Article Text

Abstract
Introduction Recent studies report the incidence and epidemiology of injury in professional rugby union; however, there is limited research in amateur and youth rugby. Injuries in youth rugby may have consequences for sports participation and physical development. The authors performed a prospective cohort study of injuries during youth community rugby.
Methods An injury surveillance programme was established for the 2008–2009 season (9 months, 1636 player-hours) of an English community rugby club. The study included 210 players, all males, in Under 9 to Under 17 (U9–U17) age groups. These were categorised into mini, junior, pubertal and school participation age groupings. Injuries were defined according to the International Rugby Board consensus statements.
Results There were 39 injuries reported (overall injury rate 24/1000 player-hours). Injury rates ranged from 0 to 49.3/1000 player-hours. More injuries occurred in junior (34.2/1000 player-hours) than in minis (11.9/1000 player-hours) (p<0.025). Higher numbers of moderate (20.6/1000 player-hours, p<0.005) and severe (9.5/1000 player-hours, p<0.05) injuries occurred in the U16–U17 age groups compared with younger age groups (U9–U10) where only minor injuries were reported. Most injuries occurred in the tackle (59%). The knee (4.9/1000 player-hours), shoulder (4.9/1000 player-hours) and head (4.3/1000 player-hours) were the most commonly affected areas. Concussion (1.8/1000 player-hours) affected half of the head injuries.
Conclusions Injuries in youth rugby occur infrequently and are lower than in adult series. The risk of injury and severity of injury increases with age. This study highlights the need for further research into injury risk factors around puberty and the need for first aid provision.
Statistics from Altmetric.com
Introduction
Rugby union is gaining in popularity, with increased numbers of children and adolescents playing regularly. In the 2008/2009 season, over 1.2 million children in England played rugby in schools and clubs.1 While there have been several recent studies reporting the incidence and epidemiology of injury in professional rugby union, there is limited understanding of the injury profile in amateur and in particular youth rugby.2
Studies in youth rugby have tended to be surveys in the school sports setting with limitations regarding the level of exposure. There are some series reporting on youth club rugby but very little information about injuries in rugby players under the age of 11 years.3,–,13
The injury rates recorded in the school setting include 17.6/1000 player-hours for ‘all injuries’ attending a casualty station recorded over 18 years in one Australian high school and 19.8/1000 player-hours in a study over 30 years in an English secondary school.7 9 Roux et al reported a lower rate of 7/1000 player-hours in South African secondary schools. Under-reporting from unsupervised observers was thought to contribute to the low injury rate.8 More recent series report rates of 27.5/1000 player-hours in New Zealand and 15.2/1000 match exposures in mixed series of American players.5 6 In community youth rugby in Argentina, the rate was 15.5/1000 player hours in youths aged 6–15 years.13 All these studies had methodological differences of age spectrum, player gender and injury definition, making comparison difficult.
Along with other contact sports, there is general acceptance that there is a risk of injury involved in playing rugby. The risk of serious injury is commonly thought to be less for children.14 Injuries sustained in youth sport may have significant consequences for physical development and activity.15 Patterns and profiles of injury in junior rugby have yet to be established. An understanding of injury characteristics in junior rugby is needed to inform injury-prevention strategies and possible rule changes aimed at player safety at the developmental level.
We performed a prospective cohort study to determine the match injury rates occurring in English community youth rugby union. Additional objectives were to identify incidence and severity of injury in different age groups, the anatomical location of the injury and the phase of play during which injuries occurred.
Method
An injury surveillance programme was established for the 2008–2009 season (9 months) at a large community rugby club in England. Ethical approval for the study was obtained from The University of Bath Ethical Committee.
All players participating in community rugby with the club were informed of the surveillance programme, and consent was obtained from their parents. The study included 210 players aged from U9 to U17.
Data on match exposure were collected by match observation by the coach, to determine the number and duration of matches played. Player exposure was determined by the number of players in each team multiplied by the total duration of the match or matches.
The coach or first aider responsible for each team observed matches and recorded players injured during each game together with the details regarding phase of play. All observers attended a preseason educational session regarding data collection. Full details of injuries (player's age, team, position, site and side of injury, type of injury if known and the event that caused the injury) were collected by the researcher for each injured player and recorded on an injury form. Minor injuries were confirmed by the coach or first aider. Formal diagnoses were obtained on those who attended their general practitioner or emergency department. Injuries were defined according to the International Rugby Board (IRB) consensus statements for injury and injury severity.16 An injury was defined using the definition used for the English Premiership studies 2002–2004 for consistency as ‘any injury that prevents a player from taking a full part in all training and match play activities typically planned for that day for a period of greater than 24 h from midnight at the end of the day the injury was sustained.2 16
Injury severity was determined by duration of injury and was based upon the IRB consensus statement with injuries being defined as minimal (2–3 days), mild (4–7 days), moderate (8–28 days) and severe (>28 days).16 Slight injuries (0–1 days) did not fall into the injury definition of this study where injury was only included if lasting longer than a ‘slight’ injury. Minimal and mild injuries were combined as minor injuries.
Players were followed up weekly to determine, to the nearest day, when the player was fit to return to play. Players were determined to have recovered when they were fit enough to be able to return to play in the playground, during school sports activities or with the rugby club. Fitness was defined by Brooks et al as ‘able to take a full part in training activities typically planned for that day and available for match selection.’2
The data were analysed by injury rate overall, age group, different age groupings and phase of play. The age groupings selected were minis (U10–U12), juniors (U12–U17), junior school (U9–U11) and senior school (U12–U17), and three developmental age groupings: prepubertal (U9–U10), peripubertal (U11–U13) and pubertal (U16–U17). The injury severity was analysed for minor (1–7 days), moderate (8–28 days) and severe injuries for each age group and for each age grouping. The site of injury was assessed by region: head and neck, upper limb, lower limb and trunk.
The rationale for the selected groupings is as follows:
Minis and juniors. These grouping are used in the club setting where the Rugby Continuum provides law variations for the developmental game. Minis have smaller pitch sizes, shorter duration of games and a smaller team size compared with juniors.
Junior school and senior school. The education structure provides these groupings. Within schools, there are differing levels of exposure to rugby; junior schools generally do not play rugby as regularly as senior schools, whose rugby season runs in parallel with the club season, so typically players are playing in both settings. Schools tend to follow the Continuum more loosely.
Stages of puberty. The pubertal development groupings reflect the changes in physical size, speed, aggression and style of play that occur with puberty.17
The variations in the game and pitch are illustrated in table 1.
Progression of changes of team, rules and pitch size in English youth rugby
Statistical methods
Injury rates were calculated as the number of injuries per 1000 player-hours of match time for each age group team. Rates were calculated for minor, moderate and severe injuries, and were stratified by level of play in single year age groups and in age groupings, mini, junior, junior school and senior school, and prepubertal, peripubertal and pubertal. Rates were calculated by site of injury and combined by anatomical area. Injury rates were calculated by phase of play in which injury occurred.
Statistical analysis was performed using χ2 and comparison of 95% CI. A level of p<0.05 was considered statistically significant. The null hypothesis was that there was no difference in injury incidence and severity between age groups. Where the 95% CIs did not overlap, the result was deemed to be statistically valid. Linear regression was performed to compare injury rates with age group (SPSS version 18).
Results
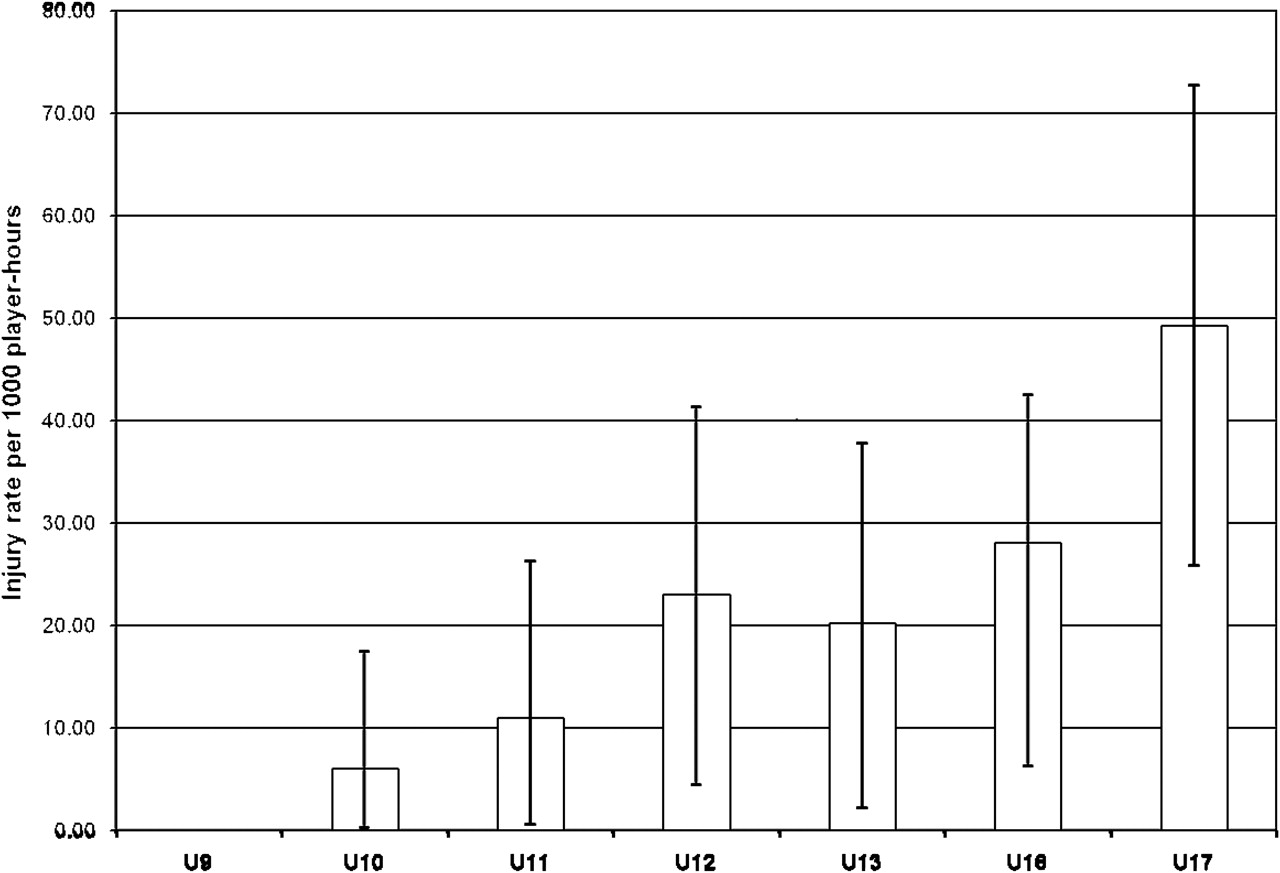
The number of players studied was 210, all male, over 1635.8 player-hours. Thirty nine injuries were recorded to 33 players, with three players (U13, U16 and U17) injured twice and one player (U17) injured four times. The overall injury rate was 24/1000 player-hours (95% CI 16.4 to 31.3). The U17 age group was injured significantly more frequently (49.26/1000 player-hours, 95% CI 25.8 to 72.7) and with a significantly greater severity of injuries than the other age groups (p<0.025). Injury rates and severity increased significantly with increasing age (p<0.01). Juniors (U13–U17) have 34.2 injuries/1000 player-hours (95% CI 21.9 to 46.4), senior school age (U12–U17) 31.6 injuries/1000 player-hours (95% CI 21.3 to 41.9) and pubertal (U16–U17) 39.7 injuries/1000 player-hours (95% CI 17.8 to 45.6). Lower rates are found in the younger age groups with prepubertal (U9–U10) 3.2/1000 player-hours (95% CI 0.0 to 9.2), junior school (U9–U11) 6.0/1000 player-hours (95% CI 0.4 to 12.9) and minis (U9–U12) 11.9/1000 player-hours (95% CI 4.1 to 19.6). Overall, there is a trend towards increasing incidence of injury with age from 6/1000 player-hours at U10 to 49/1000 player-hours at U17 with linear regression of 5.15 per 1000 player-hours per year group (CI 3.57 to 6.74, R2=0.89) (figure 1). This is equivalent to one extra injury per 200 players-hours with each year older.

Injury rate per 1000 player-hours by team age group with 95% CIs. There was a trend to increasing injury with increasing age.
There was a statistically significant increase in the rates of moderate and severe injuries with increasing age for all age groupings (table 2). Minor injuries did not show any increase with age.
Comparison of injury severity between age groups
Minor injuries (<7 days) accounted for 41% of injuries and 4.5% of days lost, moderate injuries (8–28 days) 41% of injuries and 24.7% days lost and severe injuries (>28 days) 18% of injuries and 70.8% of days lost. Three of 17 injuries in the U17 age group were prolonged and could be considered ‘career ending injuries’ with projected absence of between 6 and 12 months, potentially two seasons. These were an anterior cruciate ligament injury and two meniscal tears requiring surgical repair.
Injuries occurred to the head (4.3/1000 player-hours (7)), neck (1.8/1000 player-hours (3)), shoulder (4.9/1000 player-hours (8)), wrist (1.2/1000 player-hours (2)), hand (1.8/1000 player-hours (3)), chest (0.6/1000 player-hours (1)), lower back (1.8/1000 player-hours (3)), knee (4.9/1000 player-hours (8)) and ankle (2.4/1000 player-hours (4)). There were no injuries recorded in the elbow, forearm, upper back, stomach, buttocks, groin, thigh, lower leg, foot or multiple areas.
When grouped into head and neck, upper limb, trunk and lower limb areas (figure 2), there are no statistical differences between the areas, although the trunk tended to be less affected than the head and neck and limbs. The head, shoulder and knee suffered the highest rate of injury. The numbers involved are too small to have statistical significance, although it is notable that approximately half (1.8/1000 player-hours (3)) of all head injuries were concussion. The description of concussion given to the observers in the preseason study educational session was ‘suffering from transient loss of consciousness, confusion, dizziness, nausea or visual disturbance following a head injury.’ The other head injuries were nose trauma (2) and laceration (2). Where injuries coexisted, only the main injury was reported.

Injuries per 1000 player-hours for all subjects by body area with 95% CIs. There was no statistical difference between the injury rates.
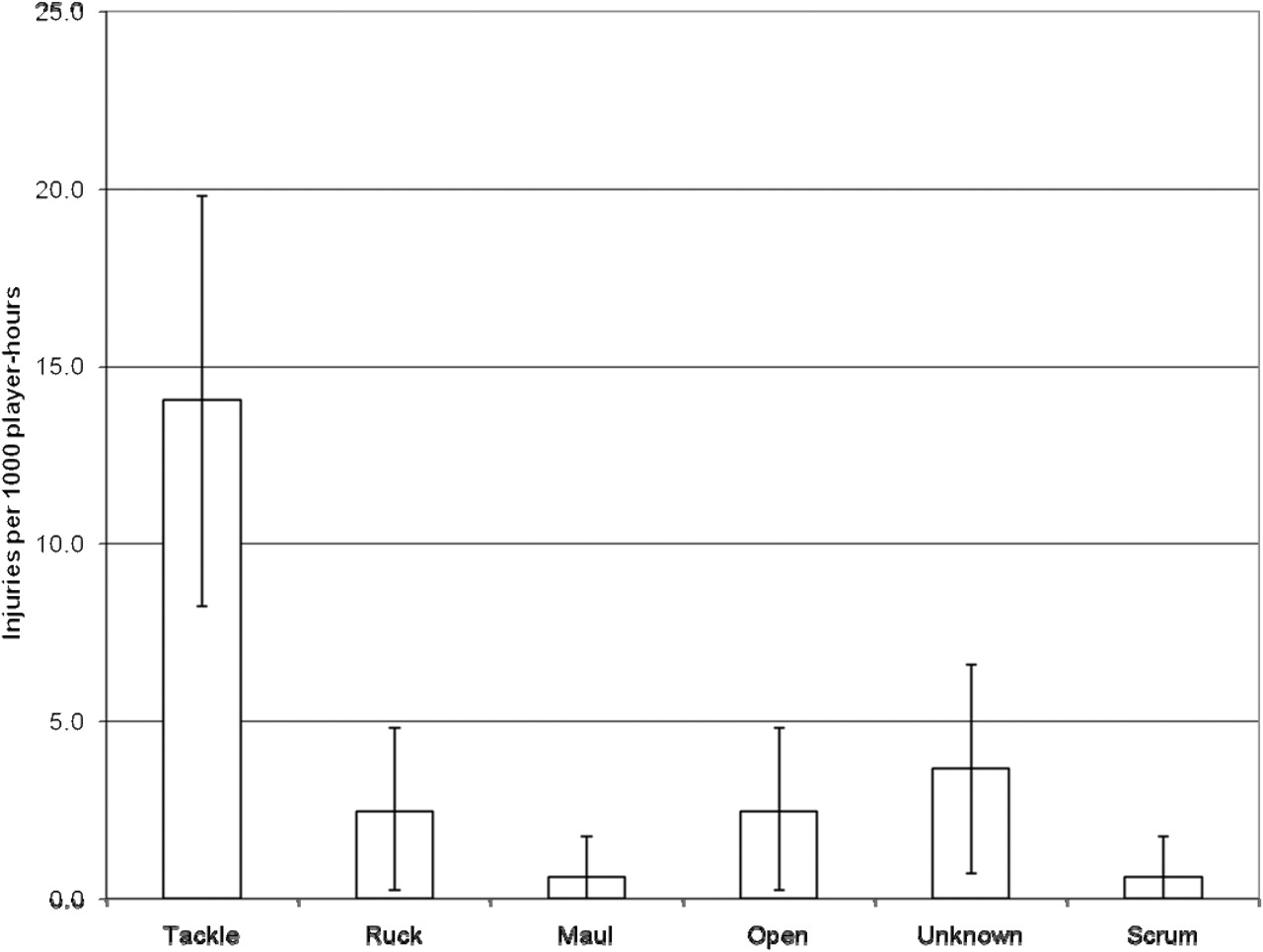
Significantly more injuries (59%) occurred during the tackle (p<0.001) than occurred during other phases of play: ruck, maul, scrum, open and unknown phases (figure 3). Tackle injuries included those to the ball carrier and the tackler.

Injuries per 1000 player-hours by phase of play causing injury with 95% CIs. Significantly more injuries occurred in the tackle compared with other phases of play.
Injury incidence and severity tended to increase with increasing age (figure 4).

Injury incidence by age group and by severity as defined by the International Rugby Board consensus statement35 minimal 1–3 days, mild 4–7 days, moderate 8–28 days and severe more than 28 days. Injury incidence and severity tended to increase with increasing age.
Players returned to play at a mean of 32 days. This varied between 0 in U9 and 54.1 days in U17 (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean duration of injury in days by age group with 95% CIs. Players returned at a mean of 32 days following injury.
Older players took a longer time to return to play following injury than younger players (figures 4, 5). This has not been analysed statistically by age group, as the small numbers allow only a descriptive analysis. Further analysis is provided for severity, which uses duration as a proxy.
Discussion
We found that the overall injury rate in junior community rugby union was 24/1000 player-hours. This is similar to the other published series. The variation of injury rates with age group has been reported for rugby participation increasing from 43.3 per 1000 player-hours in U13 to 56.2 in U15 and 63 in U18.18 We found that injury rates and severity increased significantly with increasing age (p<0.01). There was a good correlation between increasing age and increasing injury rate (R2=0.89). We appreciate this study is underpowered, and this may introduce Type I errors into the statistical analysis.
Previous studies of childhood injuries show peaks between 13 and 15 years of age rather than a uniform trend.19,–,21 Emery reviewed risk of injury in childhood and adolescent sport increasing with age, but the data were not consistently adjusted for exposure.14 In children's injuries sustained during soccer participation, the trend for increasing injuries with age is found, and this trend is maintained when exposure is considered.22,–,25
The injury rate for U17 at 49.3 injuries/1000 player-hours is higher than some recorded rates for youth rugby. Durie and Munro recorded a higher injury rate in youth rugby at 65/1000 player-hours in the First XV (16–18 year olds), although different injury definitions were used.6
The most frequent anatomical sites of injury in youth rugby union were found to be the head, neck, shoulder and wrist. Although these are comparable in distribution to series of adult players (table 3), there are several differences which are of interest. Concussion in this series occurred in approximately half of youth head injuries during rugby compared with 58% of missed game injuries in a youth series and 30% in an adult series.2 18 There is concern that there is significant under-reporting of concussion in adult studies.26 The thigh and lower leg represented a high proportion of injuries in adult rugby (table 3), but a much lower incidence occurred in youth rugby. As previous injury is a major risk factor for thigh and lower leg injuries, the lower rate may reflect the fact that youth players are less likely to have an injury history.
Site comparison between this study and Premiership2
This study shows that younger players have fewer severe injuries than older players. Minor injuries (<7 days) show no significant difference in any age grouping, but moderate injuries (8–28 days) and severe injuries (>28 days) increase with age in each of the different age groupings. These results may be influenced by attitudes to injury together with physical and endocrinological developmental changes. The older players will have progressed through their growth spurt and will be gaining muscle strength prior to musculoskeletal maturity.
We were fortunate that no catastrophic injuries occurred in our series, although the probability of observing such an injury in a study of this size is extremely low, with Fuller estimating the risk as being 0.8 per 100 000 players per year.27 Dalley et al reported increasing moderate and severe injuries with increasing age when comparing chest, back and concussion with age, and McIntosh et al showed a trend for increasing incidence of head, neck and face injuries with age.4 18
With growth and development, the body undergoes a series of changes, which may be contributory factors to injury in contact sports. Strength, speed and power increase with age, resulting in increasing maximum momentum and thus increasing potential force transfers.17 28 Pubertal changes due to increased testosterone in boys lead to increased aggression and risk-taking behaviour.29 Mismatch in size is often raised as an issue for injury, but according to the literature there is currently no evidence that this is a cause of rugby injuries.11 18
We considered that a threshold of development and size may eventually be reached by youth players leading to adult patterns of injury. We have not been able to demonstrate this statistically in our series but have observed that older age groups (U16 and U17) have an injury pattern tending towards those of adult series.
The average injury duration for the U16 and U17 teams was comparable with the English World Cup squad 2003 and English Premiership 2002–2004.2 30 Despite this similarity, comparison of return to play in youth rugby with series featuring professional players has limited validity. The determination of fitness and the return to training and play is less reliable than that in the professional sports setting. In addition, the injury duration in this series was counted in units of weeks rather than days, as in professional series. In community youth rugby, some of the time spent ‘injured’ will be waiting for appointments and treatment, and at times patchy access to rehabilitation prolonging recovery times. Where it is available, commitment to rehabilitation may be influenced by factors such as school work and social activities. Professional players by comparison, as well as having immediate access to significant medical and rehabilitation resources, have fewer external constraints on compliance with their rehabilitation.
Other factors which may influence injury rate and severity are in the law variations and game and pitch characteristics of youth rugby (table 1). Rolling substitutions are encouraged in youth rugby to ensure maximum participation and enjoyment. With increasing age, play occurs more similarly to the competitive selection principles of adult rugby, with less use of the rolling substitutions and increasing playing time for the better players. Fatigue may become an injury risk factor in the older age groups. The progression in duration of games, team size and pitch dimensions with increasing age may not influence injury rate directly, but may give a different style of play with differing player density and space for open play.
Regarding phase of play, injuries occurred most commonly during the tackle (59%) similar to adult series and affected the head, shoulder and knees.11 28 31,–,35 This highlights the importance of good coaching practice around correct tackling techniques, player conditioning and application of the laws of rugby.11
This study highlights the need for further research into injury risk factors around puberty, the need for first aid provision and in particular the awareness of concussion in young rugby players. We consider that a trained first aider in addition to the coach should be present at youth rugby games.
Age groups with the highest injury burden in rugby are the adolescents and school leavers, a stage of life which has been shown to be associated with giving up organised sporting. Unless injuries are managed in a timely manner, with access to the necessary resources, the risks of the cessation of sporting activity in adulthood may be increased.
Conclusion
Injuries in junior youth rugby occur infrequently. Injury rates are notably lower than those reported in adult series. The risk of injury is extremely low in U9 players but increases with increasing age, as does the risk of severe injury. This study highlights the need for further research into injury risk factors around puberty, the need for first aid provision and in particular awareness of concussion in young rugby players.
Acknowledgments
The authors would like to acknowledge the contributions of the youth players, parents, coaches and first aiders at Longlevens Rugby Club Gloucestershire. The contribution from C Foy for statistical advice is also acknowledged.
References
Footnotes
-
Competing interests None.
-
Ethics approval Provided by the University of Bath Ethical Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.