Article Text

Abstract
Background This study aimed to describe chondropathy prevalence in adults who had undergone hip arthroscopy for hip pain. The relationships between chondropathy severity and (1) participant characteristics; and (2) patient-reported outcomes (PROs) at initial assessment (∼18 months postsurgery) and over a further 12 months (∼30 months postsurgery) were evaluated. Finally, the relationships between chondropathy and coexisting femoroacetabular impingement (FAI) and labral pathology at the time of surgery were evaluated.
Methods 100 consecutive patients (36±12 years) who underwent hip arthroscopy 18 months previously participated. Hip Osteoarthritis and Disability Outcome Score (HOOS) and International Hip Outcome Tool (iHOT-33) data were collected prospectively at 18 months postsurgery and at 30 months postsurgery. Surgical data were collected retrospectively. Participants were grouped: Outerbridge grade 0, no chondropathy; Outerbridge grade I–II, mild chondropathy; Outerbridge III–IV, severe chondropathy. The presence of FAI or labral pathology was noted.
Results The prevalence of chondropathy (≥grade I) at hip arthroscopy was 72%. Participants with severe chondropathy were significantly worse for all HOOS subscales and the iHOT-33 at 18 months postsurgery (HOOS-symptoms (p=0.017); HOOS-pain (p=0.024); HOOS-activity (p=0.009); HOOS-sport (p=0.004); HOOS-quality-of-life (p=0.006); iHOT-33 (p=0.013)) than those with no chondropathy. At 12-month follow-up, HOOS-quality-of-life in those without chondropathy was the only PRO that improved. Relative risk of coexisting chondropathy with labral pathology or FAI was 40%.
Conclusions Chondropathy was prevalent, and associated with increasing age, coexisting labral pathology or FAI. Severe chondropathy was associated with worse pain and function at 18 months postsurgery. Little improvements were observed in participants over a further 12 months, regardless of chondropathy status.
- Arthroscopic Surgery
- Hip disorder
- Osteoarthritis
Statistics from Altmetric.com
Background
Hip osteoarthritis (OA) is a significant cause of pain, stiffness and reduced function.1 ,2 It is evident in 11% of adults aged 55–64 years in the UK3 and is associated with considerable economic, health and personal costs.4 ,5 While the impact of hip OA has been evaluated in older populations,2 ,6 ,7 arthritis is not just a disease of the elderly. Approximately 31% of people in Australia with arthritis are aged less than 55 years,8 and 2.5% of people in Western Europe, North America, Japan and Australia aged between 45 and 59 years have OA.9 Therefore, a greater understanding of the impact of early-onset hip OA on pain, function and quality of life in younger people is warranted.
In recent years, hip arthroscopy has become commonplace,10 ,11 and aims to reduce pain and improve physical function associated with early hip OA, coexistent pathology, such as labral tears, and morphological variants including femoroacetabular impingement (FAI).12–14 Our recent systematic review14 concluded that the presence of chondropathy at the time of surgery appeared to result in poorer outcomes than for those with normal cartilage.
Importantly, hip arthroscopy allows for the identification of the early changes seen in hip OA, such as chondropathy,15 ,16 which cannot be visualised using radiographs. It also enables simultaneous assessment of FAI, labral pathology and coexisting chondropathy, and therefore may allow the relationship between these factors to be investigated. Considering that meniscal pathology at knee arthroscopy increases the relative risk of knee OA by 3–14 times,17 ,18 it is plausible that factors such as labral pathology14 ,19–21 may be associated with hip chondropathy. Furthermore, while FAI can predict the development of end-stage OA after 20 years,22 ,23 its relationship with hip chondropathy is less known. The early identification of chondral changes seen in hip OA may provide an opportunity to study the natural history and progression of the disease,24 thus facilitating treatment strategies to modify disease progression.
The primary aim of this study was to describe the prevalence of chondropathy (a marker of early-onset hip OA) in a cohort of young and middle-aged adults who had undergone hip arthroscopy for hip pain. Additional aims were to evaluate the relationship between chondropathy severity and (1) participant characteristics; and (2) patient-reported outcomes (PROs) at 18 months postsurgery and over a further 12 months (∼30 months postsurgery). Finally, the relationships between chondropathy and coexisting FAI and labral pathology were evaluated.
Methods
Study design
This cross-sectional and prospective longitudinal cohort study was undertaken in a community setting.
Participants
The database of a single orthopaedic surgeon (MGP) was accessed, with consecutive patients who were aged between 18 and 60 years, and who underwent hip arthroscopy for painful intra-articular hip pathology between January 2009 and July 2011, invited to participate. Invitations were sent when patients were between 12 and 24 months postsurgery (figure 1). Participants who were unable to walk without assistance, to speak or read English, had converted to total hip arthroplasty, had undergone further hip or other surgery or had another concurrent lower limb injury were excluded. All participants completed written informed consent prior to participating in the study.

Results of patient recruitment. THA, total hip arthroplasty.
Procedures
Hip arthroscopy was performed by the single surgeon (MGP), who is a high volume fellowship-trained hip arthroscopist. Arthroscopy was performed in the lateral decubitus position with the limb in hip abduction and slight flexion. Traction was applied in the direction of the femoral neck using a padded boot with a bolster situated between the legs. Entry to the central and peripheral compartments of the hip was performed with a 70° arthroscope via a viewing mid-trochanteric portal, and an instrument anterior trochanteric portal.25 Assessment of intra-articular pathology, including the presence of chondropathy, FAI and labral pathology, was conducted using a standardised and systematic technique.
Collection of initial clinical and PRO data was prospective and took place 12–24 months (mean 18±3 months) postsurgery in a private physiotherapy clinic by a single investigator (JLK). Questionnaire data included the Hip Osteoarthritis and Disability Outcome Score (HOOS)26 and the International Hip Outcome Tool (iHOT-33),27 which are the most appropriate PROs for use in this population.28 Baseline participant information was collected and body mass index (BMI) was calculated. Information regarding time since surgery and presence of FAI, labral pathology and/or chondropathy at surgery was recorded retrospectively from surgical notes. Collection of 12-month follow-up (∼30 months postsurgery) PRO data occurred via mail, where participants were posted PRO. The PROs were scored by a single investigator (JLK), who was blinded to participant identity and initial assessment scores.
Primary outcome measure
Hip chondropathy
The Outerbridge grading system was used to define chondral injury to the acetabulum or femoral head.29 Surgical intervention included chondral debridement or microfracture as deemed appropriate by the surgeon. Participants were grouped as: those who had grade I or II chondropathy (mild chondropathy group); those who had grade III or IV chondropathy (severe chondropathy group); and those who did not have chondropathy (no chondropathy group).30
Secondary measures
Patient-reported outcomes
The HOOS26 and the iHOT-3327 PROs were used to assess the participant's symptoms. The HOOS has five subscales, those being symptoms and stiffness (HOOS-S), pain (HOOS-P), activities of daily living (HOOS-A), sport and recreation (HOOS-Sp) and quality-of-life (HOOS-Q), while the iHOT-33 is an aggregate score of all domains. Each subscale of the HOOS and the iHOT-33 has a maximum score of 100 points (best possible outcome).
FAI and labral pathology
The presence of FAI was a clinical diagnosis performed by the surgeon (MGP) based on the presence of each of the three main criteria: (1) radiological signs of FAI: from α angle measurement for cam-type impingement using Dunn view radiographs31 and measurements of the centre edge angle of Wiberg and acetabular retroversion (crossover sign) using anteroposterior pelvic radiographs for pincer impingement;32 (2) positive impingement tests in preoperative clinical examination that included hip internal rotation at 90° hip flexion33 and hip flexion measured in supine34 and (3) the presence of a cam or a pincer lesion noted at surgery.35 Surgical intervention for FAI included femoral osteoplasty or acetabular osteoplasty as deemed appropriate by the surgeon. The presence of a labral tear was defined as one that was severe enough to require surgical intervention (including labral debridement or repair), which is consistent with published definitions.35 ,36 Patients may have had multiple surgical interventions in a single arthroscopy for one or more of chondropathy, FAI or labral pathology if these pathologies coexisted, as deemed to be appropriate by the surgeon.
Data management and statistical analysis
Statistical analyses were performed using SPSS V.20.0 software (SPSS Inc, Chicago, Illinois, USA). Between-group differences in participant characteristics were compared using independent t tests or χ² as appropriate. One-way analyses of covariance (ANCOVA) were conducted to evaluate the relationship between the three chondropathy groups and the PROs, with covariates of age, gender and BMI utilised. Repeated measures analyses of variance were conducted to evaluate within-group change between the 18-month and 30-month postoperative follow-up time points for each of the three chondropathy groups. The percentage of participants who improved between the 18-month and 30-month postoperative follow-up time points by at least the previously reported minimal important change (MIC) of each PRO28 was calculated. The relative risk (95% CIs) of having hip chondropathy with coexisting labral pathology and FAI was calculated. The sensitivity and specificity of labral pathology and FAI associated with chondropathy were determined. Significance for all analyses was set a priori at p<0.05.
Results
The flow of participant recruitment is outlined in figure 1. Briefly, between January 2009 and July 2011, 355 patients underwent hip arthroscopy with a single surgeon. Of these, 334 patients fulfilled the inclusion criteria. A total of 152 patients responded to an invitation to participate in the study. Fifty-two were excluded because they were not able to attend the initial assessment; or they had further surgery or other injuries precluding their involvement. One hundred patients fulfilled the eligibility criteria, consented to participate and were included in the study cohort (figure 1).
Seventy-two of 100 patients had chondropathy at hip arthroscopy. Of these, 44 patients (61%) had mild chondropathy (Outerbridge grade I–II) while 28 (39%) had severe chondropathy (Outerbridge III–IV). Participant baseline characteristics, including differences between chondropathy groups, are summarised in table 1. In addition, when stratified according to age and gender, the data demonstrated that the prevalence of chondropathy increased with age. Prevalence ranged from 61% of participants aged between 18 and 35 years, to 100% of participants aged over 50 years (figure 2).
Baseline characteristics—chondropathy versus no chondropathy groups

Age-related prevalence of chondropathy in males and females.
The results of ANCOVA analyses of PROs between chondropathy groups at 18-month postoperative assessment are contained in figure 3. Significant between-group differences were observed for all PRO subscales (HOOS-S, p=0.017; HOOS-P, p=0.024; HOOS-A, p=0.009; HOOS-Sp, p=0.004; HOOS-Q, p=0.006; iHOT-33, p=0.013). Results of post hoc analyses indicate that participants with severe chondropathy had worse PRO scores than those without chondropathy in the: HOOS-S (mean difference (MD) 11, 95% CI (1 to 21), p=0.020); HOOS-A (MD 9 (0 to 18), p=0.042); HOOS-Q (MD 17 (4 to 29), p=0.014); and iHOT-33 (MD 12 (1 to 23), p=0.034). Those with severe chondropathy also have worse outcomes compared to those with mild chondropathy for the: HOOS-S (MD 12 (3 to 21), p=0.007); HOOS-P (MD 11 (3 to 19), p=0.007); HOOS-A (MD 12 (5 to 19), p=0.002); HOOS-Sp (MD 19 (8 to 30), p=0.001); HOOS-Q (MD 19 (7 to 31), p=0.002); and iHOT-33 (MD 15 (5 to 25), p=0.004). There were no differences in PROs between those with no chondropathy and those with mild chondropathy (figure 3).
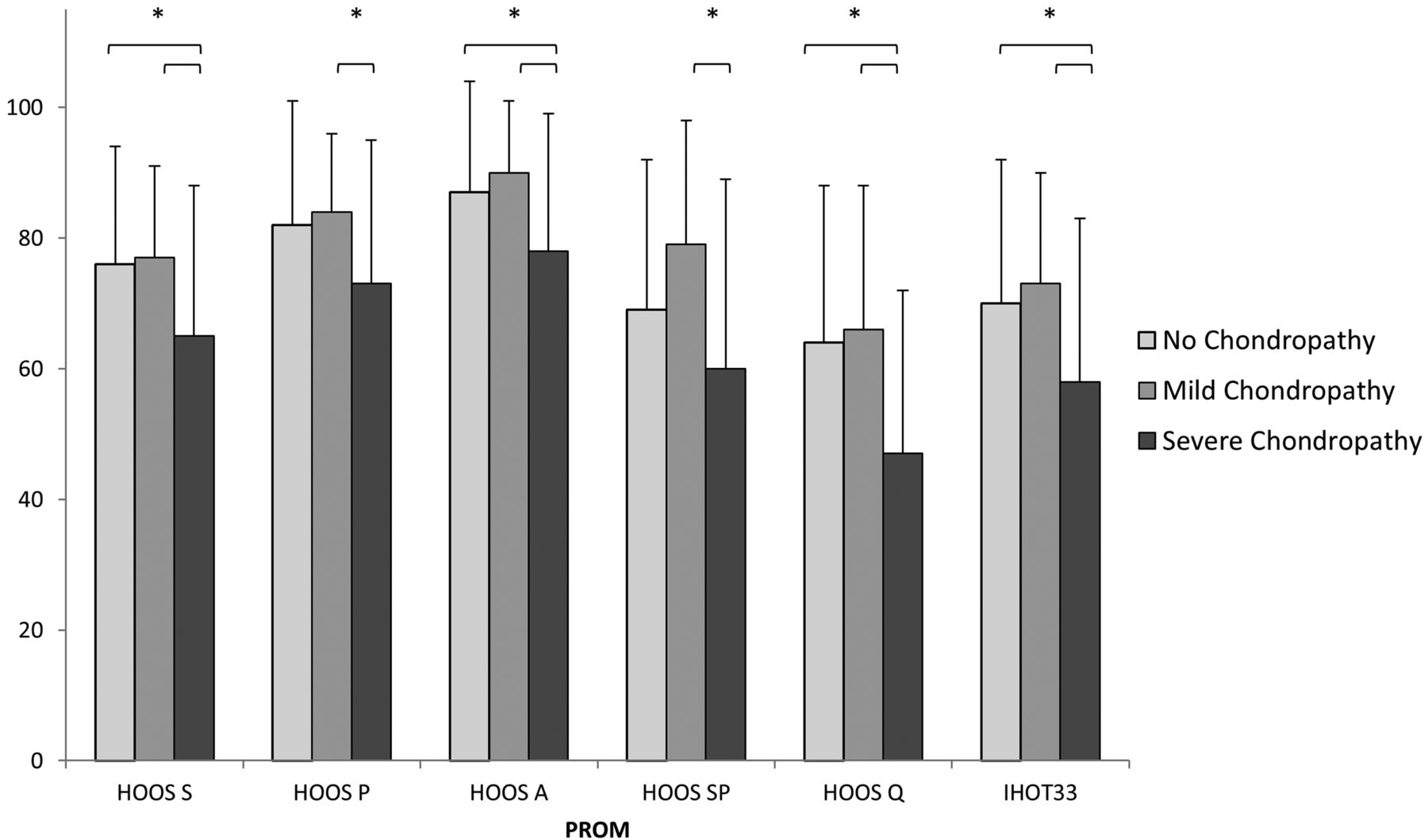
Results of patient-reported outcome measures at 18 months postoperative between chondropathy groups. *, significant post hoc finding (p<0.05); A, activity of daily living subscale; HOOS, Hip Osteoarthritis and Disability Outcome Score; iHOT-33, International Hip Outcome Tool; P, pain subscale; PROM, patient-reported outcome measure; Q, quality-of-life subscale; S, symptoms subscale; SP, sport subscale.
There were no significant within-group changes between the two postoperative time points for most PRO subscales (figure 4). The only significant improvement was in participants with no chondropathy for HOOS-Q (MD 10 (2 to 18) points; p=0.009). The percentages of participants who improved by the previously reported MIC for each PRO are contained in table 2. Improvements seen ranged from 24% of participants for the HOOS-P and HOOS-A, to 35% for the HOOS-Sp.
Percentage of participants who improved by the MIC, compared to those who did not change or worsened, between the 18-month and 30-month postoperative time points
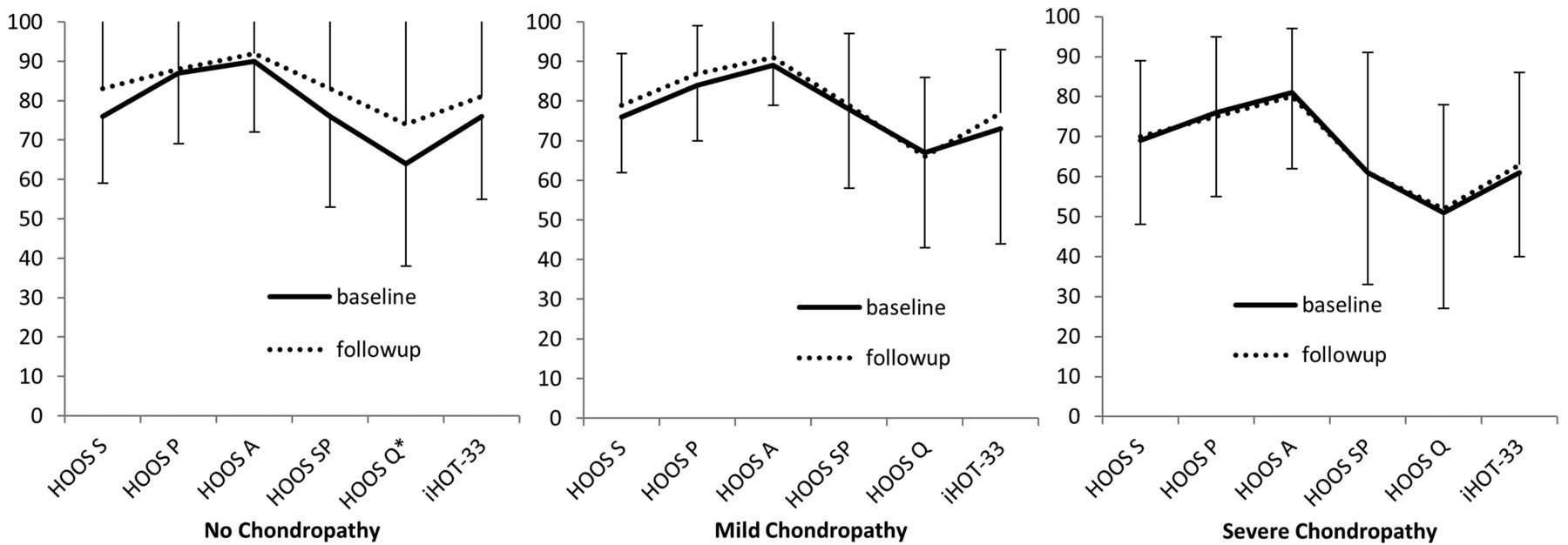
Results of change in patient-reported outcome measures for the different chondropathy groups. *, significant difference between baseline and follow-up (p=0.009); A, activity of daily living subscale; HOOS, Hip Osteoarthritis and Disability Outcome Score; iHOT-33, International Hip Outcome Tool; P, pain subscale; Q, quality-of-life subscale; S, symptoms subscale; SP, sport subscale.
The prevalence of coexisting hip pathology in the chondropathy group is presented in figure 5. The relative risk of concomitant chondropathy if labral pathology was present was 1.37 (95% CI 1.00 to 1.85); and it was 1.42 (95% CI 1.13 to 1.79) if FAI was present. The sensitivity of both labral pathology and FAI in predicting chondropathy was 80%. The specificity of labral pathology and FAI in predicting chondropathy was 42% and 35%, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Prevalence of chondropathy with coexisting pathology. FAI, femoroacetabular impingement.
Discussion
We observed that the majority of adults who had undergone hip arthroscopy for hip pain demonstrated chondropathy at surgery, and the prevalence of chondropathy increased with age. Severe chondropathy was associated with worse PRO scores at 12–24 months posthip arthroscopy, and the majority of PROs did not improve during the subsequent 12 months. Finally, the presence of FAI and labral pathology was associated with a 40% greater risk of concomitant chondropathy.
Importantly, our study indicates that chondropathy is common in most of an active (but not elite athletic) cohort of young and middle-aged people who have undergone hip arthroscopy. Notably, 61% of young adults aged between 18 and 35 years had hip chondropathy. Therefore, health practitioners may need to change the focus of treatment. Chondropathy appears to be a marker of early degenerative hip disease and treatment strategies should include those for the management of chronic disease, such as maintenance of physical activity and fitness, pain coping skills and weight management. Interestingly, we found that people with severe chondropathy performed more physical activity than those with mild chondropathy. It is possible that people with more severe disease have already undertaken strategies to manage their condition, such as modification of activity type to those which have lower impact and are less strenuous.
People with severe chondropathy recorded worse PRO scores at 18 months postarthroscopy than those with mild or no chondropathy. Our finding builds on those from systematic reviews14 ,37 ,38 and recent studies that report lower preoperative to postoperative improvements in those with severe chondropathy, compared to those with mild39 or no chondropathy.13 ,40 Since hip chondropathy at arthroscopy represents early-onset hip OA, it appears that those with more advanced chondropathy have progressed further along the disease continuum of hip OA. As severity of chondropathy increases, involvement in structures capable of generating nociception, such as the subchondral bone41 and the acetabular labrum,42 may also increase, creating a perception of greater pain and worse symptoms or function in these patients. The collection of PRO data by an independent researcher in a physiotherapy clinic, rather than a surgeon's rooms, may also explain the lower scores, as patients may be more likely to report higher scores when the data are collected by the treating surgeon.
Importantly, the PRO scores for all participants, regardless of chondropathy status, were considerably worse than those that we reported previously for healthy controls. In our previous paper, we reported PRO scores for the HOOS and iHOT-33 for healthy people aged 18–55 years. The difference between the scores in the current study, and those reported for healthy controls in the previous study, ranged from 10% for the HOOS-A in those without chondropathy to 50% for the HOOS-Q in those with severe chondropathy.28 In addition, the poor PROs after hip arthroscopy in the current study showed no evidence of resolution over a further 12-month period, except HOOS-Q, where people with no chondropathy reported a significant improvement. Furthermore, only one-quarter to one-third of all people undergoing hip arthroscopy continue to experience meaningful improvement (greater than the MIC) beyond 18 months, and remained worse than aged-matched healthy controls.28 Given these findings, it appears that better interventions are required to improve PROs at this postoperative time point in order to ensure optimal recovery.
Variations in hip morphology, including FAI, are associated with the development of hip OA.22 ,23 ,43–46 In the current study, 69% of participants with chondropathy had coexisting FAI or labral pathology. In addition, participants with labral pathology or FAI were approximately 40% more likely to also have chondropathy than those without. While further studies are required to determine if a similar relationship holds true with imaging such as MRI for labral or radiographs and CT scans for FAI,31 our findings suggest that clinicians can have a high degree of suspicion that individuals with hip pain and FAI or labral pathology may also have chondropathy.
We acknowledge some limitations in the current study. We recruited 100 participants out of a possible 334 eligible patients, creating a potential for selection bias. However, in the 234 participants who were not included in the current study, the prevalence of chondropathy was 74%, and participant age was 37 years, indicating that the included participants were likely to be representative of the whole sample. The lack of a non-surgical control group is a limitation. Future studies that include a non-surgical control may be conducted, when the non-surgical diagnosis of chondropathy becomes the gold standard. Second, we included a large age range, with the upper age limit being 60 years. The broad age range of the cohort increases the generalisability of the findings, but may reduce their specificity. In order to account for the influence of age, the between-group analysis was conducted with and without (results not presented) age as a covariate. There were no differences in our findings for each analysis. Our modest sample size is a limitation, and these findings need to be replicated in larger studies. Since the Outerbridge grading scale of cartilage defects was not originally reported for cartilage defects in the acetabulum,13 ,47 future studies could consider using grading systems established specifically for acetabular defects seen at hip arthroscopy.48 We did not perform additional subgroup analysis on each of the groups to determine the effect of types of surgical intervention, type of FAI or other coexisting pathology on outcomes, due to the sample size of this study.49 Future studies may examine these factors in patients with hip chondropathy to further our understanding of the impact of these factors in this patient group. The sample of patients included in this study may be subject to inclusion bias, as all had hip pain for which they had hip arthroscopy. However, the inclusion of a large range of pathology and the utilisation of a single surgeon performing the arthroscopy limit the effects of such bias on the results. Finally, we did not examine the preoperative PRO data.50 We chose to report PROs at 12–24 months postoperatively, as this is a time when recovery from surgery is generally considered to be complete, and follow these patients for a further 12 months to determine the natural history over this time.
In conclusion, this study documented the high prevalence of chondropathy (72%) in a young-to-middle-aged population undergoing hip arthroscopy, which increased with age. At 12–24 months postsurgery, participants with severe chondropathy had significantly poorer results in all PROs than those with mild chondropathy and those without chondropathy. Participants with no chondropathy were found to improve in quality-of-life scores at 12-month follow-up, but those with mild and severe chondropathy did not. Furthermore, the relative risk of those with labral pathology and FAI having chondropathy was 1.37 and 1.42, respectively. Considering the low PRO scores in those with chondropathy after hip arthroscopy, and the small number of patients improving beyond 18 months postoperatively, optimised rehabilitation regimens may need to be developed.
What are the new findings?
-
Chondropathy (a marker of early-onset hip osteoarthritis) was frequently observed in young and middle-aged adults undergoing hip arthroscopy.
-
Chondropathy was associated with increasing age, coexisting labral pathology and femoroacetabular impingement. Severe chondropathy was associated with worse patient-reported outcomes (PROs) at 18 months postsurgery.
-
The PRO scores were considerably lower than previously reported PRO scores in age-matched controls, at the time point (18 months postsurgery) when recovery is expected.
-
The PRO scores did not improve over the 12-month follow-up (30 months postsurgery), except that the absence of chondropathy was associated with improved quality of life.
How might it impact on clinical practice in the near future?
-
This information indicates a need to develop interventions with potential to improve patient-reported outcomes in people with hip chondropathy, particularly at a time point where recovery has been assumed to be complete.
-
Chondropathy appears to be a marker of early degenerative hip disease and treatment strategies should include those such as education, maintenance of physical activity and fitness, pain coping skills and weight management.
-
Clinicians can have a high degree of suspicion that individuals with hip pain and femoroacetabular impingement or labral pathology may also have chondropathy.
References
Footnotes
-
Contributors JLK designed the research question and study design, performed the data collection and data analysis, prepared the tables and figures and was involved in manuscript preparation. MM contributed to the study design, data processing and interpretation and was involved in manuscript preparation. AGS contributed to the study design and data interpretation and was involved in manuscript preparation. MGP contributed to participant recruitment and data interpretation and was involved in manuscript preparation. TCBP contributed to data interpretation and was also involved in manuscript preparation. KMC designed the research question and study design, performed the data analysis and was involved in manuscript preparation.
-
Funding This project was funded in part by the Australian Physiotherapy Research Foundation Beryl Haynes Memorial Grant T09-BH026.
-
Competing interests None.
-
Ethics approval The study was approved by the University of Melbourne Human Research Ethics Committee (HREC number 1033063) and the University of Queensland Medical Research Ethics Committee (MREC number 2012000708).
-
Provenance and peer review Not commissioned; externally peer reviewed.