Article Text

Abstract
Objective Injection treatments are increasingly used as treatment for patellar tendinopathy. The aim of this systematic review is to describe the different injection treatments, their rationales and the effectiveness of treating patellar tendinopathy.
Methods A computerised search of the Medline, Embase, CINAHL and Web of Knowledge databases was conducted on 1 May 2010 to identify studies on injection treatments for patellar tendinopathy.
Results 11 articles on seven different injection treatments (dry needling, autologous blood, high-volume, platelet-rich plasma, sclerosis, steroids and aprotinin injections) were found: 4 randomised controlled trials (RCTs), 1 non-RCT, 4 prospective cohort studies and 2 retrospective cohort studies. All studies reported positive results. The Delphi scores of the four RCTs ranged from 5 to 8 out of 9. Different and sometimes contradictory rationales were used for the injection treatments.
Conclusion All seven different injection treatments seem promising for treating patellar tendinopathy. Unlike the other injection treatments, steroid treatment often shows a relapse of symptoms in the long term. Results should be interpreted with caution as the number of studies is low, few high-quality studies have been conducted and the studies are hard to compare due to different methodology. More high-quality studies using the same cross-cultural reliable and valid outcome measure are needed, as well as further research into the pathophysiology. Finally, some implications are provided for clinicians who want to use injection treatments as a part of their treatment for patellar tendinopathy, distinguishing between reactive and degenerative phase of patellar tendinopathy.
Statistics from Altmetric.com
Introduction
Patellar tendinopathy or jumper's knee is characterised by activity-related anterior knee pain associated with focal patellar tendon tenderness and intratendinous imaging changes.1 This injury is often found in both recreational and top-level athletes.2 The prevalence is high especially in sports placing a high demand on speed and power for the leg extensors. Prevalence of patellar tendinopathy among elite volleyball and basketball players is 32% and 45%.2 As many as 53% of athletes with jumper's knee even retire from their sport because of this injury.3
The current concept of jumper's knee is that the underlying pathology is a degenerative tendinosis due to a failed healing response rather than a tendinitis.4,–,9 Although the exact aetiology, pathophysiology and healing mechanisms are not fully understood, it seems that cumulative microtraumata occur because of repetitive overload. The healing capacity of the tendon can be insufficient, and leads to a tendinosis zone.10 11 Another hypothesis is that inflammation plays a role in the early stage as well as in the chronic stage of tendinopathy.12 Recently, it is suggested that patellar tendinopathy has a pathology continuum which starts with reactive tendinopathy (inflammation) and can progress to a degenerative tendinopathy with a potential of reversibility.13
Many different treatments are used for patellar tendinopathy, such as rest, anti-inflammatory medication, eccentric training, extracorporeal shockwave therapy and surgery. No single treatment has proven to result in a consistent, near-complete recovery in all patients.10 14 15 The most common (usual care) intervention for patellar tendinopathy is eccentric exercise. Single-leg decline squats are often used to increase patellar tendon forces.15,–,17 Performing an eccentric exercise programme provides a 50–70% chance of improving knee function and pain, so that athletes can return to pre-injury levels of sports activity.18 However, in many patients, an eccentric training programme is not successful, therefore other methods of treatment have been developed, including (peri)tendinous injections. A certain volume of a liquid is injected into or close to the affected tendon to treat patellar tendinopathy. Many different injection methods, fluids and medication are currently used. To our knowledge, a comparison of the effectiveness of the various injection treatments does not exist. The aim of this systematic review is to describe the different injection treatments, their rationales and their effectiveness in treating patellar tendinopathy.
Methods
A computerised literature search of the Medline, Embase, CINAHL and Web of Knowledge databases was performed on 1 May 2010. The reviewers accomplished database searches with a combination of relevant search terms (figure 1). Search terms on existing injection methods were phrased based on the expertise of sports medicine physicians of University Medical Center Groningen and by searching relevant literature. The search was limited to literature published in English. A total of 153 unique articles were found in the literature search.
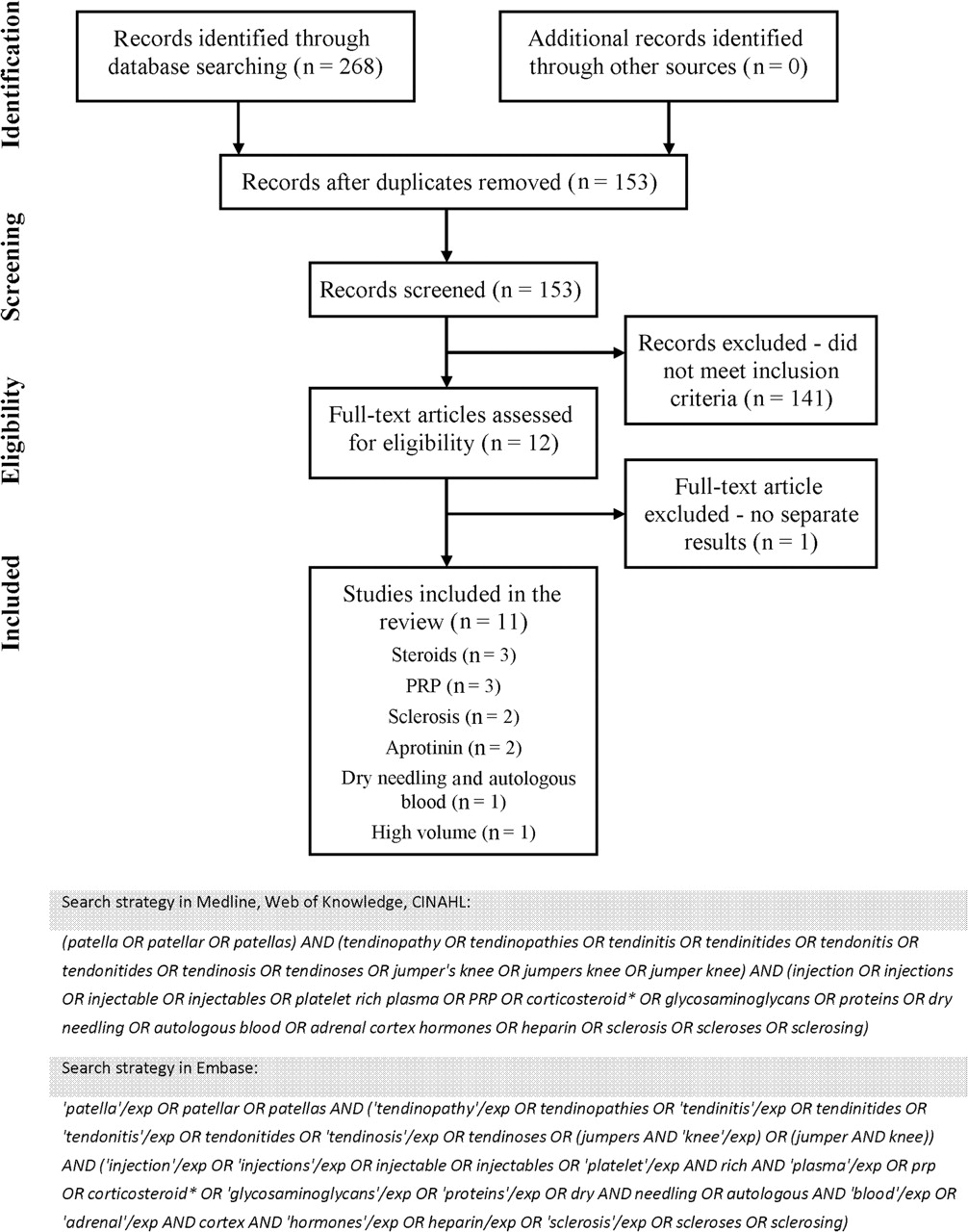
{kind=link}
Literature search.
Only articles that met the following criteria were assessed:
Research population of humans with a diagnosis of patellar tendinopathy.
Research on the effectiveness of one type of injection treatment.
Clinical trials with pain, sport activity, patient satisfaction and/or physical tests as outcome measures.
Studies in patients with several different tendinopathies were only included if the results for patients with that condition were described separately. Titles and abstracts were examined independently by two reviewers to include those articles that met the aforementioned criteria. Twelve of the 153 studies met the criteria and were included after examining their title and abstract. The reference lists of the included articles were hand-searched to find other possibly relevant studies. No additional studies were found during this search. After reading the articles, one study was excluded in which multiple tendinopathies were investigated and no separate results provided for patellar tendinopathy. Hence, the total number of studies included in this review is 11.
Two assessors independently assessed methodological quality of the included articles using Delphi criteria.19 The Delphi list is originally designed for the quality assessment of randomised controlled trials (RCTs). In this review, the non-RCTs were also scored on this list to make some comparison possible. Although non-RCTs will not be able to obtain the maximum score as a result of the design of the Delphi list, in the comparison with RCTs this in fact will reflect the lower level of these studies. To be able to compare the non-randomised studies with each other, these were additionally scored for methodological quality on the Newcastle-Ottawa Scale (NOS).20 Although comments on this scale exist,21 Deeks et al22 concluded that this scale is suitable for use in a systematic review. When the scores (Delphi and NOS) per assessor differed from each other, a consensus was reached in a meeting with both assessors.
Results
Eleven studies included 4 RCTs, 1 non-RCT, 4 prospective cohort studies and 2 retrospective cohort studies. Table 1 summarises the main features of these studies, with the injection treatment on which the most high-quality research is performed listed first. Studies on seven different injection treatments were found in the literature search. These included three studies on platelet-rich plasma (PRP), three on steroids (one in combination with aprotinin), three on sclerosis, three on aprotinin (one in combination with steroids), one high-volume and one dry needling and autologous blood injection. No studies on heparin injections were found. The studies included patients with symptomatic patellar tendinopathy with a duration ranging from 1 to 240 months. Furthermore, most studies included patients who had not improved with various other treatments. Age of the subjects ranged from 17 to 55 years and most subjects were athletes ranging from recreational to elite level. In most cases, the Victorian Institute of Sport Assessment – Patellar questionnaire (VISA-P) or a pain level on a Visual Analogue Scale (VAS) was used as primary outcome measure. All studies reported the positive effects of the investigated injection treatment. The two assessors who performed the quality assessment agreed on 95% of the items of the Delphi list and on 92% of the items of the NOS. A consensus was reached in a meeting with both assessors. The Delphi scores ranged from 1 to 8 on a 9-point scale, with the score of the four RCTs ranging from 5 to 8 points. The score of the seven non-randomised studies on the NOS ranged from 2 to 6 on a 9-point scale.
Published studies on injection treatments for patellar tendinopathy
Steroids
Most high-quality studies investigated steroids; three RCTs, by Fredberg et al,23 Kongsgaard et al24 and Capasso et al,25 were conducted on steroid injection treatments. The authors describe different reasons to include a steroid treatment group in their trial. Ultrasound images show that steroids can reduce inflammation and oedema of a tendon,26 but cannot repair degenerative changes. Although sparse histological documentation of inflammatory cells in damaged tendons exists, Fredberg et al23 postulated that change in a tendon can be both degenerative and inflammatory, and a significant reduction in oedema and thickness of the steroid-treated tendons can probably be achieved through an influence on inflammatory processes. According to Kongsgaard et al,24 effects of steroid injections on patellar tendinopathy remain elusive. Some studies indicate harmful effects whereas others found reduced tendon pain, swelling and vascularisation. For this reason, Kongsgaard et al24 included a steroid group in their research. A steroid group is also included in a study by Capasso et al25 because steroids are often used in the management of both tendonitis and degenerative joint disease.
Fredberg et al23 concluded that a steroid treatment can normalise the ultrasonographic pathological lesions in patellar tendons and has dramatic clinical effects. The often-seen relapse of symptoms in patients is ascribed to the combination of steroids with too aggressive rehabilitation. A limitation of the study is the short crossover period, which allows placebo and treatment groups to only be compared in the short term, while it is long-term effects that have particular clinical relevance.
The study of Kongsgaard et al24 evaluated clinical, structural and functional effects of steroid injections, eccentric training and heavy slow resistance training in patellar tendinopathy. They suggest that the investigated treatments had similar (positive) short-term effects; however, on a long-term basis, the eccentric and resistance group maintained their effects, whereas the effects of steroids deteriorated at 6-month follow-up.
The aim of Capasso et al25 was to investigate the efficacy and tolerability of aprotinin injections. The results of steroid treatment were significantly worse than aprotinin treatment. One of the limitations of this study is the outcome measure. A clinical assessment of symptoms and sport resumption classified as poor, fair, good or excellent as outcome measure has its limitations, and it is questionable whether this is a sensible and reliable outcome measure.27 Furthermore, the lack of a baseline measurement is another limitation of the study.
It is remarkable that all outcome measures in the steroid injection studies of Kongsgaard et al24 and Capasso et al25 showed improvement in the short term, yet improvement deteriorated in the long term (6 months). A relapse was also observed by Fredberg et al23 from the 4-week to 6-month follow-up. Further, the final follow-up measurements of the studies of Kongsgaard et al24 and Capasso et al25 showed better outcomes of, respectively, training protocols and aprotinin injection than of steroid injection.
Sclerosis
The effects of sclerosing injections on patellar tendinopathy patients are investigated by two studies by Alfredson and Ohberg28 and Hoksrud et al.29 Sclerosis is the injection of a chemical irritant (eg, polidocanol). A link between neoneurovascularisation and tendon pain in patients with chronic patellar tendinopathy is assumed from previous research.30 Neovessels and accompanying nerves might be responsible for the pain symptoms; treatment with sclerosing injections targets the neovessels. It is hypothesised that by destroying the neovessels and accompanying nerves chemically, the tendon pain could be cured.
Alfredson and Ohberg28 found a significant decrease in pain during activity, concluding that sclerosis has a potential for curing tendon pain. The limitation of a lack of control group exists in this study. A strong trend towards a group-by-time interaction in VISA-P score after 4 months (p = 0.52) was found by Hoksrud et al.29 A significant improvement in VISA-P score (p = 0.01) was reported for the treatment group, whereas no change was reported for the control group (p = 0.86). A limitation of this study is the relatively short follow-up of the placebo group, yet the data of the control group indicate that no effect was present in the placebo period and dramatic improvement was observed when the control group was offered sclerosis treatment (crossover after 4 months). It is concluded that the observed changes can be attributed to the sclerosing injections, therefore sclerosis seems to be a promising treatment.
Aprotinin
Aprotinin injection treatment was investigated by Capasso et al25 and Orchard et al.31 The rationale of aprotinin treatment is based on many recent publications that found an increase in matrix metalloproteinases (MMPs) in tendinopathic tissue. Excessive collagenases may be a reason for delayed recovery in patients.32 With this presumption, Orchard et al31 and Capasso et al25 hypothesised that local injection of a collagenase inhibitor seems sensible for treating chronic tendinopathy. Aprotinin is such a collagenase inhibitor; in vitro, it is a strong inhibitor of MMPs, including the collagenases, with a likely mechanism of inhibition of the plasmin-activation pathway of MMPs.31
The study of Capasso et al,25 briefly described in the ‘Steroids’ section, suggests that aprotinin injections may have a lasting beneficial effect for patellar tendinopathy patients. Orchard et al31 conducted a retrospective cohort study, investigating whether aprotinin injection treatments for common forms of tendinopathy would lead to good clinical improvement. They concluded that for major load-bearing tendons (eg, Achilles, patella, hamstring tendons) in active individuals, aprotinin is a more appropriate second-line injection option than cortisone preparations. Limitations of this study are the lack of a control group and its retrospective design, and the outcome measures only comprise patients' opinions about their condition. Only two low-quality studies investigating aprotinin exist. Although results look promising, it is hard to draw conclusions from these studies.
Platelet-rich plasma
Three studies investigated the effects of PRP injection treatments for patellar tendinopathy: Volpi et al,33 Kon et al34 and Filardo et al.35 PRP is prepared from autologous blood, it contains a ‘cocktail’ of growth factors, which is coupled with a further release of these factors when the platelets are activated. Growth factor application has an important role in the healing of damaged tissue. This offers opportunities in aiding regeneration of tissue with low healing potential as in patellar tendinopathy. A complex regulation of several growth factors increases the expression of procollagen types I and III, improves mechanical properties and promotes tendon cell proliferation and tendon healing.34 The exact working mechanism of this complex process is not fully understood. The precise role of the ‘cocktail’ of growth factors is not clear, although it seems that among other growth factors platelet-derived growth factor (PDGF), transforming growth factor β (TGF-β) and vascular endothelial growth factor (VEGF) promote tissue healing.36,–,39
All studies concluded that PRP injection is a promising treatment. However, the quality of these studies is low (Delphi score = 2). Among the limitations are the absence of a control group and the use of a control group with different population characteristics than the treatment group.
Dry needling and autologous blood
Dry needling and autologous blood injections are only investigated in a combination in one study by James et al.40 Dry needling is repeatedly passing a needle through the abnormality of a tendon, and is applied to stimulate an inflammatory response within the tendon. James et al40 hypothesise that the collagen fibres in the tendinosis area are disrupted, stimulating an internal bleeding. Strengthening of the tendon should then be accomplished by the formation of granulation tissue which is a consequence of the inflammatory response. Their rationale for autologous blood injection closely resembles the previously described rationale for PRP; autologous preparations rich in growth factors induce cell proliferation and promote synthesis of angiogenic factors during the healing process. Several growth factors (eg, PDGF and TGF-β) may also act as humoral mediators in the induction of the healing cascade. For these reasons, they investigated dry needling in combination with autologous blood injection.
The aim of James et al40 was to assess the efficacy of ultrasound-guided dry needling and injection of autologous blood as a treatment for patellar tendinopathy. They concluded that this combination is a promising treatment for the condition. A limitation is the absence of a control group. The combination of therapies and low quality of this study furthermore complicate a statement about a single method of treatment.
High volume
High-volume injection treatment is investigated in one study by Crisp et al.41 The rationale used in this study is similar to that used for sclerosing injection treatment by Alfredson and Ohberg28 and Hoksrud et al.29 The hypothesis of Crisp et al41 was that disruption of neoneurovascularisation could be achieved by mechanical means, namely by injecting large volumes of fluid in the area where the neovessels penetrate the tendinopathic lesion (interface between the posterior aspect of the paratenon of the patellar tendon and Hoffa's body). Power Doppler ultrasound showed the immediate disappearance of neoneurovascularisation after injection.41 They additionally used small amounts of local anaesthetics and corticosteroids to relieve immediate pain and prevent an inflammatory reaction, respectively. Their aim was to evaluate a high-volume injection treatment for patellar tendinopathy. They found a significant improvement in VISA-P after a high-volume injection treatment and concluded that high-volume injections are helpful for the treatment of patellar tendinopathy. Because only one low-quality study on this treatment exists, it is hard to make definitive statements on the treatment. The main limitation of this study is its retrospective design, which may result in a recall bias as the VISA-P had to be completed in a retrospective manner. Furthermore, the small amount of corticosteroids that was added to prevent an injection-related inflammatory response may be a confounding factor.
Discussion
This is the first systematic review to provide a complete review of the existing literature on injection treatments for patellar tendinopathy. Eleven studies on seven different injection treatments were found, overall reporting positive outcomes. However, a careful interpretation of the results is necessary, as the number of studies is low and few high-quality studies are available. The mean Delphi score is only 3.4 (range 1–8) out of a maximum of 9.
The only injection treatment on which three RCTs were conducted is steroids. These studies indicate that steroid treatment is effective in the short term, yet show relapse in the long term. The results of a systematic review by Barr et al42 on the effectiveness of steroid injections compared with physiotherapeutic interventions for lateral epicondylitis show the same; whereas steroid treatments were favourable in the short term compared to physiotherapeutic interventions, the latter were more favourable in the intermediate-to-long term.42 Other reviews on steroid treatment for shoulder and elbow tendinopathy show relapse after steroid injections as well.43 44 A recurrence rate of 72% after steroid injections in lateral epicondylitis is reported.45 Additionally, an impaired synthesis of collagen has been found in tendons injected with steroids.24 It can therefore cautiously be concluded that steroids have a positive effect on patellar tendinopathy in the short term, but a relapse of the symptoms occurs in the long term.
As for the other injection treatments, all studies report positive outcomes. It might thus be possible that an intra- or peritendinous injection by itself already influences the symptoms of patellar tendinopathy positively. One of the insights on injection therapies is that any injection with an irritant solution can be beneficial for the treatment of a condition.46 A review on this so-called prolotherapy showed positive results of treatments groups compared with controls, although limited high-quality studies on prolotherapy for musculoskeletal pain or sport-related soft tissue injuries exist.46 Another possible explanation for the positive outcomes in all studies is the existence of a publication bias; also the low-quality designs have to be taken into account.
The limited number of studies makes it hard to draw firm conclusions on the effectiveness of the individual injection therapies. Only one of the studies included in this review compared multiple injection treatments, and found that aprotinin injections result in more improvement in patellar tendinopathy patients than steroid injections.25 However, the quality of this study is moderate and no other studies exist confirming these results. Further, there are only four RCTs and one non-RCT comparing injection treatment with a control group receiving training, no treatment or lidocaine injection. Because of differences in concurrent treatments, outcome measures, injection protocols and study populations, the studies are difficult to compare and no firm statements on the differences in effectiveness of the injection treatments can be made.
Another treatment besides injection is thought to be required to promote healing of a tendinopathic tendon, as the healing process is a complex system in which mechanical and chemical factors work together.47 48 A combination of an injection together with a mechanical stimulus (physical therapy) does raise the question where the possible effects can be ascribed to, injection or physical therapy. No studies exist in which injection therapy together with physical therapy is compared to physical therapy alone. However, in most studies described in this review, the symptoms did not improve from a previously performed exercise programme. Therefore, an injection in combination with physical therapy seems beneficial and might be of greater benefit than solely an exercise programme. Although some form of physical therapy programme was prescribed in all the studies, large differences exist between studies in type of concurrent treatments, which hinders comparisons. For example, in some studies, patients were allowed to resume their sport activities the second week after injection, whereas in other studies, patients were allowed to resume their sport activities after 12 weeks. Moreover, a combination of injection treatment with physical therapy results in inconclusiveness as to which treatment the effects can be ascribed to. Concurrent treatment, tendon loading in combination with an injection, does, however, seem to be needed for treatment effectiveness. In order to be able to compare the results, it is advised to standardise the concurrent treatment and report it clearly.
Another factor that makes it difficult to compare the studies is that no universal outcome measure is used. The most used outcome measure is the VISA-P, but several VAS scores, degree of satisfaction and the Tegner scale are also used. It is important to have the same reliable and valid outcome measure to compare studies; the need for internationally accepted golden standards in outcome measures is also described by Frohm et al.49 The most suitable outcome measure for studies investigating the outcome of treatments in patellar tendinopathy is possibly the VISA-P score, because it is a reliable index of the severity of patellar tendinopathy and it is specifically designed for that condition.50 This outcome measure is already used often in studies on patellar tendinopathy. Besides English, the VISA-P is also proven to be reliable and valid in Swedish,49 Italian51 and Dutch.52 The VISA-P score may provide a suitable outcome measure in these languages, but cross-cultural validation of the VISA-P for other languages has yet to be examined.
The studies also differed on the characteristics of the study population. One example is whether patients received previous therapy and which type. Patients in six studies were recalcitrant to previous treatments, one study had a ‘mixed’ population (91 had no previous therapy and 25 steroid treatment) and in four studies the previous therapy of the treated patients was not mentioned.24 29 31 40 Although the mean duration of symptoms was longer than 12 months in all studies, the range was wide (1–240 months). The fact that the effectiveness of injection treatments is determined in different patient groups complicates comparison of treatments.
No severe adverse events related to the injections were reported in the subjects of the reviewed studies. The worldwide distribution of aprotinin (Trasylol) is currently suspended by the distributor because of health risks when injected intravenously in high doses during cardiac surgery. In tendinopathy, an anaphylactic reaction is reported as a possible side effect of an aprotinin injection. An allergic reaction is rare after initial aprotinin injection (1 per 1000 reported in anaesthetics), however, not uncommon in following injections (up to 3% per injection) for chronic tendinopathies.53 Orchard et al31 reported 13 probable systemic allergic reactions, but these were managed by a single epinephrine injection. A sclerosing injection with polidocanol has a possible risk of tendon necrosis due to disturbed tendon blood flow, however, this risk is only small and much higher in, for example, surgery.28 29 Furthermore, a small chance of rupture of the tendon exists after every injection in or near a tendon. The steroid injection is the only injection treatment of which some evidence exists that it weakens the tendon and seems to increase the risk of rupture.54 55 Finally, a negligible chance of infection exists after every injection.
It can be concluded that more high-quality clinical studies are needed. The fact that the precise working mechanism of the injection treatments is not fully known also needs more research. Moreover, issues related to this, such as the place of the injection need more clarification. Seven of the reviewed studies used peritendinous and four used intratendinous injections. The studies on autologous blood and PRP injections all used intratendinous injections and the studies on all other injection treatments used peritendinous injections. It is demonstrated that intratendinous steroid injections can temporarily weaken the tendon in contrast to peritendinous steroid injections.54 Peritendinous steroid injections are therefore preferred. Further research is needed to obtain a better understanding of the effects of intratendinous versus peritendinous injections in other injection treatments.
In line with the previous discussion, further clarification of the pathophysiology is needed to better understand the different and sometimes contradictory rationales that are described. These rationales vary from stimulation of the healing process to inflammatory stimulation or suppression and neovessel destruction. Most research indicates that hardly any inflammation is involved in chronic patellar tendinopathy; it is thought to be a failed healing response. However, some researchers recently postulated that inflammatory cells are involved in chronic patellar tendinopathy and it actually may be a combination of a degenerative and inflammatory condition.12 56 Cook and Purdam13 advocate a model in which the pathology of a tendinopathy proceeds through several stages. They divided the pathology of patellar tendinopathy for clinical use into two stages: reactive/early tendon disrepair and degenerative/late tendon disrepair. Based on this model, biological reasoning and the current knowledge, some cautious recommendations can be given for clinical practice. In the reactive/early tendon disrepair phase, treatment should consist of load reduction, pain management (non-steroidal anti-inflammatory drugs) and, if one wants to give injection treatment in this phase, steroid injections. The other described injection treatments can be given in the degenerative/late tendon disrepair phase, as part of an exercise-based training programme including slightly painful eccentric exercises, to improve tendon regeneration. However, more research is needed to gain better insight into the pathophysiology and consequently the best injection treatment at each stage of patellar tendinopathy.
What is already known on this topic
Patellar tendinopathy is a hard-to-treat injury with a high prevalence especially in jumping athletes. Injection treatments are increasingly used as treatment for patellar tendinopathy. The amount of research on injection treatments is growing.
What this study adds
This is the first systematic review into injection treatments for patellar tendinopathy. The presumed working mechanisms of the injections and outcomes of the studies are presented. Overall, injection treatments seem promising, however, results need to be interpreted with care, as the number and quality of the studies are limited.
Conclusion
Overall, injection treatments seem promising for the treatment of patellar tendinopathy, however, present research is mainly of low quality and confers no clear benefit to a given intervention. Steroid injection treatment is effective in the short term, but shows relapse into pre-treatment levels in the long term. It is hard to draw firm conclusions on the effectiveness of injection treatments, as the number of studies is low and only few high-quality studies are available. The rationales of the several injection treatments differ, yet some seemingly contradictory rationales could have a place when considering the continuum model of tendon pathology. More high-quality clinical research and more research into the condition's pathophysiology are needed to determine whether injection treatments are effective and in which particular stage of patellar tendinopathy.
Acknowledgments
The authors would like to thank Karin Sijtsma of the Central Medical Library of the University Medical Center Groningen for her help during the literature search.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.