Article Text

Abstract
Background Groin/hip injuries are common in the athletic population, particularly in sports requiring kicking, twisting, turning and rapid acceleration and deceleration. Chronic hip, buttock and groin pain account for 10% of all attendances to sports medicine centres. Understanding risk factors for field-based sports (FBS) players is important in developing preventive measures for injury.
Objective This systematic review aims to identify and examine the evidence for groin/hip injury risk factors in FBS.
Methods 14 electronic databases were searched using keywords. Studies were included if they met the inclusion criteria and investigated one or more risk factors with relation to the incidence of groin/hip injuries in FBS. Studies were accumulated and independently analysed by two reviewers under a 12-point quality assessment scale (modified CASP (for cohort study design) assessment scale). Owing to the heterogeneity of studies and measures used, a meta-analysis could not be conducted. As a result risk factors were pooled for analysis and discussion.
Results Of the 5842 potentially relevant studies, 7 high-quality studies were included in this review. Results demonstrated that previous groin/hip injury was the most prominent risk factor, identified across four studies (OR range from 2.6 (95% CI 1.1 to 6.11) to 7.3, (p=0.001)), followed by older age (OR 0.9, p=0.05) and weak adductor muscles (OR 4.28, 95% CI 1.31 to 14.0, p=0.02) each identified in two studies. Eight other significant risk factors were identified once across the included studies.
Conclusions 11 significant risk factors for groin/hip injury for FBS players were identified. The most prominent risk factor identified was previous groin/hip injury. Future research should include a prospective study of a group of FBS players to confirm a relationship between the risk factors identified and development of groin/hip injuries.
- Sporting Injuries
- Injury Prevention
- Groin Injuries
- Hip Disorder
Statistics from Altmetric.com
Introduction
Sports injury risk factors are defined as entities that contribute to the occurrence of athletic injury.1 They can be considered intrinsic or extrinsic to the individual as well as modifiable or non-modifiable.2 Intrinsic risk factors are person-related (eg, age), while extrinsic are environment related (eg, playing surface).3 Modifiable risk factors can be altered to reduce injury rates (eg, strength), through the use of injury prevention strategies.1 ,2 Alternatively, non-modifiable risk factors cannot be altered to reduce injury rates (eg, previous injury).1 ,2
A UEFA prospective injury study defined a groin/hip as “Injury located to the hip joint or surrounding soft tissues or at the junction between the anteromedial part of the thigh, including the proximal part of the adductor muscle bellies…leading to a player being unable to fully participate in future training or match play.”4 Groin/hip injuries are common in the athletic population, particularly in sports requiring kicking, sudden changes in direction, twisting, turning and rapid acceleration and deceleration.5 Such biomechanics are central in field-based sports (FBS). These biomechanical requirements, in addition to the axial and rotational loads of 12 times player's body weight experienced during competition,6 could explain the high incidence of groin/hip injuries in this population. Groin/hip injuries have been studied across the sporting population and encompass: skeletal (pubic bone stress fracture, femoral fractures, avulsion injuries and bony bruising), articular (labral tears, osteitis-pubis and femoral-acetabular impingement), soft tissue (muscular strains/tendinopathies, bursitis, inguinal/sports hernia) and others (hip haematoma, neural, referred pain and tumors).2 ,5 ,7 The complexity of the diagnosis in groin/hip injuries creates a difficult rehabilitation prospect.
The incidence of groin/hip injuries is considerable in FBS. Chronic hip, buttock and groin pain account for 10% of all attendances to sports medicine centres.8 Groin injuries account for 2–5% of all sports injuries9 and are among the top six most commonly cited injuries in Rugby Union (RU).10 As the prevalence of these injuries has increased since 2002 they have moved from 16th to 4th place in most common training injuries in the Rugby Football Union annual audit.11 An incidence of groin injuries as high as 23% has been reported over two consecutive seasons in a study of Rugby League players.12 An incidence of 24% of chronic groin pain was reported in academy level Gaelic footballers last year.13 Chronic groin pain is the second most common problem within the sport.13 Hawkins and Fuller14 reported 41% of all soccer injuries are muscular strains, with 31% of these being groin strains. In the Australian Football League the incidence of new groin/hip injuries over a 3-year period was 10%, with an incidence of 17% of all match injuries.15 An epidemiological study of the National American Football League training camps found an incidence of groin strain injuries to be 0.7/1000 practice-hours and 1.63/1000 game-hours, over a 9-year period.16 These figures across the international sporting population represent the importance of identifying groin/hip injury risk factors as the first step of injury prevention.
Understanding the individual risk factors for groin/hip injuries for players participating in FBS that utilise similar playing biomechanics17 ,18 is important as a basis to develop injury prevention measures.3 For the purpose of this review FBS include; Football/Soccer (referred to as Soccer), Rugby League and Union, Australian Rules Football (ARF), American Football (AF), Gaelic Football, Hurling and Field Hockey.
A previous systematic review2 identified previous injury, greater abductor to adductor strength ratios, sports specificity training, preseason sports-specific training as individual risk factors for groin strain injury. However, that review did not focus on a specific sporting population or specific study design. It reviewed both a painful and pain-free population, including current, long-term and previous groin injuries and injury interventions. Caudill et al19 systematically reviewed risk factors for sports hernias, but again failed to focus on a specific sporting group with similar playing biomechanics. Thus the aim of this review was to concentrate on a specific sporting group, that is, FBS, and to systematically review the risk factors for groin/hip injuries in this population.
Methods
This study was conducted according to the PRISMA guidelines.20
Eligibility criteria
The inclusion and exclusion criteria were developed by the lead reviewer.
Inclusion criteria
Studies were included if they investigated one or more risk factors and related them to the incidence of groin/hip injuries in FBS. Studies must have taken place over at least one FBS playing season. Owing to the diversity of definitions for groin/hip injuries or risk for injury, synonyms of such were accepted. Only studies written in English (as translation service was unavailable) with access to full text were considered.
Exclusion criteria
Studies involving animals/cadavers. Studies examining players with current groin/hip injury and/or pain were excluded. Intervention studies were excluded.
Titles and abstracts of articles were reviewed by the lead reviewer using broad criteria including sport examined and study design. At this point, the second reviewer was involved in determining which studies should be obtained and viewed in full text. For final selection of studies, the full text was reviewed by both reviewers. Any disagreements were resolved by discussion, with the option of including a third reviewer (NDB). The final selected articles were quality assessed independently by the first and second reviewers.
Type of studies
Types of studies included were either prospective or retrospective cohort design.
Type of participants
Participants included across the studies were pain free athletes actively participating in an FBS. These FBS included: Rugby, Soccer, ARF, AF, Gaelic Football, Hurling and Field Hockey. Additionally, participants included in the studies were over the age of 18 at the time of data collection.
Information sources and search
Twelve electronic databases were searched. These databases included: AMED, CINAHL, Cochrane library, EMBASE, MEDLINE, Nursing and Allied Health Collection, OVID EBOOKS, PEDro, PubMed, Science Direct, SPORTSDiscus and Web of Science. Databases were searched from inception to February 2012 by the lead reviewer (JR). Reference and citation tracking was performed on included studies. Records were kept of the number of returned articles from each search. Databases were searched using a combination of keywords. These keywords were broken into categories to ensure an extensive search of participant population.
-
Category 1: ‘Field based sports’ ‘sports’.
-
Category 2: ‘Risk Factors’ ‘Association’.
-
Category 3: ‘Groin’ ‘Groin injury’ ‘adductor’ ‘Osteitis Pubis’ ‘Pubic bone stress’ ‘Hip’ ‘Labral tear’ ‘trochanteric bursa’ ‘Femoral neck stress fracture’.
This search strategy process was reviewed and reproduced by second reviewer (KMC). Please refer to online supplementary appendix 1 for an example of Science Direct search strategy and the results.
Study selection
Study selection was determined by whether studies met the predefined inclusion criteria. Study selection process is outlined in figure 1.

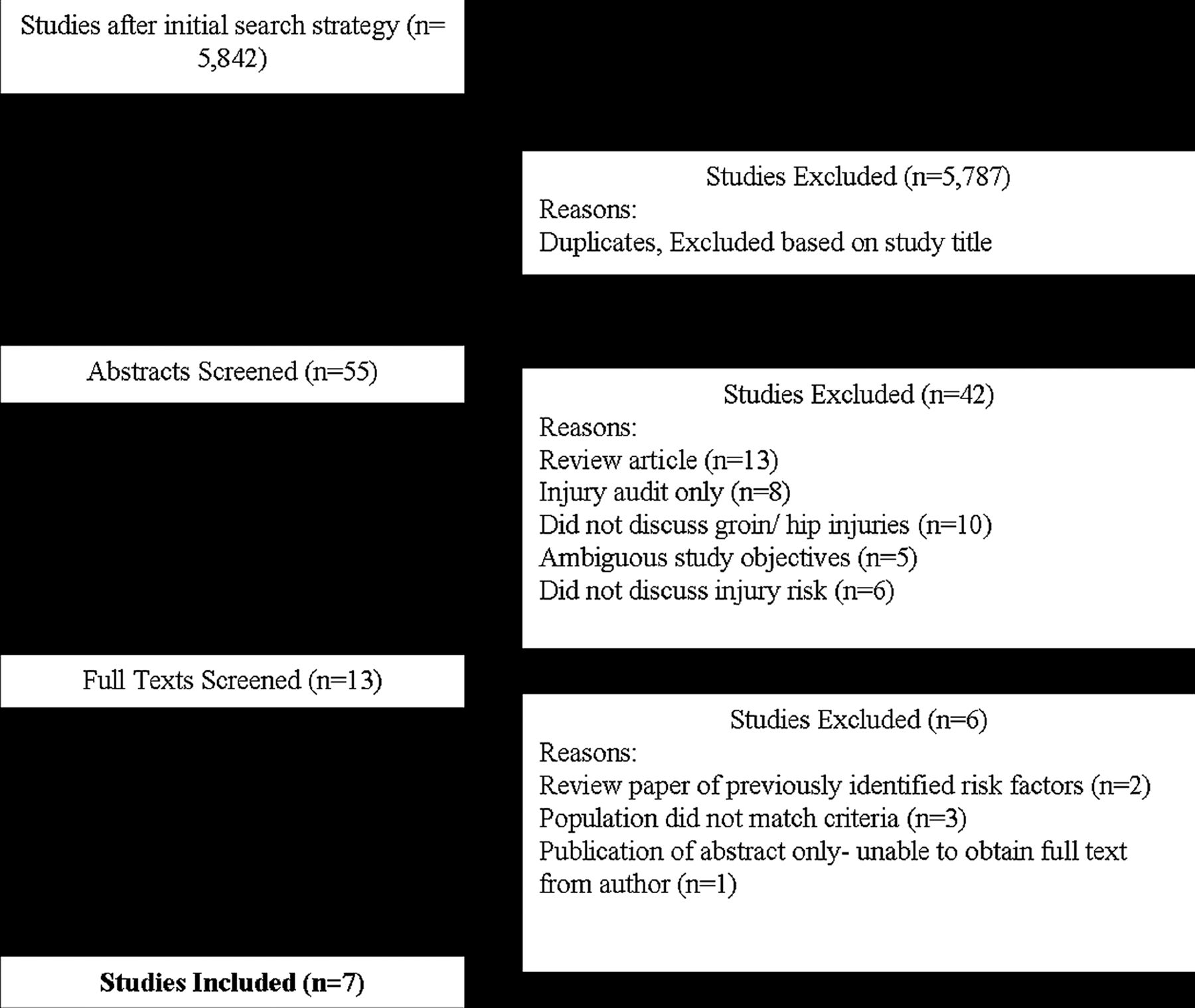{kind=link}
Flow chart of the study identification procedure.
Data collection process
A data collection table (tables 2 and 5) was predesigned based on a method employed in a previous systematic review.2 Reviewers collected the information separately and collated it.
Data items
Study characteristics were recorded under predefined headings including: FBS reviewed, prevalence of groin/hip injury, study design and aims, country where study took place, participant characteristics, definition of injury, risk factors examined, outcome measures used, statistical tests employed and significant risk factor identified.
Risk of bias in individual studies
Included studies were assessed using a modified CASP assessment tool (for Cohort study design; table 3). This tool assessed the risk of bias in individual studies.
Summary measures
Summary measures used to analyse risk of injury differed across all included papers. These measures included: ORs, incidence rate ratios, interclass coefficients, HR and number of injuries/1000 h of play.
Planned methods of analysis
Included studies were quality assessed using a 12-point modified CASP assessment tool (for Cohort study design) (table 3). Both reviewers (JR and KMC) practiced using this scoring tool on excluded studies to ensure marking accuracy. Both reviewers independently assessed and rated the included studies as ‘positive’ (scoring 1 point), ‘negative’ (no point) or ‘uncertain’. Any uncertainties were discussed and resolved with agreement of the awarded score. Owing to the heterogeneity of the risk factors examined, outcome measures used and risk factor analysis employed, the authors were unable to perform meta-analysis. The risk factors identified across the studies were pooled and analysed together to identify the most common groin/hip injury risk factors in FBS.
Results
Identification of studies
The initial search yielded 5842 potentially relevant papers (table 1). After duplicates and studies which did not match inclusion criteria (eg, intervention studies, population outside of criteria) were excluded, 55 papers remained. Subsequent to both reviewers independently evaluating these abstracts the number of papers was narrowed to 13. This was narrowed to seven after reading the full text and a discussion meeting between reviewers. Both reviewers deemed these seven papers3 ,5 ,12 ,21–24 appropriate to be quality assessed (figure 1). Searching the reference lists of these papers did not yield any additional results. The selection procedure is outlined in figure 1.
Number of papers yielded from initial literature search
Description of the included studies
Description of injury incidence, population examined and study origin is presented in table 2. The authors could not draw a mean figure for groin/hip injury incidence across the studies due to the heterogeneity of injury incidence description found (table 2). Populations studied were entirely men. Sporting population examined included soccer, ARF and rugby, from Australia, France, Iceland, Norway and Sweden. Participant numbers range from 50822 to 2924 with a mean of 267 and a total of 1875 participants. Player experience ranged from ‘amateur’ to ‘elite’. All seven studies had a follow-up of at least one playing season with one study following through a 10-year period.
Injury incidence in FBS studies reviewed
Methodological quality
All seven studies were quality assessed by both reviewers using a 12-point quality score-(table 3).
Quality assessment criteria score
This is a modified version of the CASP guidelines (a valid and reliable quality assessment tool) designed for this systematic review, based on an approach by Lankhorst et al.25 The methodological quality of 6/7 studies rated were 11/12, with a single study scoring 10/12 (table 4). The consistent area in which all the studies failed to achieve a score was ‘clearly defined inclusion criteria’. There was full agreement between rates on study quality, therefore no further statistical analysis was required.
Quality score of the reviewed studies (Y=yes, N=no)
Risk factor characteristics
As stated, risk factors can be identified as intrinsic or extrinsic to the player and further recognised as modifiable or non-modifiable.2 There was a combination of intrinsic, modifiable and non-modifiable risk factors assessed across the studies included in this review-(table 5).
Characteristics of included studies
Description of results
Data extracted from these studies (including risk factors examined and identified, outcome measures used, statistical results and sample sizes) is summarised in table 5. Non-modifiable risk factors for groin/hip injury in FBS identified included previous injury, age, age of maturation and small dominant femur diameter.
Previous injury was the highest reported risk factor for groin/hip injuries (n=4/7studies).3 ,5 ,21 ,24 Previous groin injury was identified as a significant risk factor for soccer3 ,21 and ARF players.5 ,24 Soccer players risk is reported to be 2.6 (95% CI 1.1 to 6.11) to 7.3 (p=0.001) times greater if they had a previous groin/hip injury.3 ,21 Older age was the second most prevalent non-modifiable risk factor (n=2/7 studies), in soccer (OR 0.9, p=0.05)3 and rugby league (p<0.05)12 populations. One study found that soccer players were at increased risk of a groin/hip injury if they were an early maturer (p=0.002).23 Similarly, smaller dominant femur diameter (WL 0.89, p=0.001) was identified as a significant risk factor for groin injuries in a rugby league study.12
Six modifiable risk factors3 ,12 ,21 ,23 for groin/hip injury in FBS were identified in this systematic review. The risk factor of body mass (BM)/weight (both measured in kg thus will be referred asBM) was the joint third most common risk factor identified (n=2/7 studies).12 ,24 O'Connor12 identified increased BM (WL 0.96, p<0.05) as a risk factor for rugby players in sustaining a groin injury (injured 90.5±9.5 kg vs non-injured 84.7±10.2 kg). Conflicting with these results, Verrall et al24 stated that a lower BM (incident rate ratio (IRR)=0.92 95% CI 0.87 to 0.97, p=0.004) (injured 72.50±3.28 kg vs non-injured 84.92±1.99 kg) was a significant risk factor for groin injury in ARF players. Weak hip adductor muscles (WHAM) is the other third most common risk factor identified for groin/hip injuries in this review (n=2/7).12 ,21 Engebretsen et al21 found that weak adductors was a significant risk factor (OR 4.28 95% CI 1.31 to 14.0, p=0.02) for groin/hip injury in a soccer population. Decreased hip Abduction (Abd) (OR 0.9, p=0.05)3 and total hip range of motion (ROM; IRR 0.9, 95% CI 0.83 to 0.99, p=0.03)24 were each identified once, in different studies, as a significant risk factor for groin/hip injuries in FBS. The final modifiable risk factors identified was a combination of Abd and Adduction (Add)-with-rotation peak torque (WL 0.94, p=0.02) strength ratio of hip muscle groups, angle of Add and Abd-with-rotation peak torque (WL 0.76, p<0.001) and bilateral difference in extension peak torque.12
Discussion
This systematic review examined risk factors for groin/hip injury in FBS. Eleven groin/hip injury risk factors were identified. The key findings recognised in this review were: previous groin/hip injury was the most prominent risk factor identified in four studies,3 ,5 ,21 ,24 followed by older age3 ,12 and weak adductor muscles12 ,21 each identified in two studies. Other significant risk factors identified once across the included studies are: early maturing players,23 smaller dominant femur diameter,12 increased/decreased BM,12 ,24 decreased hip abduction ROM3 and total hip rotation ROM24 and Abd and Add-with-rotation peak torque,12 strength ratio of hip muscle groups12 and bilateral difference in extension peak torque.12 All seven studies in this systematic review scored highly in quality assessment. An important finding was that six of the seven studies were prospective in design (table 5), reinforcing the validity of the results and eliminating recall bias.
Non-modifiable risk factors
The most prominent risk factor for groin/hip injuries identified in this review, and across the literature, was player history of a previous injury.2 ,3 ,5 ,21 ,22 ,26 The largest cohort study to date of male soccer players found previously injured players were at seven times greater risk of sustaining new groin injury than their non-injured counterparts.3 ARF players have six times greater risk of sustaining a groin/hip injury if they had a history of a previous groin/hip injury than those without.5 In ARF 32% of adductor strain injuries were reported as recurrent injury27 while this figure was as high as 44% in the ice hockey28 population. Causative factors for groin/hip injuries in FBS population may include both intrinsic (ie, muscle strength21) and extrinsic (field conditions1) risk factors. There may also be clinical reasons for player's history of previous injury making them more at risk of another groin/hip injury. These include: remaining deficits in physical conditioning, scar tissue formation, inadequate rehabilitation, reduced proprioception, altered movement patterns or premature early return to play after the initial injury and the number of times the player has sustained this type of injury.22 ,29 ,30 Previous history of groin/hip injury has not yet been identified as a risk factor in an RU population study, nor has the OR risk been calculated for those with such a risk factor.
The second most prominent, non-modifiable risk factor was older age.3 ,12 As the players age their body's collagen tissue changes in nature becoming less elastic and less able to absorb forces.31 ,32 This then results in the tissues being less adaptable to respond to quick force changes (characteristic of the biomechanics involved in FBS) or recover from fatigue.31 ,32 This hypothesis was supported by a study by Johnson et al33 which stated that abduction to adduction torque significantly decreases with advancing age. The physiological evidence for increasing age as a risk factor for injuries cannot be disputed.31–33 Of the seven studies examined in this systematic review two3 ,12 support the argument that increasing age was a risk factor for players in sustaining a groin/hip injury. Four studies5 ,21 ,23 ,24 did not examine increasing age as a risk factor for groin/hip injury. One study22 did not support the argument, as significant results were not found in their study. The authors22 did acknowledge that analytical methods differed to the study by Arnason et al3 which may explain the discrepancy in results.
An atypical groin/hip injury risk factor identified in this systematic review was that early maturing football players have a greater probability of sustaining a groin/hip injury.23 This risk factor was identified in only one study23 which examined chronological and skeletal age in relation to injury incidence and severity in soccer over a 10-season study period. This finding was also supported by the work of Backous et al34 and Linder et al35 These studies found that a higher rate of sports injury was established in the more mature soccer players, who were also found to be muscularly weak.34 ,35 Furthermore there was a direct correlation observed between advanced sexual maturity and injury incidence in ARF players.23 The hypothesis behind this risk factor was that, although players may be chronologically the same age as their playing counterparts, skeletally they were ‘older’ and thus at increased risk of a groin/hip injury, as discussed previously.
The final non-modifiable injury risk factor identified was that players with a smaller dominant femur diameter were at increased risk of injury.12 The author speculated that a smaller dominant femur diameter may alter the origin and insertion point of the adductor longus, which may alter the muscle efficiency. Furthermore this anatomical change may alter the muscle's ability to generate force and cope with stress.12 This explanation was currently a hypothesis and warrants further investigation for confirmation.
Modifiable risk factors
The most prominent modifiable risk factors were BM and WHAM (table 5), both identified in 2/7 studies.
WHAM was identified as a risk factor for groin/hip injuries in FBS in 2/7 studies in this review.12 ,21 Engebretsen et al21 stated that soccer players with WHAM have a four times greater risk of sustaining a groin injury compared to those without weakened musculature. This was supported by O'Connor12 whose study demonstrated that non-injured players had higher peak torques in hip adduction compared to those that sustained an injury. While the evidence for WHAM as an injury risk factor in FBS is limited it is well established within ice hockey literature. Emery26 stated that reduced muscle strength was a risk factor for acute muscle strains in ice hockey players. Tyler et al28 evaluated hip adductor strength in 47 ice hockey players and found that muscle strength was 18% lower in the players who sustained an adductor injury. The authors hypothesised that the cause of injury was related to eccentric loading of the adductors when decelerating during strid.28 While FBS place differing demands on players, they share high levels of acceleration and deceleration to ice hockey, suggesting a similar need for balanced hip muscle strength to resist injury.
Within the literature there was conflicting evidence regarding increased or decreased BM as a risk factor for groin/hip injuries in FBS players. O'Connor12 argued that a higher BM in conjunction with smaller dominant femur diameter places Rugby League players at a statistically significant risk for sustaining a groin injury. In contrast Verrall et al24 stated that ARF players with a lower BM have a greater risk of injury than their team-mates. Examining these studies individually highlights some methodological differences. First, there were 100 participants in O'Connor's study, which was a good representation of the population group. The results demonstrate that those with lower BM remain uninjured (p<0.05) and those of higher BM are at greater risk of injury (p=0.058). Increased BM was also supported as a risk factor for injuries in RU players in the New Zealand rugby injury and performance project.36 In comparison to O'Connor,12 only 29 ARF players participated in the study by Verrall et al.24 This sample size was a low representation of this population and lowers the external validity of the study. Additionally, authors based their results and analysis on only four players developing a chronic groin injury as result of low BM. The small sample size may reduce our confidence in the findings of this study.24 Authors express that increased risk occurs in athletes who were lighter as they were unable to meet the extensive aerobic demands of ARF.24 However they stated it was difficult to account for the finding of decreased BM being associated with development of chronic groin injury.24 Thus, on the weight of the current literature,12 ,24 the more robust argument was that increased BM places FBS players at risk of a groin/hip injury during the playing season.
Hip abduction ROM and total hip rotation ROM have both been identified in individual studies as a significant risk factor for groin/hip injury in soccer and ARF players, respectively.3 ,24 Arnason et al3 found that players with reduced hip abduction ROM had a significant risk of sustaining a groin injury. These results were supported by earlier work of Ekstrand and Gillquist37 who demonstrated that soccer players, who had less hip abduction than the control group, were more at risk of a groin injury. The biomechanics and intensity of the sport place a high demand on the hip musculature and could result in muscle tightness and injury.5 Gabbe et al5 stated that synergistic and opposing muscle length or ROM may cause strain on adductors leading to injury. Decreased abduction ROM was supported as a groin/hip injury risk factor in soccer with further studies warranted to confirmation it as a risk factor across FBS.
Total hip rotation (internal and external) ROM has been identified as a risk factor for ARF players in sustaining a groin/hip injury throughout playing season. Authors stated that players with lower total hip rotation ROM at the start of the season were more likely to subsequently develop a chronic groin injury.24 It has been highlighted already that this study had a small population size and subsequently the results may not be completely reliable. These results were somewhat supported by Verrall et al38 who propose that players activity in ARF could lead to a capsular response, with subsequent restriction of hip ROM, biomechanically disadvantaging the athlete and making them more vulnerable to injury. To conclude that decreased total hip ROM was a significant risk factor for groin/hip injuries across FBS, more high-quality studies were required.
The final intrinsic modifiable variable identified was the ratio of strength forces of muscles (more specifically hip adductors vs abductors) acting on and around the hip joint.12 O'Connor12 found peak torque differences in non-dominant limb adduction and abduction with rotation and bilateral difference in extension peak torque between injured and non-injured rugby league players. These results became part of the author's variable list in determining whether players were predisposed to groin/hip injury. Merrifield and Cowan39 support the argument that strength ratio differences acting in and around the hip joint increases a players risk of injury. Authors stated that a strength imbalance of greater than 25% was identified in players prone to adductor strains. The importance of these strength balances has been a long-standing theory, with research published in 1987 highlighting that the failure of these stabilising and propulsive muscles was resultant in adductor strain injuries.40 This theory is also supported by a study which identified that once high-performance athletes sustained an adductor muscle strain, the player may be at increased risk of rectus strain or athletic pubalgia due to an imbalance of forces across the anterior hip musculature.41 Furthermore, an investigation of the ice hockey population found that adduction strength was 95% of abduction strength in the uninjured players versus injured athletes adduction strength was only 78% of abduction strength.28 Authors concluded that those hockey players with an adductor-to-abductor strength ratio of less than 80% were 17 times more likely to sustain a groin injury.28 Although these figures were in reference to ice hockey players (the biomechanics of which are different to FBS) this information has transferability across populations with regard to injury prevention. As strength ratio differences was only identified as part of a list of groin/hip injury risk factors in one FBS study,12 confirmation is needed as to whether it is a stand-alone groin/hip injury risk factor for players participating in FBS.
Limitations of this review
Despite the excellent quality of the literature examined (table 2) several limitations must be identified. First, due to the heterogeneity of the studies included (especially the methodology employed) it was not possible to perform statistical or meta-analysis of the results. The different definitions of injury, risk factors examined and how they were examined across the studies resulted in risk factors being pooled and discussed together.
A second limitation was that any studies outside the English language were excluded from this systematic review, which may have limited the risk factors identified. Third, all the included studies were lacking clearly defined inclusion/exclusion criteria. Although the population in each study was clearly defined using playing experience and anthropometric data, the absence of inclusion and exclusion criteria inhibits study reproducibility. While all the studies provided height and weight means of the investigated population group, none examined BM index in terms of injury occurrence. This extra variable may have been identified as a significant as a risk factor for groin/hip injuries in FBS players.
Three of the seven studies analysed did not have a control group.5 ,22 ,23 This was not a requirement for quality assessment as authors felt studies investigating injury risk factors (based on variables such as injury incidence and duration) should not require comparison to a control group. For example; Le Gall et al23 examined the effects of early versus late maturers and their risk of injury. A control group for such a study was not warranted unless the authors wanted to compare the injury incidence to another soccer group or FBS. A final methodological limitation was that, although studies examined in this review followed players through the season with regard injury status and training/match exposure, they have only tested player's objective outcome measures once during the playing season.3 ,12 ,21 It would be incorrect to assume that player's strength, ROM, flexibility and so forth do not change as injury occurrence, fatigue and extrinsic risk factors ensue during the playing season.
Additionally it should be acknowledged that the CASP quality appraisal tool is limited in its specificity in scoring studies. For example, it does not give account for specific methodological factors such as sample size therefore studies may get an inflated quality score. Lastly, a notable absence in this systematic review was the investigation of external/extrinsic factors, such as weather conditions, playing and training surfaces, lengths of training and boot styles on FBS player's risk of injury. A previous review also observed this fact and suggested that future studies investigating extrinsic risk factors were essential.2
Conclusion
Only seven papers matched the inclusion criteria and were quality assessed in search of risk factors for groin/hip injuries in FBS. In order of prominence, risk factors identified were: previous injury, older age, BM, WHAM, biologically early maturating players, smaller dominant femur diameter, decreased hip abduction ROM and total hip rotation ROM and strength ratios of hip muscle groups (hip abduction and adduction-with-rotation peak torque and bilateral difference in extension peak torque). These groin/hip injury risk factors were identified, reasoned and discussed with reference to the current research in the field. Limitations of this systematic review were identified, the most prominent of which being the heterogeneity of the studies disallowing meta-analysis. Future research should focus on confirming the less supported groin/hip injury risk factors in an FBS population. This may be achieved by compiling subjective, objective and functional outcome measures as part of a testing procedure in an FBS population. This would be of particular importance in a rugby player-based population, based on the incidence of groin/hip injuries highlighted previously. Using these tests on the same group of players through a playing season and comparing the results in relation to groin/hip injury status, would confirm or negating these groin/hip injury risk factors in a rugby population.
What are the new findings?
-
This review identified 11 risk factors for groin/hip injury in Field-Based Sports (FBS).
-
This review documented limitations and shortcomings in the current field of literature regarding the examination of groin/hip injury risk in FBS.
-
This review highlighted the need for a uniform definition of what a groin/hip injury is.
-
This review highlights areas for future research in the field of groin/hip injuries in FBS.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors JR, KMC and NDB were all involved in conception and design. JR and KMC independently reviewed the literature. JR extracted the studies data. JR and KMC were involved in rating the literature, with NDB acting as third party to arbitrate any disagreements in ratings. JR was the primary author in preparing the manuscript for publication, with KMC and NDB reviewing the document prior to submission.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.