Article Text

Abstract
Background The incidence and outcomes of sudden cardiac arrest (SCA) and global strategies for prevention of sudden cardiac death (SCD) in football are not known. The aim of this study was to estimate the occurrence of cardiac events in football and to investigate the preventive measures taken among the Fédération International de Football Association (FIFA) member associations internationally.
Methods A questionnaire was sent to the member associations of FIFA. The first section addressed the previous events of SCA, SCD or unexplained sports-related sudden death within the last 10 years. Further questions focused on football player medical screening strategies and SCA resuscitation response protocols on the field.
Results 126 of 170 questionnaires were returned (response rate 74.1%), and 103 questionnaires (60.6%) were completed sufficiently to include in further analysis. Overall, 107 cases of SCA/SCD and 5 unexplained football-associated sudden deaths were reported. These events occurred in 52 of 103 responding associations (50.5%). 23 of 112 (20.5%) footballers survived. 12 of 22 (54.5%) players treated with an available automated external defibrillators (AED) on the pitch survived. A national registry to monitor cardiac events was established in only 18.4% of the associations. Most associations (85.4%) provide regular cardiac screening for their national teams while 75% screen teams of the national leagues. An AED is available at all official matches in 68% of associations.
Conclusions National registries to accurately measure SCA/SCD in football are rare and greatly needed. Deficiencies in emergency preparations, undersupply of AEDs on the field during matches, and variability in resuscitation response protocols and training of team-staff members should be addressed to effectively prevent SCD in football.
- Cardiology
- Cardiology prevention
Statistics from Altmetric.com
Introduction
Sudden cardiac arrest (SCA) is the leading cause of sudden death in athletes during sports participation.1 In 2012, two tragic cardiac events occurring in professional footballers in a relatively short period (Fabrice Muamba and Piermario Morosini) shattered the world of football and captured the attention of the sports medicine community around the globe. However, the precise incidence of exercise-related cardiac events in sport is unknown, and estimates highly depend on the category of athletes and sampling methods. Former surveys indicate that 0.7–3 young competitive athletes per 100 000 suffer from sudden cardiac death (SCD) per year.2–8
Currently, a baseline medical screening programme consisting of a personal and family medical questionnaire, a focused physical examination and a 12-lead resting ECG can detect the majority of genetically based potentially fatal cardiac abnormalities in footballers.9–14 To this preventive end, football's governing body, the ‘Fédération International de Football Association’ (FIFA) and specifically its Medical and Research Center (F-MARC) are committed to promoting and improving the prevention of SCD in football.15–18 However, despite the primary prevention strategies, there will always remain the risk of unexpected SCA during and after training and competition.4 ,7 Consequently, measures for the provision of basic life support (BLS), including the prompt use of automated external defibrillators (AED), have become the most important life-saving factor in the event of SCA in sport.19–22
In football, the world's most popular sport, played by more than 300 million players worldwide, limited studies are available which address the particular occurrence of SCA, outcomes of resuscitation and local implementation of current recommendations for emergency preparations. Thus, the primary intention of this study was to gain insights in the occurrence of catastrophic cardiac events in football, as well as primary prevention and resuscitation response protocols on the field among FIFA member associations.
Methods
There are 209 FIFA member associations. An electronic questionnaire (appendix 1) was sent to the chief medical officer of 170 FIFA member associations, who could be contacted for further enquiries if necessary. Owing to technical reasons, the survey could not be sent to 39 associations. The survey investigated three areas. The first section asked for football-related events of SCA, SCD or unexplained sports-related sudden death within the last 10 years. The second and third sections focused on established cardiac screening strategies and resuscitation response protocols (eg, BLS/AED) in case of cardiac arrest on the field. The responders had the possibility to specify their answers.
Descriptive statistics are reported as means, range and SD.
Results
In total, 126 of 170 questionnaires were returned (response rate 74.1%). Only 103 of the returned questionnaires (60.6%) were completed accurately and sufficiently to include in further analysis.
Events of SCA, SCD and unexplained football-associated sudden deaths
In total, 107 cases of SCA/SCD and 5 unexplained football-associated sudden deaths were reported in 52 of the responding FIFA member associations (50.5%; figure 1), and 51 of the FIFA member associations (49.5%) reported no cardiac events within the last 10 years.
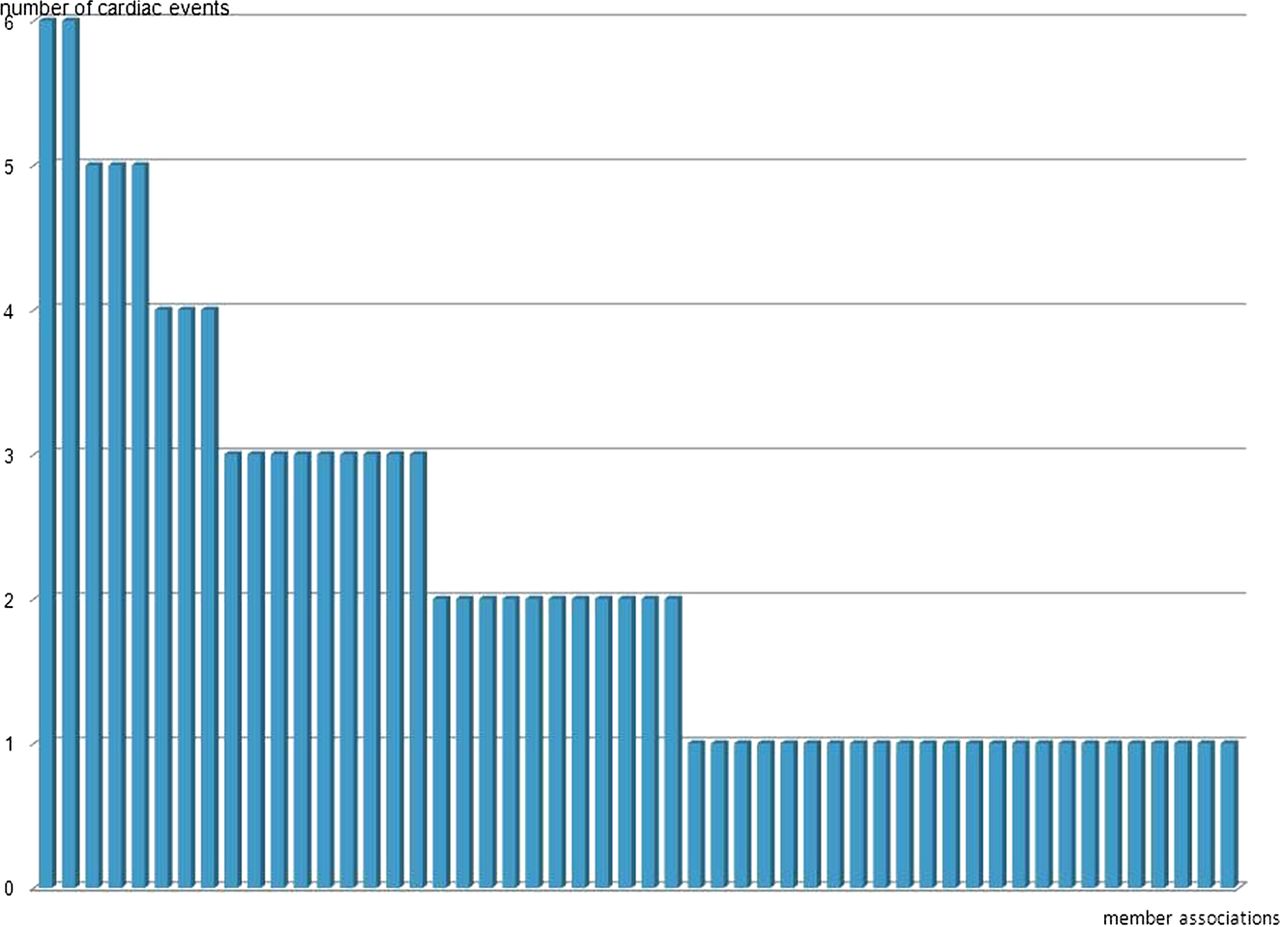
{kind=link}
Distribution of cardiac events within responding Fédération International de Football Association (FIFA) associations. Access the article online to view this figure in colour.
In the cases reported, the average age of the players that suffered cardiac events was 24.9 years (range 11–54, SD±13.8).
Death was the outcome of the cardiac event in 89 of 112 (79.5%) cases, and only 23 of 112 (20.5%) football players survived. Details of the resuscitation were provided in 95 of the 112 cases. Twenty-three cases were treated with an AED on the pitch. Twelve of the 22 (52.2%) football players with SCA treated with an available AED on the pitch survived, while 10 of the 23 (43.5%) died despite the use of an AED. In nine cases of SCA, the football player survived without the presence of an AED on the pitch, although the details of the emergency medical response by the ambulance are not known and may have included defibrillation.
Screening strategies to prevent SCD
Nineteen of the submitting FIFA member associations (18.4%) have a registry for cardiac events.
Eighty-eight FIFA member associations provide regular cardiac screening for their national teams (85.4%) while 66 FIFA member associations additionally screen the teams of their national leagues (64.1%). The majority of physicians follow the official FIFA precompetition medical assessment (PCMA) recommendations23—particularly in 87.5% of the national team screenings and 83.3% of the national league screenings.
The screening was initiated at an average age of 14.2 years (range 8–20, SD±2.2) in the national team players and at an average age of 15.3 years (range 10–21, SD±2.5) in the national league players.
Basic life support strategies
An AED is regularly available at official matches in 68% of FIFA member associations, with only 35% of FIFA member associations requesting an AED during both matches and training sessions. Financial resources and educational deficiencies were noted as the primary obstacles to implementing AED programmes.
An official ‘medical action plan’ for medical emergencies on the field is mandatory in 66 (64.1%) FIFA member associations that answered the questionnaire and 61 (59.2%) that mandate an annual simulation practice session by medical and team staff. Fifty-seven FIFA member associations provide regular BLS courses (55.3%).
The cardiopulmonary resuscitation (CPR) and AED skills are highly variable depending on the staff function (table 1).
Basic life support skills of different staff positions
Discussion
Although the overall incidence of SCD in sport is a relatively low-frequency event, its tragic occurrence demands an evaluation of current preventive measures. This retrospective survey estimated the occurrence of cardiac events and assessed the prevention strategies of SCD in football across an international sample of FIFA member associations. The study presents important data to assist the development of FIFA policies aimed at the prevention of SCD in football. An initial estimation of the occurrence of SCA, SCD or unexplained sports-related sudden death in football among FIFA member associations was conducted along with an examination of cardiac event registries. The study also investigated the presence of PCMA compliant programmes for cardiovascular screening, and evaluated the resuscitation response protocols and staff BLS training in the event of a cardiac arrest on the field.
Although football is the world's most popular sport and highly visible in the professional arena, the true incidence of catastrophic cardiovascular events in football is unknown. Interest and awareness of this medical problem are evident as reflected by the high return rate of the questionnaire (74%) by member associations. However, only 18.4% of the FIFA member associations had existing national registries for SCA and SCD in their national football associations. The lack of such national football registries makes it difficult to estimate the global incidence of SCD in football, probably leading to an underreporting of the problem.
Although the sampling method underlies a relevant sampling bias, it provides striking data: The survey documented 112 cardiac arrest events within the last 10 years, implicating at least almost one cardiac arrest per month, which were reported in only half of the FIFA member associations, with the rest reporting no events, either because their occurrence was unknown or non-existent. A number of the FIFA member associations reported only a single fatal event during the past decade, raising the possibility of undetected and unreported cardiac events. Therefore, one of the outcomes of this study is the need to establish national SCA registries in all FIFA member associations to monitor and establish the true incidence of SCA and related events in football in the future.
Overall survival from exercise-related SCA in the young was reported in only 11% in a series of 486 cases in the USA from 2000 to 2006.24 This study suggests that survival from SCA in football can be greater than 50% if an AED is available and used promptly on the pitch. Although the survival rate in the current study might be overestimated by a sampling error, other studies have also demonstrated a high survival rate (64%) for on-site AED use in young athletes with SCA.25 The lower survival rates of SCA on the field may reflect the absence of an AED, lack of recognition or an error in cardiac arrest diagnosis (eg, vasovagal syncope or seizure).25 Nevertheless, current international CPR guidelines underline the importance of effective and efficient CPR (eg, chest compressions) and the early use of an AED as the mainstay of a successful resuscitation from SCA.19
It is alarming that only two-thirds of the responding FIFA member associations (68%) have an AED regularly available at official matches and even less, roughly one-third (35%), provide an AED during training sessions. The lack of financial resources and relevant deficiencies in education concerning first-responder resuscitation on the field were listed as the main reasons for this dramatic omission and need resolution if the resuscitation capability on the football field is to be upgraded to acceptable standards. Currently, mandatory CPR and AED training appears to be available in only about half of the responding FIFA member associations (64.1% provide a default ‘medical action plan’ for medical emergencies on the field, 59.2% mandate an annual practice of the medical and team staff, and 55.2% demand regular BLS courses). It also appears that skills in CPR and AED use are highly variable, depending on the staff function. As expected, team physicians are the most well trained of all team and staff members. However, all team staff responsible for the supervision of players during training or competition should be trained to recognise and respond to a life-threatening emergency.
The current study was not designed to compare local features and regional differences. However, comparison to a recent survey of 190 top-level European football clubs and their facilities implicates that improvements in emergency preparations for cardiovascular events at sporting arenas are critically needed. For example, only 72% of these clubs reported the presence of an AED in their arena and 65% reported an existing CPR training programme.26
Despite modern resuscitation strategies, the best form of treatment is prevention of cardiac incidents in the first place. To this end, FIFA traditionally puts great emphasis on efforts to prevent SCD in football by means of its PCMA guidelines and regulations.17 ,18 ,27 ,23 This has resulted in two-thirds of the member associations providing regular PCMA screening for their national teams. However, availability of PCMA screening for the teams playing in the national leagues is much lower (52.4%). Despite the provision of PCMA, undetectable cardiac abnormalities at risk of SCA will persist and emergencies will continue on the football field. In these events, immediate and skilled first responder resuscitation on the field with prompt availability of an AED may well make the difference between life and death.
Limitations
The results of this survey have been reported without any validation method being available to confirm the results obtained, and the study findings represent only the responding FIFA associations (60%) with completed questionnaires. It is therefore possible that the actual reported occurrence of SCA and SCD is underestimated, which in essence may indicate a far larger problem than is evident from the reporting member associations. As aforementioned, a sampling error or reporting bias may have affected the number of events reported and subsequent survival rates. Owing to technical reasons, the questionnaire could not be submitted electronically to all member associations (170 of the 209 associations received the questionnaire). It was also not possible to obtain detailed clinical information or resuscitation details regarding all 112 cardiac events.
Conclusion
Exercise-related sudden cardiac events have become a major issue in international football. The development of national SCA registries is crucial to quantify and investigate SCA in football. Although the majority of FIFA member associations provide regular cardiac screening to national team players, this availability of screening needs to be further improved.
The unavailability of AEDs next to the field during competitions and training is unacceptable, as is the variability of CPR training of football team staff members, both of which require active resolution and promotion internationally.
To document the commitment of the FIFA governing body and as a consequence of this study, the FIFA Congress 2012 decided to provide each member association with an AED and a complete educational package for paramedics, coaches, athletic trainers and referees to raise the knowledge and have an action plan ready in case an emergency of SCA occurs. F-MARC will develop instructional courses within its developmental grass-roots programmes to include relevant information to prevent SCD.
What are the new findings?
-
Although the majority of Fédération International de Football Association (FIFA) member associations provide regular cardiac screening to national team players, this availability of screening needs to be further improved.
-
National registries to accurately measure sudden cardiac arrest/death (SCA/SCD) in football are rare but greatly needed.
-
Deficiencies in emergency preparations, undersupply of automated external defibrillators on the field during matches, and variability in resuscitation response protocols and training of team-staff members are obvious but should be addressed to effectively prevent SCD in football.
How might it impact on clinical practice in the near future?
-
The development of national sudden cardiac arrest (SCA) registries is crucial to quantify and investigate SCA in football.
-
The unavailability of automated external defibrillators (AEDs) next to the field during competitions and training is unacceptable, as is the variability of cardiopulmonary resuscitation skills training of football team staff members, both of which require active resolution and promotion internationally.
-
As such, the Fédération International de Football Association (FIFA) Congress 2012 decided to provide each member association with an AED and a complete educational package for paramedics, coaches, athletic trainers and referees to raise the knowledge and have an action plan ready in case an emergency of SCA occurs.
Acknowledgments
The authors gratefully thank Dr Yacine Zerguini, Dr Guncharah Singh, Dr Bert Mandelbaum, Dr Tim Meyer and Philipp Tobler for their crucial support in developing and distributing the questionnaire.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors All the authors listed contributed and serve as guarantors of the paper. They accept full responsibility for the work and the conduct of the study, had access to the data, and controlled the decision to publish. The authors of the manuscript contributed to this work as follows: CS, JD, EK and JDv substantially contributed to the conception and design of the study/questionnaire, as well as the acquisition, analysis and interpretation of data. CS drafted the article and revising it critically for important intellectual content. JDr, EK and JDv revised the manuscript critically for important intellectual content CS, JDr, EK and JDv were involved in final approval of the version to be published.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
▸ References to this paper are available online at http://bjsm.bmj.com