Article Text

Abstract
Background Hamstring injuries are the most common muscle injury in male amateur soccer players and have a high rate of recurrence, often despite extensive treatment and long rehabilitation periods. Eccentric strength and flexibility are recognised as important modifiable risk factors, which have led to the development of eccentric hamstring exercises, such as the Nordic hamstring exercise. As the effectiveness of the Nordic hamstring exercise in reducing hamstring injuries has never been investigated in amateur soccer players, the aim of this study is to investigate the effect of this exercise on the incidence and severity of hamstring injuries in male amateur soccer players. An additional aim is to determine whether flexibility is associated with hamstring injuries.
Study design Cluster-randomised controlled trial with soccer teams as the unit of cluster.
Methods Dutch male amateur soccer players, aged 18–40 years, were allocated to an intervention or control group. Both study groups continued regular soccer training during 2013, but the intervention group additionally performed the Nordic hamstring exercise (25 sessions over 13 weeks). Primary outcomes are the incidence of initial and recurrent hamstring injury and injury severity. Secondary outcomes are hamstring-and-lower-back flexibility and compliance. Compliance to the intervention protocol was also monitored.
Discussion Eccentric hamstring strength exercises are hypothesised to reduce the incidence of hamstring injury among male amateur soccer players by 70%. The prevention of such injuries will be beneficial to soccer players, clubs, football associations, health insurance companies and society.
Trial Registration NTR3664.
Statistics from Altmetric.com
Background
Soccer is the most popular sport worldwide, with 275 million participants of either sex and of all ages.1 In general, sports participation generates a physically active lifestyle. However, the beneficial health effects of sport are tempered by the risk of injury.2 Unfortunately, soccer has a high injury rate, with male amateur soccer players being particularly prone to injury.3–7 Of all players, 60–100% sustain at least one injury per soccer season.8 ,9 In terms of incidence rates in amateur players, soccer leads to 21.9 injuries per 1000 match hours and to 3.4 injuries per 1000 training hours.3 ,7
Hamstring injuries, defined as any physical complaint affecting the posterior side of the upper leg irrespective of the need for medical attention or time loss from soccer activities,10 are the most common soccer-related muscle injury.11 ,12 They account for 13–17% of all soccer injuries and require extensive treatment and long rehabilitation periods, leading to absence from training and matches for up to 90 days.8 ,7 ,12 ,13 Hamstring injuries also have a high recurrent rate, varying from 12% to 33%.12–15
Of a number of potential risk factors for hamstring injuries, such as age, previous hamstring injury, muscle architecture, fatigue, flexibility, core stability and strength, flexibility and strength are considered important modifiable risk factors.16–18 Biomechanical analyses have shown that hamstring ruptures typically occur in the latter part of the swing phase during sprinting.19 ,20 Before the foot hits the ground, the hamstring is (sub)maximally stretched over the knee joint, but at the same time it has to counter isokinetic forces from the preswinging leg. The higher the sprinting velocity, the greater these forces are.19 ,20 The vulnerability of the hamstring to injury during this phase of sprinting is associated with inadequate eccentric strength of the hamstring.21–23
Exercises to increase eccentric muscle strength, such as the Nordic hamstring exercise or hamstring curl, have shown to reduce the rate of hamstring injury by 65–70%, and particularly recurrent injuries, in professional soccer players.24–26
Male amateur soccer players form the largest subgroup of soccer players worldwide, with the incidence of injury increasing with higher levels of play.3 ,4 Strategies to prevent hamstring injuries, such as the Nordic hamstring exercise, may reduce the incidence of hamstring injury, medical costs and personal suffering of the injured player.27–29
The aims of this study are to investigate the preventive effect of the Nordic hamstring exercise on the incidence and severity of hamstring injuries in male amateur soccer players and to establish whether flexibility is associated with an increased risk of hamstring injury.
Methods/design
Design and randomisation
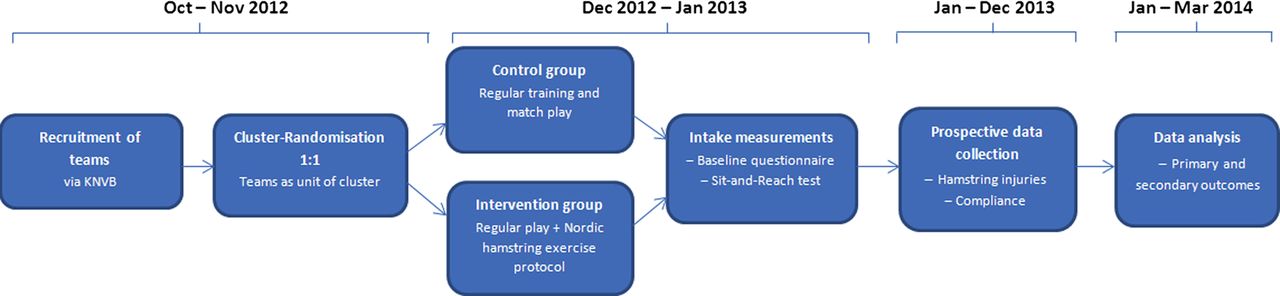
This prospective, cluster-randomised, parallel group trial was designed in accordance with the consolidate standards of reporting trials (CONSORT) guidelines (figure 1).30 Soccer teams were used as the unit of cluster to avoid the risk of bias if individuals were randomised to the intervention programme.31 After computer-generated random assignment of team numbers, an equal number of teams were randomised to the control or intervention group by an online research randomizer (http://www.randomizer.org).

Consolidate standards of reporting trials (CONSORT) flow diagram of trial design.
Study setting
This trial is being carried out in collaboration with the Royal Netherlands Football Association (KNVB). Soccer teams from four separate districts playing in Dutch first-class (‘Eerste Klasse’) amateur field soccer competition were invited to participate. These teams generally play one or two matches a week, with two or three training sessions per week. After the four districts had been selected, instruction meetings, to inform the purpose and methods of the study, were held for the coaches and medical staff of participating teams, organised by the research team in each district.
Eligibility criteria
Dutch male amateur soccer players, aged 18–40 years, were eligible for inclusion. Players who joined a participating team after the start of the trial were not included. All players were asked to give their informed consent before the start of this study. Players unwilling to do so were excluded from the trial.
Intervention
The ‘Nordic hamstring exercise’, in literature also referred to as the Nordic curl, improves the eccentric strength of the hamstring muscles. The exercise is performed in pairs (see figure 2).24

The Nordic hamstring exercise (adapted from Petersen et al[24]).
{}
Players start in a kneeling position, with the torso from the knees upward held rigid and straight. The training partner ensures that the player's feet are in contact with the ground throughout the exercise by applying pressure to the player's heels/lower legs. The player then lowers his upper body to the ground as slowly as possible to maximise loading in the eccentric phase. Hands and arms are used to break his forward fall and to push him back up after the chest has touched the ground to minimise loading in the concentric phase.32 The exercise was supervised by the team coach or medical staff and took place immediately after the completion of normal training as recommended by Small et al,33 before cooling down.
After the winter break in the 2012–2013 season (last 2 weeks in December), all teams started their normal training schedule about 3–5 weeks before the competition restarted (the season typically runs from July to May), which is typical for elite amateur soccer competition in Western Europe. The intervention (see table 1) started at the beginning of this training schedule, with a constructive phase (weeks 1–5) and a maintenance phase (weeks 6–13).24 ,25
Nordic hamstring exercise protocol
Players in the intervention group were instructed to perform 25 sessions of the Nordic hamstring exercise during the first 13 weeks after the winter break. Players were told about the possibility of Delayed Onset of Muscle Soreness (DOMS), a known side effect of eccentric exercises.32 Players who were injured at the beginning of the intervention could start the protocol week 1 after full recovery. Players who sustained an injury during the intervention period, which limited the execution of the Nordic hamstring exercise, were instructed to contact the research team.
Data collection
Baseline characteristics
Prior to the start of the intervention, all players completed a questionnaire to record baseline characteristics: date of birth, weight, height, nationality, years of experience as a soccer player, leg dominance, field position, preventive measures taken (such as inlays, taping, bandages, thermal pants, muscle strengthening exercises or stretching) and other injuries incurred before the start of the study (in particular, hamstring injuries and anterior cruciate ligament injuries).
Hamstring injuries
The medical staff of participating teams (eg, physical therapists and/or sports masseurs) are responsible for registering all hamstring injuries for a full calendar year (2013). A hamstring injury is defined as any physical complaint affecting the posterior side of the upper leg irrespective of the need for medical attention or time loss from soccer activities.10 A recurrent hamstring injury is defined as an injury of the same type and at the same site as an index injury and which occurs after a player's return to full participation from the index injury.10 Recurrent injuries are subdivided into ‘early recurrences’ within 2 months after a player's return to full participation, ‘late recurrences’ between 2 and 12 months after a player's return to full participation and ‘delayed recurrences’ more than 12 months after a player's return to full participation.10 All hamstring injuries are registered on a special form, and a so-called recovery form is completed when the player is fully recovered. Data are being collected on the epidemiology (location, type and duration of the injury) and aetiology (including intrinsic and extrinsic factors, such as injury history and field condition) of the hamstring injury and information on residual complaints and tertiary prevention.
Hamstring-and-lower-back flexibility
Hamstring-and-lower-back flexibility (HLBF) was measured in all players at the start of the study, using the Sit-and-Reach test (SRT)34–37 (see figure 3).

{kind=link}
{kind=link}
{kind=link}
Sit-and-Reach test.
The medical staff was instructed how to perform the SRT procedure at the soccer club. Participants were not allowed to warm up before doing the SRT. A player is asked to sit on the floor, with the legs together, the knees extended, the ankles in 90° dorsiflexion and the soles of the bare feet placed against the foot panel of the test box. Then, the player is asked to place his hands on top of each other with the hand palms facing downward, and to slowly reach forward as far as possible, moving a reach indicator along the measuring scale on the box and to hold the maximum stretch for 2 s. The test supervisor ensures that the player's knees, arms and fingers remain extended throughout the test. Both knees should be locked during the test. Measurements are repeated twice, with a 15 s interval, during which the player is allowed to sit up straight, but not to stand up or stretch. SRT scores were recorded to the nearest 0.5 cm. HLBF was not measured in players who were unable to perform the SRT as instructed (eg, because of limited knee extension after injury).
Exposure and compliance
The number of times a player performed the Nordic hamstring exercise protocol (intervention group), the number and duration (in minutes) of training sessions (both group and individual training) followed and the number and duration (in minutes) of matches played are recorded weekly for 1 year by the team coach, using a computer-based registration form. Match exposure is defined as play between teams from different clubs.10 Training exposure is defined as team-based and individual physical activities under the control or guidance of the team's coaching or fitness staff that are aimed at maintaining or improving players’ soccer skills or physical condition.10 Coaches will also record reasons why players do not attend training or matches (eg, sickness, injury, hamstring injury, individual training, training elsewhere or other) per individual player.
The research team will remain in contact weekly (by telephone, email or visits) with team coaches and players having a view to encouraging compliance with data registration. In addition, newsletters, evaluation meetings and a website designed for this specific study will be used to stimulate participation and compliance.
The intervention teams will be monitored with regard to implementation and performance of the Nordic hamstring exercise and other self-initiated preventive strategies for hamstring injuries (eg, core stability and plyometric exercises) and the control teams will be monitored with regard to self-initiated preventive measures for hamstring injuries, specifically the Nordic hamstring exercise.
Outcomes
Primary outcomes are the incidence of initial and recurrent hamstring injuries, the severity of the injury and the number of intervention sessions completed. Secondary outcomes are HLBF and compliance. Data will be collected from all participants. The incidence of injuries is reported as the number of injuries per 1000 player-hours for both matches and training.10 Injury severity is defined as the number of days that have elapsed from the date of injury to the date of the player's return to full participation in team training and availability for match selection.10
Sample size
On the basis of the literature, we expected that the intervention would lead to a 70% reduction in the rate of hamstring injury compared with control.24 During a soccer season, about one in 11 players has a hamstring injury with a 30% chance of recurrent hamstring injury.24 With two-sided testing, a significance level of 0.05 and power of 0.8, each study group should include 175 players. With a clustered design, an inflation factor (intracluster correlation coefficient=0.05) of 1.9 was applied to the sample size, and with an estimated dropout rate of 7%8 ,24 we calculated that 712 players would need to be recruited (n=356 for intervention group and n=356 for control group). Since first-class amateur teams consist of about 19 players, a total of 38 teams was considered sufficient.
Statistical methods
SPSS V.21.0 will be used to analyse the quantitative data. Descriptive statistics (means and SD) will be used to describe baseline characteristics and exposure data. The incidence of initial and recurrent hamstring injuries will be analysed on an intention-to-treat basis.
T tests and Mann–Whitney U tests will be used for continuous variables and χ2 tests for categorical variables. Poisson general log-linear analysis and Cox hazards regression with survival curves will be used to compare the intervention and control groups.
Compliance with the intervention will be calculated on the basis of information provided by the team coaches. As the protocol consists of 25 sessions, compliance will be calculated per team as: nh (amount of Nordic hamstring exercise sessions)/25 × 100=% compliance. Additional analysis will be performed to check whether certain variables are related to missing data or dropout.
Ethical approval and informed consent
This trial was approved by the medical ethics committee of the University Medical Center Utrecht (File number 12-575/C). Where applicable, important modifications will be communicated with the same ethics committee that provided approval. The trial was registered in the Dutch Trial Register (NTR3664) as the Hamstring Injury Prevention Strategies (HIPS) study. All participants receive brief and comprehensible oral and written information in accordance with the Helsinki Declaration.38 Informed, written consent is obtained from all participants by one of the researchers (NvdH) before baseline tests. Personal information about enrolled participants will be used confidentially before, during and after the trial.
Discussion
Hamstring injuries in amateur soccer can lead to medical costs, work absenteeism, reduced performance and personal suffering.27 The Nordic hamstring exercise has been shown to substantially reduce the incidence of hamstring among professional soccer players.24–26 However, because there are differences in medical staff, level of play, training frequency, training intensity and compliance to preventive measures between professional and amateur soccer players, the data for professional players cannot necessarily be extrapolated to amateur players. Even so, it would be worthwhile to reduce the incidence of such injuries among amateur players. Not only for the players themselves, but also for society, health insurance companies, football associations and football clubs. Eccentric strength training may be an effective way to prevent these injuries, to benefit of all concerned (more matches played, reduced absenteeism and medical costs). This study has the advantage of a large study population (2×19 teams), and the use of terminology and methodology consistent with the consensus statement on injury definitions in soccer will generate data that can be compared with those of other studies.10 Data modification and data loss are limited by the use of specially designed, computer-based registration forms for team coaches and medical staff.
Trial status
Participants were recruited in October–November 2012 and were randomised to the intervention and control groups in December 2012. The intervention started in January 2013. Data collection is in progress and will be completed in January 2014. Data analyses are expected to be completed in May 2014.
Acknowledgments
The authors thank the Royal Netherlands Football Association (KNVB) and players, coaches, medical staff members and other representatives of participating clubs for their contributions during the trial.
References
Footnotes
-
Contributors Nick van der Horst, Dirk-Wouter Smits and Frank Backx made a direct and substantial contribution to the design and development of the trial protocol and were mainly responsible for writing the manuscript. Jesper Petersen contributed substantially to the development of the intervention. All authors had a substantial input in the draft manuscript, and all have read and approved the final version of the manuscript.
-
Funding This study is funded with grants from the Netherlands Organisation for Health Research and Development (Dnr: 75020024) and the Royal Netherlands Football Association (KNVB).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The medical ethics committee of the University Medical Center Utrecht (File number 12-575/C).
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Data sharing statement If required, we are willing to share data, including relevant analyses, to any reviewers.