
Spectrum of intentionality.
Injuries not inflicted include “acts of God”, for example a branch falling on someone's head, and other single person “accidents” like falling or tripping. Inflicted injuries may be inflicted by self or other. Injury events inflicted by self could range from cutting oneself while slicing a bagel to a suicide attempt. The motives for the act and outcome differ in these two cases. Those inflicted by others would range from true “accidents” inflicted by another person, for example someone inadvertently tripping another person, to an assault. Again, motives for the act and outcome differ.
This new paradigm was assessed using cases in a surveillance study of adolescent injuries. We compared the properties of the new paradigm with conventional, dichotomous classifications of intent. We reviewed 986 consecutive emergency department injuries. The surveillance included injuries in 10–19 year olds from seven hospitals in the District of Columbia. It includes clinical data and all statements describing how the injury occurred abstracted from the medical record.
Three investigators independently classified all cases using the new paradigm and three others used conventional definitions of intent. Assignment of intentionality was based on descriptions of the injury and assumptions about probable events from the clinical data.
Initially we reviewed 500 cases and classified the intent. We then discussed differences in interpretations and developed a set of rules with examples to guide further classification using the new paradigm. Inter-rater reliability was measured.
Results
In the new paradigm, more injuries involved intentional motives for the act compared with the conventional classification. For example, in sports injuries, 87% were coded as unintentional acts compared with 96% using current methods. For instance, in a football injury where a child is “tackled”, the act of tackling is intentional though the outcome of a concussion may or may not be. In current dichotomous coding, that injury is considered unintentional.
Reviewing 986 injuries using the new paradigm definitions, 15% were inflicted by self, 48% inflicted by other, 35% not inflicted, and 2% undetermined. Trained investigator coding of all injuries using conventional dichotomy and the new paradigm are presented in table 1. Table 2 presents injuries inflicted by others.
Intentionality of injuries (n=986); values are %
Intentionality of injuries inflicted by other (n=398); values are %
Using current dichotomous coding definitions there was 93% agreement between paired raters with an average κ of 0.86. In the new paradigm, questions on intentionality of act, intentionality of outcome, and infliction of act, the agreement in the total sample was 89%, 91%, and 88%, respectively, with κ of 0.79, 0.80, 0.76. We coded 500 cases initially, reviewed discrepancies, and coded a second group of consecutive injury cases. Per cent agreement improved from 85%–89% to 91%–92%, with κ improvement from 0.67–0.77 to 0.82–0.84.
Discussion
This new paradigm begins to disentangle issues important in determining injury intent, and further describes important circumstances of injury. Certain limitations of the study and paradigm should be considered. First, use of chart information for description of the cause of injury is problematic. There may be incomplete reporting of events by the patient or incomplete questioning on the part of medical personnel. Incomplete documentation or illegible documentation is also common. Second, coding requires interpretation, which adds another layer of uncertainty. Finally, in some cases, the problem of ascertaining true motives in the act and outcome of an injury is difficult and requires some judgment. None the less, we feel it is important to understand the plausible and possible mechanisms of injury to guide interventions. All these limitations are present in any classification system and are not inherent problems of this paradigm. Further work will assess the validity of chart abstraction determination of intent by comparing chart abstraction determination to interviews with injury victims. We tested this paradigm with a sample of injuries among adolescents. It is likely that many injuries in youth, including exploratory acts in young children or risk taking behavior in adolescents, may involve deliberate, intentional acts with unintended harm. In situations of injury due to adult neglect, another level of coding intent of the supervisory adult may be needed.
Clearly, for a single injury there may be many scenarios involving a range of intent. The new paradigm dichotomizes injuries as inflicted or not inflicted (“acts of God”). Among inflicted injuries, there are essentially three possibilities including (1) unintentional act and outcome, (2) intentional act, unintentional outcome, and (3) intentional act and outcome. For instance, for firearm injuries there are several configurations for these inflicted injuries, and intent would differ depending on whether it was an assault, mistaken target, or true accidental firing (for instance during cleaning) (table 3). This paradigm goes beyond a simple dichotomization and describes various configurations of the three characteristics with six possible scenarios. Interventions may differ depending on these circumstances of injury.
Example: firearm injuries
We describe this paradigm and method of implementation to stimulate others in the injury prevention field to expand their thinking about the role of intentionality in the causation of injury. Classification and validation of intentionality are important if we are to truly understand the causes of injuries, which, in turn, is critical for the development of effective prevention strategies. Intentional motive may play a part in some injuries currently considered “unintentional”. This paradigm expands the definition of intentionality, recognizes a spectrum, and provides improved understanding of the causal sequence of injury.
Acknowledgments
We wish to thank Donna Pickett at the National Center for Health Statistics for her review of the manuscript. We also thank the emergency department collaborators in the DC Child/Adolescent Injury Research Network surveillance including Melissa Clarke, MD, Millicent Collins, MD, Duncan Harviel, MD, Yolanda Haywood, MD, David Milzmann, MD, Mark Smith, MD, and Jim Vafier, MD.
This project was supported by the Centers for Disease Control and Prevention and the Robert Wood Johnson Foundation Generalist Faculty Scholars Program (Dr Cheng). This paper was presented at the Pediatric Academic Societies meeting in Washington, DC, May 1997 and the Annual Meeting of the American Public Health Association in Indianapolis, November 1997.