Article Text

Abstract
Objective First, to look for appropriate closed kinetic chain exercises to restore intramuscular imbalance between upper trapezius (UT) and serratus anterior (SA) in overhead athletes. Second, to determine the influence of using diagonal pattern muscle recruitment during knee push up plus (KPP) exercises on scapular electromyographic activity.
Design Single group repeated-measures design.
Setting Controlled laboratory study.
Participants Thirty-two physically active individuals in good general health who did not have a history of neck and/or shoulder injury or surgery nor participated in high-level overhead sports or performed upper limb strength training for more than 5 h/week.
Interventions Subjects performed the standard KPP and six variations.
Main outcome measurements Electromyographic activity of the three trapezius parts and the SA.
Results Four exercises with a low UT/SA can be selected for rehabilitation of intramuscular balance: standard KPP, KPP with homolateral leg extension, KPP with a wobble board and homolateral leg extension and one-handed KPP. The use of a wobble board during KPP exercises and performance on one hand has no influence on SA electromyographic activity.
Heterolateral leg extension during KPP stimulates lower trapezius activity, whereas homolateral leg extension stimulates SA activity.
Conclusions In case of intramuscular scapular imbalance, some exercises are preferable over others because of their low UT/SA ratio. The use of a kinetic chain approach during KPP exercises influences scapular muscle activity.
Statistics from Altmetric.com
Complexity of shoulder biomechanics is expressed in the high prevalence of shoulder injuries in overhead athletes.1 2 Recently, the role of the scapula in the pathogenesis of shoulder injuries has been given increasing interest.3,–,5 Scapular dyskinesis has been associated with subacromial and internal impingement.6,–,11 To regain a stable base for the humerus and allow for optimal throwing motion, scapular muscle training is an essential part in rehabilitation of overhead athletes.4 12 13
The serratus anterior muscle (SA) is considered to be an important stabiliser of the scapula.14 Provided cooperation with lower trapezius (LT), SA is optimally positioned to keep the scapula aligned with the thorax and ensure dynamic stabilisation. Weakness of SA is often present in overhead athletes with secondary impingement syndrome.15,–,17 Furthermore, intramuscular imbalance between SA and upper trapezius (UT) has been described.8 The challenge is to find exercises that specifically target the weak SA and minimally activate UT. In a study of Ludewig et al,18 electromyographic (EMG) activity of SA and UT was measured during the standard push up plus exercise (SPP) and modifications. SPP and knee push up plus (KPP) revealed highest SA activity and lowest UT/SA ratios and are therefore recommended for selective SA strengthening.
Closed kinetic chain exercises have been shown to stimulate mechanoreceptors, which contribute to shoulder joint stabilisation.4 19,–,21 This stimulus is suggested to be enlarged by adding an unstable base, possibly resulting in higher EMG activity.22,–,24 However, no differences with respect to SA activity were found so far in push-up exercises performed on a mini-trampoline or a Swiss ball.25,–,28
Another push-up modification that possibly increases SA activity is performing the exercise on one hand. An EMG analysis by Uhl et al showed very high activity of the posterior deltoid and infraspinatus during one-handed KPP.29 However, they did not analyse SA muscle activity.
In overhead athlete rehabilitation, a recent trend is the kinetic chain approach, which tends to incorporate other body segments in shoulder exercises.30 During a throwing motion, the body works as a dynamic unit and uses lower limbs and trunk to aim for the highest force and velocity at the hand of the throwing arm.31 Myofascial connections exist, by which lower limb muscle activity might influence scapular muscle activity. When the leg is extended, contraction of the gluteus maximus muscle tightens the thoracolumbar fascia. The stress of the thoracolumbar fascia is transmitted to the heterolateral scapula.32 33 The influence of leg extension on scapular muscle activity during push-up exercises has not yet been investigated.
The first purpose of this study is to look for appropriate exercises to restore intramuscular imbalance between UT and SA and therefore show high SA activity with low UT/SA ratio. More specifically, we wanted to investigate the influence of changing three aspects to the KPP on SA EMG activity and UT/SA ratio, namely, the addition of a wobble board, performance on one hand and extension of the homolateral or heterolateral leg.
Second, we wanted to investigate the influence of using diagonal pattern muscle recruitment during KPP exercises on scapular EMG activity of the three trapezius parts and SA.
Materials and methods
Subjects
Thirty-two physiotherapy students (16 men, 16 women) volunteered for this study. They were recruited at the department of Rehabilitation Sciences and Physiotherapy (Ghent University). Mean age was 22.88 years (2.43 years), mean height 1.73 m (0.09 m), mean weight 65.59 kg (8.14 kg), and mean body mass index was 21.95 (±1.84). All participants were physically active, in good general health, without history of neck and/or shoulder injury or surgery. They did not participate in high-level overhead sports nor performed upper limb strength training for more than 5 h/week. All subjects gave informed consent. The Ethical Committee of Ghent University Hospital (Ghent, Belgium) approved the investigation.
Instrumentation
For registration of EMG activity of the three trapezius parts and SA, a Noraxon Myosystem 1400 electromyographic receiver (Noraxon USA, Inc., Scottsdale, Arizona, USA) was used. Sampling rate for data collection was 1000 Hz (bandwidth of 10–1000 Hz). The device had a common mode rejection ratio of 115 dB. Gain was set at 1000 (signal-to-noise ratio <1 µV root mean square (RMS).
Skin surface was shaved and cleaned to reduce skin impedance (<10 kΩ). In all participants, the dominant side was tested. Bipolar Ag-Cl surface electrodes (Blue sensor; Medicotest, Ballerup, Denmark) were placed over UT, middle trapezius (MT), LT and SA. SENIAM (Surface ElectroMyoGraphy for the Non-Invasive Assessment of Muscles) recommendations were followed for electrode placement and interelectrode distance.34 Electrodes for UT were placed halfway between the spinous process of C7 and the posterior acromion. For registration of MT activity, electrodes were placed halfway on the horizontal line between the thoracic spine and the root of the scapular spine. Electrodes for registration of LT activity were placed obliquely upward and laterally along a line between the intersection of the scapular spine with the vertebral border of the scapula and the seventh thoracic spinous process.12 35,–,38 Electrodes for SA registration were applied anterior to the latissimus dorsi and posterior to the pectoralis major.18 26 39 A reference electrode was placed on the sternal part of the homolateral clavicle.
Correct electrode placement was checked and the signal was calibrated.
Testing procedure
In the first part of the investigation, maximal voluntary isometric contractions (MVIC) of UT, MT, LT and SA were quantified for normalisation.12 38 40 MVIC of UT was measured during resisted isometric abduction. Participants were seated with the arm elevated 90°.41 To determine MVIC of MT, participants were lying prone with their dominant arm abducted 90° and externally rotated. In this position, resistance was applied to further horizontal abduction. For measurement of MVIC of LT, participants were lying prone with their dominant arm abducted so that the arm was in line with the muscle fibres. Resistance was applied to further horizontal abduction. MVIC of SA was quantified with the participants sitting with their arm flexed forward 130°. Resistance was applied to further elevation. Three repetitions of 5 s were performed with 5 s rest between contractions. This was controlled by a metronome (60 beeps/min). One investigator verbally encouraged the participants. Between MVIC measurements of different muscles, 2 min of rest was provided. This procedure has been used in other EMG studies and has proven useful.12 18 26
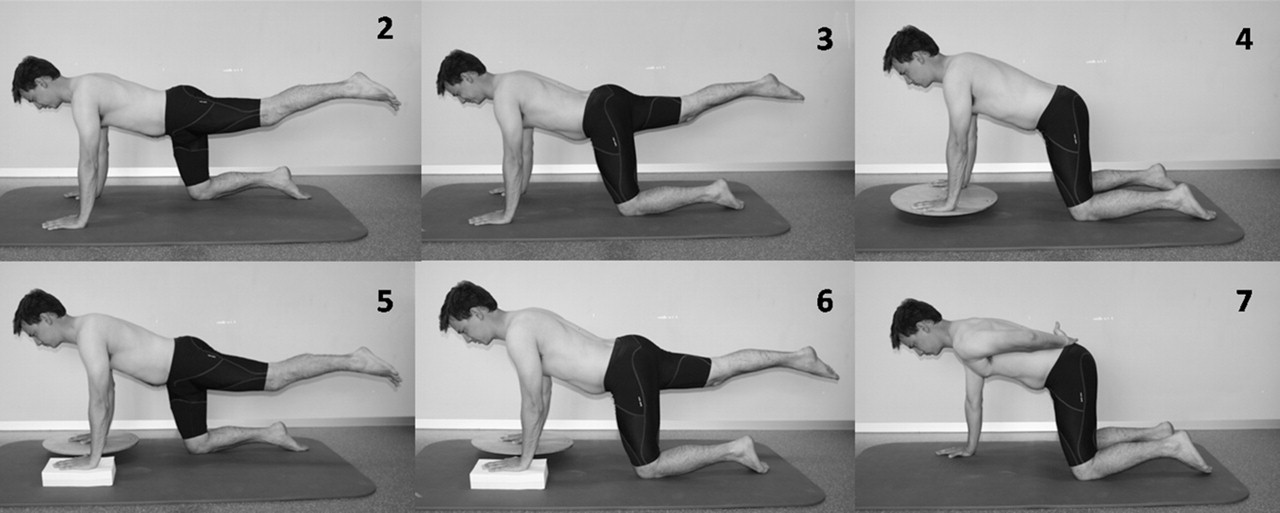
In the second part of the investigation, participants performed standard KPP (fig 1) and six variations (fig 2). Sequence was randomised to avoid influence of learning or fatigue and prevent order biasing. A metronome was used to control speed of performance (60 beeps/min). Participants completed five repetitions of each exercise with 5 s of rest in between. Between two different exercises, there was a resting period of 2 min.

Exercise 1, standard knee push up plus.

{kind=link}
{kind=link}
Exercise 2: knee push up plus (KPP) with heterolateral leg extension. Exercise 3: KPP with homolateral leg extension. Exercise 4: KPP with a wobble board. Exercise 5: KPP with heterolateral leg extension and a wobble board. Exercise 6: KPP with homolateral leg extension and a wobble board. Exercise 7: one-handed KPP.
Signal processing and data analysis
Myoresearch 98 Software Program was used for signal processing. Raw EMG signals were converted analog/digital (12-bit resolution) at 1000 Hz. The digital signals were full wave rectified and low-pass filtered (single pass, Butterworth, 6 Hz low-pass filter of the sixth order). Resting EMG activity was considered baseline activity. The three intermediate seconds of every repetition of MVIC were used for further analysis. EMG signals of the first and last repetition of the exercises were not accounted for.
For all subjects, MVIC was averaged across the three intermediate seconds for each muscle. Mean EMG activity of each muscle was calculated across the three intermediate repetitions of every exercise, for all subjects. Those values were subsequently normalised and thus expressed as a percentage of MVIC.
Statistical analysis
SPSS V.15.0 for Windows (SPSS Science, Chicago, Illinois, USA) was used for statistical analysis. Means and SD were calculated across subjects for normalised UT, MT, LT and SA EMG activity of each exercise (table 1).
Mean normalised EMG activity of scapular muscles during seven KPP exercises (% of maximal voluntary isometric contraction)
Ratios were calculated by dividing normalised EMG activity of UT by normalised EMG activity of SA for UT/SA ratio. Means and SD for UT/SA ratio were calculated (table 2). Ratios higher than 1 are not desirable because this implies UT activity is higher than SA. Ratios lower than 1 suggest lower relative UT activity and therefore indicate an exercise is appropriate for restoring muscular balance.
UT/MT, UT/LT and UT/SA
A Kolmogorov–Smirnov test showed normal distribution of the data. First, we wanted to detect differences in normalised EMG activity of UT, LT, MT and SA between the exercises. An analysis of variance (ANOVA) for repeated measures was performed for each muscle with “exercise” as a within-subjects factor (seven levels).
Second, we were interested in finding differences in UT/SA ratios between the exercises. Therefore, ANOVA for repeated measures was performed with exercise as a within-subjects factor (seven levels). In case of significance of Mauchly's test of sphericity, Greenhouse–Geisser correction was performed. The α level for ANOVA was set at 0.05. Post hoc analysis was done with Bonferroni correction for multiple comparison.
Results
Intramuscular balance UT/SA
UT/SA ratios (table 2) were very advantageous in general. As to mean UT/SA ratios, clinically relevant and statistically significant differences were found (F=15.119; p<0.01). Exercise 3 shows the lowest UT/SA ratio of all exercises and is significantly different from UT/SA in exercises 1 (p=0.001), 2 (p=0.005), 5 (p<0.001) and 6 (p<0.001). Thus, extension of the homolateral leg during KPP lowers the UT/SA ratio. Furthermore, UT/SA ratio in exercise 6 (0.54 (0.30)) is significantly lower than UT/SA in exercise 5 (p=0.002). This supports the positive influence on UT/SA ratio of homolateral leg extension. UT/SA ratios in exercise 2 (p=0.03) and in exercise 5 (p=0.002) were significantly higher than in the first exercise (KPP). Therefore we can conclude extension of the heterolateral leg results in a higher UT/SA ratio.
UT/SA in exercise 2 is significantly lower than UT/SA in exercise 5 (p=0.017), and UT/SA in exercise 3 is significantly lower than UT/SA in exercise 6 (p<0.01). Apparently, addition of a wobble board results in an increase of UT/SA. Finally, UT/SA ratio in exercise 7 is not significantly different from UT/SA in exercise 1. One-hand support does not change UT/SA ratio in comparison with standard KPP.
SA EMG activity
Statistical analysis showed significant differences in SA activity (table 1) between the exercises (F=59.048; p<0.001). When the homolateral leg is extended (exercise 3), SA activity is significantly higher than in all other exercises (p<0.001).
SA activity in exercise 2 is significantly lower than in exercises 1 (p=0.001), 6 (p=0.004) and 7 (p<0.001). SA activity in exercise 5 is significantly lower than in all other exercises (all p<0.001). Thus, heterolateral leg extension generates a lower mean SA EMG activity.
SA activity in exercise 6 is significantly lower than SA activity in exercise 3 (p<0.001), which implies that adding a wobble board lowers SA activity. This phenomenon is also obvious when comparing SA activity in exercise 5 with that in exercise 2 (p<0.001) and when comparing SA activity in exercise 4 and exercise 1 (p<0.001). There is no significant difference in SA activity between exercises 7 and 1, which indicates performing a KPP on one hand has no influence on SA activity.
UT, MT and LT EMG activity
When considering mean normalised EMG activity of UT, MT and LT (table 1), values are overall very low during KPP and variations. We compared trapezius EMG activity in exercise 2 with that in exercise 1 and trapezius EMG activity in exercise 5 with that in exercise 4 because these exercises only differ in the extension of the heterolateral leg. To clear out the influence of homolateral leg extension, we compared exercise 3 to 1 and exercise 6 to 4.
LT mean normalised EMG activity shows consistent significant differences (F=25.795; p<0.001). Both exercises during which the heterolateral leg was extended show a significantly higher LT activity than all other exercises. LT activity in exercise 2 is significantly higher than LT in exercises 1 (p<0.001) and LT activity in exercise 5 is significantly higher than LT in exercise 4 (p<0.001).
There is no significant difference in LT activity when the homolateral leg is extended. With regard to UT and MT mean normalised EMG activity, significant differences were present, but none of them were useful to answer our research questions. There was no pattern present in the results for EMG activity of the upper two trapezius parts.
Discussion
From a clinical point of view, it is especially of interest which exercises are appropriate for restoration of scapular muscle balance in overhead athletes. Four exercises, showing low UT/SA ratio, can be selected, namely, standard KPP, KPP with homolateral leg extension, KPP on a wobble board with homolateral leg extension and one-handed KPP. KPP with extension of the homolateral leg shows the lowest UT/SA ratio with highest mean SA activity (44.20%). These closed kinetic chain exercises should be used in the early stages of scapular strength training.42 43 Once a stable scapular base is achieved, shoulder rehabilitation should gradually progress towards functional open chain exercises.
To investigate more specifically the effect of an unstable surface on SA muscle activity, we compared exercises 2 and 5, 3 and 6, and 1 and 4 because the presence of a wobble board is the only difference between them. SA activity decreased by adding a wobble board. This is possibly due to the higher position of the hands, placing more weight on lower and less on upper extremities. Lehman et al found similar results. They showed SA activity increases when more weight is placed on the upper extremities by elevating the feet during SPP.27 Further research should investigate if eliminating height difference in upper and lower extremity support or adding an unstable base at lower extremity support results in higher SA EMG activity. However, we should be aware of the possibility that the use of an unstable surface influences other aspects of motor control, such as muscle timing or recruitment patterns, rather than muscle activity itself.
To answer the question whether SA muscle activity changes when KPP is performed on one hand, we compared exercises 1 and 7. Our results showed no significant differences, which indicates that SA muscle activity is not influenced by performance on one hand. Other muscles than SA probably provide the additional stabilising muscle activity needed.
The second objective of this study was to identify the influence of leg extension on scapular EMG activity. Many clinicians use the principle of the kinetic chain in athlete shoulder rehabilitation, mostly by extending the heterolateral leg to increase scapular activity in a diagonal pattern, but there has never been any investigation to confirm this approach. To answer this question, we compared scapular muscle activity during exercise 1 and exercises 2 and 5. When extending the heterolateral leg, LT activity increases and SA activity decreases. Myofascial connections, as described by Meyers et al and Porterfield and DeRosa, can provide a possible explanation for these results.32 33 Extension of the heterolateral leg generates gluteus maximus activity, which tightens the thoracolumbar fascia in the direction of the contralateral scapula. This probably facilitates LT with consequently higher muscle fibre recruitment. It would be interesting to investigate the role of the latissimus dorsi in this. Possibly, the scapula is destabilised by this muscle when the heterolateral leg is extended and therefore requires higher LT activity.
SA on the other hand has been described as part of an anterior flexion chain that runs from the heterolateral leg flexion musculature and internal oblique muscle, through the homolateral external oblique muscle to SA. When the heterolateral leg is extended, antagonistic leg flexion musculature is inhibited. Consequently, the anterior flexion chain is not operative. This could explain why SA activity is lower when the heterolateral leg is extended.
To clear out the influence of homolateral leg extension, we compared scapular muscle activity during exercise 1 and exercises 3 and 6. Because there were no differences in LT activity, we can conclude homolateral leg extension has no effect on LT muscle fibre recruitment. This is in agreement with the explanation given above. When the homolateral leg is extended, this exerts an effect to the heterolateral scapula along the posterior extension chain but not to the homolateral shoulder. The heterolateral leg bears more weight, resulting in a higher stabilising muscle activity encompassing the hip. This activates heterolateral internal oblique muscle, which in turn stimulates homolateral external oblique muscle activity, possibly resulting in higher SA muscle fibre recruitment.
Extrapolation of these results to other age categories or to shoulder patients should be performed with caution because our study population consisted of young, healthy subjects. Ludewig et al18 investigated scapular EMG activity during push-up exercises in both healthy subjects and subjects with shoulder dysfunction. They found no differences in how both groups responded across the exercises. However, it is more appropriate to investigate this with the exercises from this study before drawing conclusions. Furthermore, we should note that although our results are a good basis for selection of appropriate exercises for rehabilitation of scapular intramuscular balance, no proof has been given that training results in better scapular function. This is an interesting topic for further investigation.
Another important limitation of this study is the use of surface EMG during dynamic movements. Precautions were taken by following SENIAM prescriptions and by maximal standardisation and accuracy.34 In addition, we strictly followed recommendations of previous investigations that used surface EMG to analyse scapular muscle activity.12 18 26 44 However, despite precautions, cross talk could have occurred during measurements.
Conclusion
We investigated scapular EMG activity during KPP and six commonly used variations. Four exercises with low UT/SA ratio can be selected for rehabilitation of intramuscular balance in overhead athletes with scapulothoracic dysfunction: standard KPP, KPP with homolateral leg extension, KPP with a wobble board and homolateral leg extension and one-handed KPP. The use of a wobble board during KPP exercises nor the performance of KPP on one hand has an influence on scapular muscle EMG activity. It would be interesting to investigate other aspects of motor control, such as muscle timing and recruitment patterns, during KPP exercises and variations.
When using a kinetic chain approach during KPP, heterolateral leg extension increases LT activity, whereas homolateral leg extension increases SA activity. Further research should investigate EMG activity of the important muscles involved in anterior and posterior muscle chains, such as gluteus maximus, latissimus dorsi and the abdominal muscles, to determine their role in this.
What is already known on this topic
Scapular dyskinesis is recognised to contribute to impingement. Little evidence-based research is available to guide physical therapists in their choice of exercises.
What this study adds
Some KPP modifications are preferable over others because of their low UT/SA ratio. Extension of the homolateral or heterolateral leg during KPP influences scapular muscle activity differently.
Acknowledgments
The authors would like to thank Mr Kristof De Mey for his assistance with the manuscript.
References
Footnotes
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study was conducted with the approval of the Ethical Committee, Ghent University Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.