Article Text

Abstract
Aims: To study the mechanism and the means of preventing soccer eye injuries.
Methods: Kicked soccer ball velocities were measured for a range of ages and experience. Soccer balls (sizes 3, 4, and 5), inflated to 3, 6, and 9 psi, were impacted onto an artificial orbit and the results analysed at 1000 frames per second. Protective eyewear was fitted to a headform then impacted and evaluated.
Results: The mean peak ball velocity was 20.4 (SD 6.2) m/s. Soccer balls at 18 m/s entered the orbit between 7.5 and 8.7 mm. There was no significant difference in orbital penetration as a result of ball size or pressure. The soccer ball stayed in the orbit approximately 10 ms and appeared to have a suction effect as it withdrew. Protective eyewear that complied with sports protective eyewear standard ASTM F803 prevented contact of the ball to the eye.
Conclusions: The soccer ball causes eye injury by entering the orbit. Protectors that pass ASTM F803 would prevent orbital intrusion.
- soccer
- trauma
- protective eyewear
Statistics from Altmetric.com
Despite the fact that soccer is a common cause of serious sports eye injury, usually from the kicked ball, little is known of the mechanism by which the ball causes eye injury and the efficacy of eye protection.1–3 This study was done to determine the velocity of the kicked soccer ball for various ages and levels of experience, determine the mechanism of soccer ball induced eye injuries and whether ball size and inflation are important risk factors, and evaluate the effectiveness of existing eye protectors.
PATIENTS AND METHODS
Fifty four male Portuguese soccer players (nine indoor professional, 12 outdoor amateur, 21 outdoor professional, 12 young professional) each kicked a soccer ball once from the penalty mark. In addition, 165 Massachusetts players (64 female, 101 male) ages 5–53 (31 ages 5–9, 46 ages 10–13, 81 ages 14–18, seven ages 25–53) each kicked an age appropriate soccer ball once from the penalty mark. Velocities were measured with a sports radar gun positioned on a tripod behind the goal net.
An air cannon4 was used to propel number 3, 4, and 5 soccer balls, and other sports balls, at an artificial orbit.5 Because the soccer ball wrapped around the anterior surface of the orbit, a 30 cm square 3 mm steel plate was affixed around the orbital periphery to permit photography at 1000 frames per second.
Nine models of eyewear, advertised for sports use, were placed on a Canadian Standards Association headform that corresponded to the head size of an adult woman and a 13 year old young man. Two of the models passed the ASTM F803 sports protective eyewear standard for racquetball, squash, and women’s lacrosse, three models passed ASTM F8036 for racquetball and squash, four models failed ASTM F803 but passed the US industrial protective eyewear standard ANSI Z87.7 Marking paste, to indicate contact of the protector to the eye, was applied to the eye of the headform. The eyewear was impacted with a number 5 soccer ball at 17.7 (SD 0.9) m/s (40 mph).
RESULTS
Ball velocities measurements
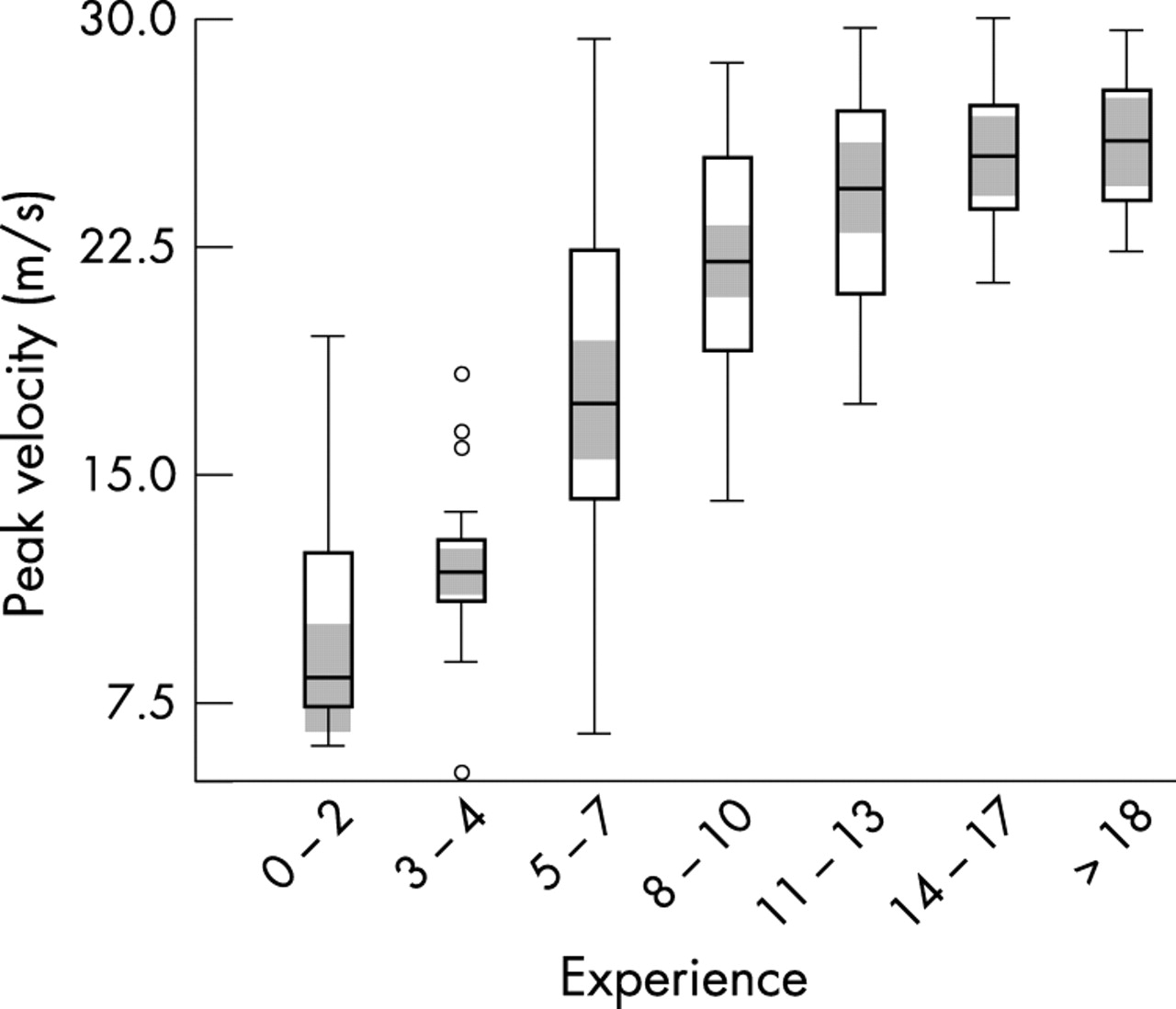
Portuguese players kicked the ball at a mean velocity of 26.2 m/s (58.6 mph) with the outdoor professionals exceeding the velocities of the indoor professionals and the outdoor amateurs. The amateur players from Massachusetts averaged a peak velocity of 18.5 m/s (41.4 mph) with players in the 10–18 age groups having higher velocities than the others. There was better correlation of ball velocity with experience than with age (fig 1).

Soccer ball peak velocity by years of experience.
Artificial orbit
Soccer balls (fig 2) penetrated into the orbit between 7.5 and 8.7 mm. There was no significant difference in penetration by the smaller diameter soccer balls, nor did under-inflation result in any significant increase in orbital penetration. The penetration was significantly less with soccer balls than with tennis balls (18.6 mm at 90 mph), racquetballs (16.1 mm at 90 mph), and lacrosse balls (20.0 mm at 54 mph); however, the soccer balls remained in contact with the interior of the orbit far longer (8.7–11.0 ms) than tennis, racquetball, and lacrosse balls (3–4 ms).

Soccer ball impact onto artificial orbit. The orbit (anterior plane, small arrow) is penetrated 8.1 mm by the 18 m/s (40 mph) size 3 soccer ball, which compresses on the steel plate surrounding the orbital fixture (large arrow). The compression phase of the ball, that drives a small knuckle of the ball into the orbit (1–4 ms), is easily seen by studying the dark triangles on the ball. During rebound, the slow orbital exit of the ball compared to the rebound from the plate (5–10 ms) produces a secondary suction effect on the orbital contents.
Eyewear
All of the eyewear that passed the ASTM F803 sports protective eyewear standard for racquetball and squash prevented eye contact. None of the eyewear that failed ASTM F803 but passed ANSI Z87 prevented eye contact by the protector lens bottoming out on the eye of the headform. None of the polycarbonate lenses in any of the protective eyewear shattered. The ball deformed significantly and moulded to facial contours (fig 3).

{kind=link}
{kind=link}
{kind=link}
Impact of size 5 ball at 17.7 m/s (40 mph) on headform with protective eyewear that passes ASTM F803 for racket sports and women’s lacrosse. No eye contact.
DISCUSSION
Since there is not enough energy from heading to cause retinal haemorrhages,8 it is almost certain that the soccer ball must directly impact the eye to cause a retinal tear or other significant eye injury. When the soccer ball hits the eye (especially in younger players where the orbital rims are less developed) more energy is directly transmitted to the exposed temporal retina while the nose protects the nasal retina. A suction component9 most likely adds to the distortion of the globe anatomy that causes stresses resulting in tearing of structures in the anterior and posterior segments of the eye.
The force delivered by the portion of the soccer ball that enters the orbit is only a small fraction of that contained in the entire ball. A large amount of the ball’s energy is absorbed by the face and the portion that enters the orbit is spread out over approximately 10 ms. That there were no open globe injuries implies that the peak force and force onset rate are less from a kicked soccer ball than from a standard major league baseball at 23.2 m/s (55 mph).5 The balls that cause open globe injuries are either hard and transmit energy quickly (golf, baseball) or penetrate into the orbit very deeply (squash). When compared to other sports balls, the soccer ball penetrates less but remains in the orbital space 2.5–10 times as long. Hard balls (field hockey, baseball, softball, polo, golf) rebound in a fifth to a tenth of the time of the soccer ball.
Even though the incidence of an eye injury to any given player in one soccer game is quite small, the large number of worldwide soccer players makes this relatively small risk to a given individual an injury occurrence problem for society. Reducing the number of injuries by encouraging players to use readily available protective eyewear that conforms to ASTM F803 would be in the best interests of public health.
Acknowledgments
This study was partially funded by the Massachusetts Lions Eye Research Fund.