Article Text

Abstract
Objective To compare the accuracy and efficacy of ultrasound (US)-guided injections versus landmark-guided injections of the subacromial space, biceps tendon sheath, acromioclavicular (AC) joint and glenohumeral (GH) joint.
Methods PubMed, Medline and Cochrane libraries were searched up to 31 July 2013. Two independent authors selected and evaluated randomised controlled trials comparing the accuracy and/or efficacy of US versus landmark-guided injection of the shoulder girdle. A meta-analysis of accuracy, pain Visual Analog Scale (VAS), function score and reported adverse events were performed.
Result Four cadaveric studies (300 cadaveric shoulders) and nine live human studies (514 patients) were reviewed. Based on three studies for AC joint, the accuracy of US versus a landmark-guided injection was 93.6% vs 68.2% (p<0.0001). Based on single studies, the accuracy of US versus a landmark-guided injection was 65% vs 70% for the subacromial space (p>0.05), 86.7% vs 26.7% for the biceps tendon sheath (p<0.05), and 92.5% vs 72.5% for the GH joint (p=0.025). Based on three studies for the subacromial space, the US group had a significantly greater reduction in pain (mean difference (MD)=1.47, 95% CI 1.0 to 1.93), and improvement in function (standardised MD=0.70, 95% CI 0.39 to 1.01) at 6 weeks postinjection. Based on a single study for the biceps tendon sheath, the US group had a significantly greater reduction in pain (MD 1.9, 95% CI 1.2 to 2.6) and improvement in function (MD=10.9, 95% CI 6.57 to 15.23).
Conclusions US-guided injections showed greater accuracy for all shoulder girdle injections, with the exception of the subacromial space. There was improved efficacy for the subacromial space and biceps tendon sheath injections.
- Intervention efficacy
- Shoulder
- Ultrasound
Statistics from Altmetric.com
Introduction
Shoulder pain has been identified as the third most common musculoskeletal symptom following back and knee pain.1 ,2 Rotator cuff, proximal long head of the biceps tendon, acromioclavicular (AC) joint, and glenohumeral (GH) joint disorders are considered the main sources of pain arising from the shoulder girdle.3 ,4 Although there has been a debate about the efficacy of local corticosteroid injections for patients with shoulder pain, corticosteroid injections are widely used for short-term pain relief and to facilitate the acute rehabilitation phase for patients with shoulder pain.5–9
Shoulder girdle injections have traditionally been done ‘blind’ (anatomical landmark guided injections); however, the use of image guidance (fluoroscopy or ultrasonography) has been shown to improve the accuracy of injections for different anatomical locations of the shoulder girdle.10 ,11 The increased accuracy of shoulder corticosteroid injections has been shown to correlate with improved efficacy.12 ,13 Additionally, ultrasound (US)-guided injections have become more popular because of the recent advances in image quality, decreased cost of use, portability and lack of radiation exposure.11 ,14 However, several studies raised concerns regarding the increased costs and the lack of significantly improved clinical efficacy with US-guided injections.15–17
The first systematic review that attempted to address these concerns in relation to the shoulder injections reported significant improvement of pain and shoulder function for US-guided injections compared to landmark-guided injections. 18 In contrast, a recent Cochrane review concluded that there was no improved efficacy or advantages of US-guided injections that justify the significant added cost; this conclusion was based on a single study.15 ,19 However, there were several limitations identified for that review.19 Additionally, no previous review evaluated the efficacy of the injections based on the different anatomical locations of the shoulder girdle. This systematic review and meta-analysis aimed to evaluate (1) the accuracy of US-guided injections compared to landmark-guided injections of different shoulder girdle joints, and (2) correlation of accurate localisation with reduced pain and improved function in patients.
Methods
Search strategy
The search strategy and the systematic review protocol were performed in compliance with the PRISMA statement.20 The electronic database of PubMed, Medline and Cochrane were searched up to 31 July 2013. The Mesh terms used were: ultrasonography, anatomical, landmark, corticosteroids, intra-articular, injections, shoulder pain, subacromial impingement, rotator cuff, biceps tendon, GH joint and AC joint. Identified systematic reviews’ bibliographies were also searched for relevant articles (box 1).10 ,18 ,19 ,21 ,22
Eligibility criteria
(A) Inclusion criteria
1. English language papers.
2. Randomised and/or quasi-randomised clinical trials.
3. Human clinical trials comparing the accuracy and/or efficacy of US versus landmark-guided injections.
4. Cadaver clinical trials comparing the accuracy of US versus landmark-guided injections.
5. Anatomical target locations: (i) subacromial space; (ii) biceps tendon sheath (iii) AC joint; (iv) GH joint.
(B) Exclusion criteria
1. Non-English language papers.
2. Case reports, technical reports, pilot and uncompleted studies.
3. Studies with no data analysis and/or power analysis.
4. Animal studies.
AC, acromioclavicular; GH, glenohumeral; US, ultrasound.
Studies selection and critical appraisal
Two authors independently assessed the titles and abstracts from the combined electronic search database for eligibility. Disagreements between the two authors were resolved through a discussion with the third author, and all three authors agreed on the included studies. Similarly, the selected studies were evaluated for bias risk appraisal following the Cochrane review method for intervention, and using the RevMan V.5.2 software.23 Authors also evaluated the studies for any additional limitations related to participant selection, sample size, intervention, confounders, outcomes assessment and data analysis.
An assessment score was developed as follows to simplify the presentation of the quality of analysed trials: (A) For efficacy trials, the score was based on 25 items, with a 3-point scale ranging from 0 to 3 (0=high risk; 1=unclear risk; 2=low risk), and a total score of 0–50 (low-quality—high-quality study). Efficacy trials were graded according to the score: low quality (<30), moderate quality (30–40) and high quality (>40). (B) Similarly, the accuracy trials were assessed based on 15 items using the same scale with a total score of 0–30 and graded as: low quality (<18), moderate quality (18–24) and high quality (>24).
Measurement of efficacy and accuracy
The meta-analysis was performed using the RevMan V.5.2 software.23 Selected papers were further organised according to the anatomical site of injection (subacromial space, biceps tendon sheath, AC joint and GH joint) and according to the outcome (accuracy or efficacy). Studies that reported a pain score (Visual Analog Scale (VAS) or Numerical Rating Scale (NRS)), function score and/or reported adverse events at the same follow-up interval for the same anatomical site were added to the meta-analysis for that group. The mean difference (MD) for change in pain between groups was calculated on a 10-point scale and the standardised MD (SMD) was calculated for change in function. Similarly, studies examining the accuracy of the injection for the same anatomical site were added to the meta-analysis. The 12 index was used to quantify the statistical heterogeneity among the studies added to the meta-analysis.24
Results
Search results
Thirteen clinical trials (four cadaveric studies (300 cadaveric shoulders; 150 shoulders in each group) and nine live human studies (514 patients; 259 in the US group and 255 in the landmark group)) were included in this systematic review (figure 1).25–37 There was total agreement (κ=1) between the two authors who selected and evaluated the clinical trials. Six studies assessing the accuracy (table 1), and Eight studies assessing the efficacy (table 2) of the US-guided injections compared to Landmark-guided injections were reviewed.
Summary table for studies comparing the efficacy of US-guided injections to landmark-guided injections
Summary table for studies comparing the accuracy of US-guided injections to landmark-guided injections

Studies selection flow chart. SAS, subacromial space; ACJ, acromioclavicular joint.
(I) Bias risk assessment (table 3-I): (1) One study used a quasi-randomisation method as the patients were alternately assigned to either the US group or the landmark group in the sequence in which they joined the study.32 Additionally, five more studies did not report the randomisation method used.25 ,26 ,31 ,33 ,34 (2) The allocation concealment method was reported in three studies.29 ,30 ,36 (3) Two efficacy studies reported blinding of the participants.28 ,32 (4) Four studies failed to report blinding of the investigator.25 ,26 ,34 ,37 (5) Three studies failed to report the actual number of patients who completed the full study.25 ,26 ,30 (6) Bias related to selective reporting was noted in three studies. In the first study, the authors did not specify if they measured an active or passive range of motion.26 In the second study, the authors did not explain the rationale for using a modified version of the Constant score.27 In the third study, the authors only reported the data for participants who had active abduction impairment, and did not provide a range of motion measurements.30
Critical appraisal of selected trials
(II) Limitations related to patient selection and sample size (table 3-II): (1) Small sample sizes (10–15 participants in each group) were noted in two studies.33 ,35 Two studies performed a power analysis prior to the study.34 ,37 (2) All efficacy studies excluded patients with a prior cortisone injection and intervention, except for two studies which failed to exclude patients with a prior cortisone injection and/or intervention.26 ,32 (3) Three studies were noted to have heterogeneous shoulder pathology of the participants.25 ,27 ,30 Another two papers had a weak diagnostic method to confirm the presence of bicipital tendinitis/tendinopathy or adhesive capsulitis (inclusion criteria were based on a clinical finding without a confirmatory imaging of the underlying pathology).31 ,32 (4) Four studies failed to report an imaging evaluation of the shoulders prior to the injection.31 ,34 ,35 ,37 (5) All efficacy studies compared the patient demographics at baseline except for one study.26 One study had significantly older participants in the landmark group compared to the US group.33 Two cadaver studies failed to report cadaver demographics (body mass index).34 ,37 (6) There was no significant difference in baseline pain and/or functional score between groups except for one study, where patients in the US group had lower functional scores compared to the landmark group.25 (7) All studies included patients in the chronic stage with a mean duration of symptoms of ≥7 months, except for one study.27 Two studies failed to report the mean duration of symptoms.26 ,31 (8) Another limitation was the characteristics of cadaveric tissue compared to live tissue, which could have affected the accuracy of the injection.34–37 Two studies performed the injection on cadaveric shoulder specimens that would be optimal for positioning; however, this might not be the case when dealing with a real-life patient.34 ,35
(III) Limitations related to intervention and cofounders (table 3-III): (1) One study did not report the injection approach.27 Two studies reported the use of an in-plane approach for the US group, but they did not clearly report the point of entry or the exact approach.25 ,30 (2) All the efficacy studies failed to assess the accuracy of the injection in both groups, except for one study that used postinjection MR arthrography to assess the accuracy of the injection.28 Although another study used a postinjection US to assess the accuracy in the landmark group, another imaging modality (MR arthrography) should have been used to compare both techniques.30 One cadaveric study used an ultrasonography evaluation of the AC joint in both groups before and after the injection of 2–5 mL of water instead of using a direct dissection or another imaging modality.36 (3) Two papers reported the number of years of experience for investigators who performed the injections.32 ,35 Three papers failed to report the qualification(s) of the investigators who performed the injections.25 ,27 ,31 (4) Two studies allowed a repeated injection for patients with poor response after the first injection.27 ,31 One study used six consecutive injections in each group.32 Another study used half the dose of the injectate for patients with a history of diabetes; however, they did not provide the details about the exact numbers of diabetic patients in each group.31 (5) The use of NSAIDs/analgesics during the study was not reported in three studies.25 ,26 ,32 Although another three studies reported that the use of medications was discontinued, recorded or limited to a certain dose, the data for medication consumption was not reported in the results section.28 ,29 ,31 (6) Participation in physiotherapy or home-based exercise programmes was not reported in four papers.26 ,27 ,29 ,31 Although the other three studies reported that patients with a reduced range of motion were instructed to perform a home exercise programme, none of the studies recorded the frequency, intensity, type and time for the exercises performed, or the patients’ compliance.25 ,30 ,32
(IV) Limitations related to assessment and data analysis (table 3-IV): (1) One study had limited the follow-up to 1 week postinjection.26 Another study had a follow-up assessment every 4 weeks, with a mean follow-up time of 31 and 34 weeks for the US and landmark groups, respectively.31 However, it is not clear at what time points the follow-up outcome data presented in the paper were collected. (2) Three papers failed to report on the side effects related to the injections in each group.26 ,29 ,32 One paper did not specify which group had the reported adverse events.27 (3) All but two studies did not compare the mean change difference for the pain and function scores between the US and landmark groups.25 ,30 One study did not compare the measured outcome at baseline or follow-up, as it based its results on significant improvement in the US group and lack of significant improvement in the landmark group.26 (4) Several studies used multiple tools to assess the efficacy and clinical outcomes postinjections without correcting the p values to avoid type I error.25 ,27–32 (5) Two studies did not clearly report the test used for statistical analysis of the presented data.26 ,31
Accuracy and efficacy results
Subacromial space injection
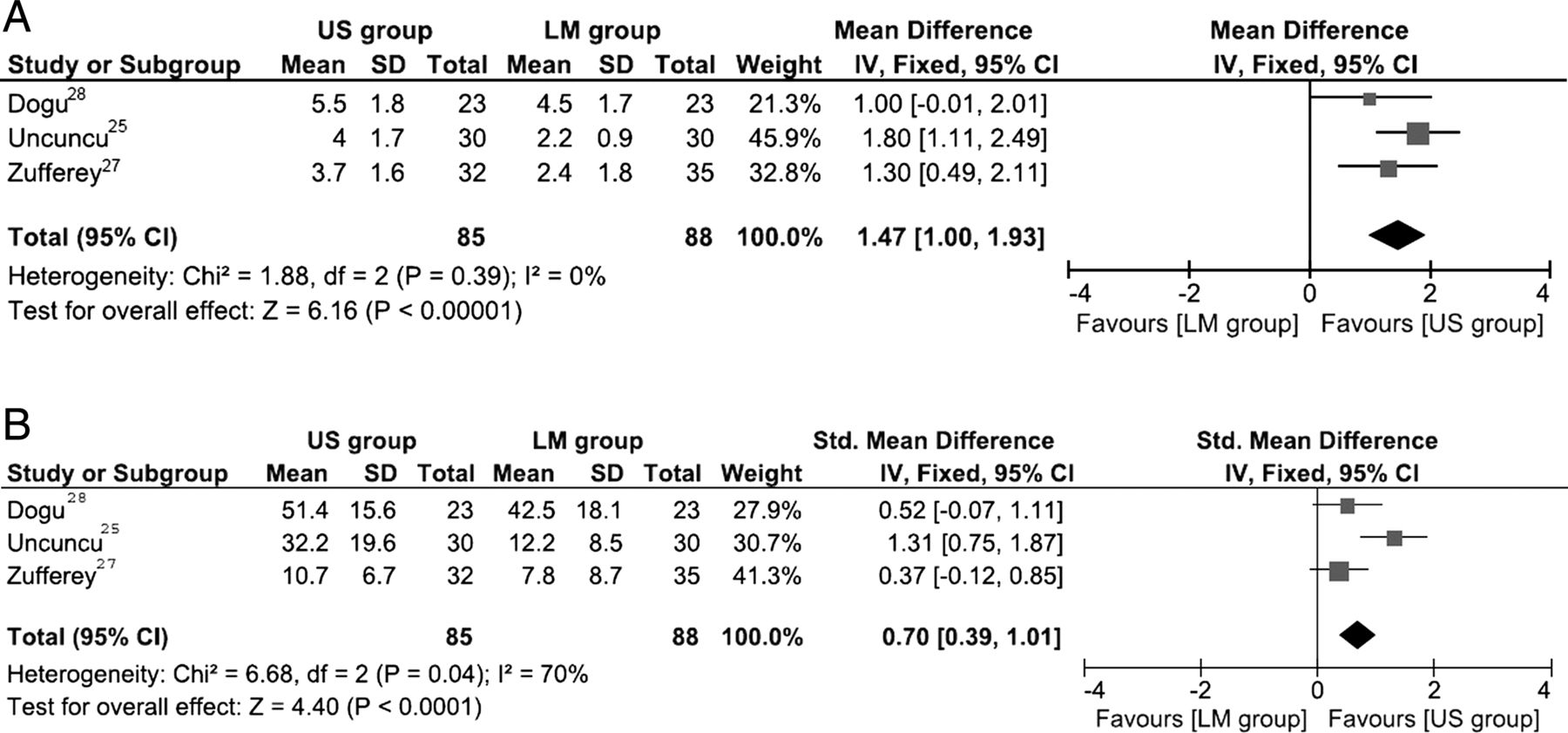
Based on one trial (high quality), the accuracy of US-guided injections versus landmark-guided injections was 65% versus 70% (p>0.05).28 Based on three trials (two moderate and one high quality), the US group had a significantly greater reduction in pain (MD 1.47, 95% CI 1.0 to 1.93, p<0.00001, I2=0%) and greater improvement in function (SMD 0.70, 95% CI 0.39 to 1.01, p<0.0001, I2=70%; figure 2A, B) at 6 weeks postinjections.25 ,27 ,28 Based on two trials (one moderate and one high quality), there was no significant difference for the reported adverse events (1/53 in the US group and 6/53 in the landmark group, risk ratio (RR) 0.17, 95% CI 0.02 to 1.30, p=0.09).25 ,28 The adverse events were limited to mild postinjection pain or skin peeling in one patient who had a landmark-guided injection.25
{kind=link}
{kind=link}
Forest plot graph for efficacy of subacromial space injections. (A) MD for pain change in the US group compared to the Landmark group at 6 weeks post injection. (B) SMD for functional score change in the US group compared to the Landmark group at 6 weeks post injection. MD, mean difference; SMD, standardised MD; US, ultrasound; LM, landmark.
Biceps tendon sheath injection
Based on one trial (moderate quality), the accuracy of US-guided injections versus landmark-guided injections was 86.7% versus 26.7% (p<0.05).33 Based on one trial (low quality), the US group had a greater reduction in pain (MD 1.9, 95% CI 1.2 to 2.6, p<0.00001) and greater improvement in function (100-point scale) (MD 10.9, 95% CI 6.57 to 15.23, p<0.00001).31 There was no significant difference between groups for the reported adverse events (0/35 in the US group and 0/45 in the landmark group).31
GH joint injection
Based on one trial (moderate quality), the accuracy of US-guided injections versus landmark-guided injections was 92.5% versus 72.5% (p=0.025).34 Based on one trial (low quality) for patients with adhesive capsulitis, the US group had a lower reduction in pain VAS with (MD −0.6, 95% CI (−0.8 to −0.4), p<0.00001), and no significant difference between groups for function (40-point scale) (MD 0.12, 95% CI (−1.33 to 1.58), p=0.87) at 6 weeks postinjection.32
AC joint injection
Based on three trials (one high quality and two moderate quality), the accuracy of US versus landmark-guided injections was 93.6% versus 68.2% (p<0.0001, I2=0%).35–37
Discussion
The results of this systematic review and meta-analysis showed a significantly improved accuracy for US-guided injections into the biceps tendon sheath, GH joint and AC joint compared to landmark-guided injections.33–37 However, the accuracy of the subacromial space was similar between US-guided injections (65%) and landmark-guided injections (70%).28 Except for the AC joint, the injection accuracies were based on single studies, and should thus be interpreted with caution. This is particularly important to note for the subacromial space injection, as one study has reported a higher accuracy (accurate placement in all cases) for both injection techniques.17 Similarly for the GH joint, another study reported a higher accuracy of the landmark-guided injections (98.2%).38 Several factors come into play when reflecting on why variations exist in the reported accuracies of musculoskeletal injections in the literature. Some of this variation may be influenced not only by the injector's years of experience, but also by the nature of training and the case volume load over time. In addition, several weaknesses have been noted with the manner in which injection accuracy itself has been investigated in the literature.11 Thus, one can consider that only meta-analysis data may be of value when comparing the accuracy between two techniques.
Despite the lack of improved accuracy for US-guided injections of the subacromial space based on one study, there was a significantly greater improvement in terms of pain reduction and functional gain in the US group in the meta-analysis.25 ,27 ,28 Although this could arguably be related to the lack of participant blinding (2/3 studies), one would expect the placebo effect to be minimal with both groups receiving the same injection.25 ,27 An important factor to consider is the increased patient comfort and less needle manipulation with US-guided injections, which was not assessed. With regard to functional score improvement, there was substantial heterogeneity between the studies and a small clinical effect.25 ,27 ,28 This could be better explained by the lack of a structured home exercise/physiotherapy programme impacting the size of the clinical effect.39 Of additional importance is that most of the trials included patients with chronic symptoms, which might have limited functional gain from a corticosteroid injection alone, making it difficult to assess if there was a difference between groups.
The improved accuracy of the biceps tendon sheath injections correlated with an improved clinical outcome in the US group.31 ,33 On the other hand, the improved accuracy of the GH joint injections correlated with a greater short-term improvement in the US-guided injection group, but there were no added benefits beyond the third week.32 ,34 However, this was based on a single study with two notable limitations:32 (1) Patients selected for the study were in the chronic stage (Frozen stage) of adhesive capsulitis, which has less response to corticosteroid injections.40 (2) The initial cortisone injection was followed by five consecutive weekly hyaluronate injections.32 This might explain the early improvement in the US group; however, with repeated injections, there was the increased probability of an accurate injection in the landmark group.
Disagreement with previous systematic reviews
The recent Cochrane review reported no significant improvement in efficacy with US-guided injections.19 However, the following limitations are noteworthy for that review: (1) There was considerable heterogeneity in the included trials, and the authors did not perform the analysis based on the injection location, as they added trials by Lee et al (GH joint injection) and Naredo et al (injections were not limited to the subacromial space in the US group) to their combined analysis. (2) The authors relied on the final pain and function score MD between groups instead of the mean change difference, which provides a more accurate method to detect changes and takes into consideration any variation at baseline. (3) Although the review included five studies, they based their conclusion mainly on one trial by Ekeberg et al,15 which compared the efficacy of US-guided injections of the subacromial space with that of systemic corticosteroid injections in the gluteal muscle. 25 ,26 ,30 ,32 (4) In addition to Ekeberg et al's15 trial not being designed to compare the efficacy of US-guided injections with that of landmark-guided injections, another important limitation was noted for that study; the systemic group received a US-guided injection of 5 mL 1% lidocaine into the subacromial space for the purpose of blinding. This lidocaine injection might have contributed to the local pain relief, which has been reported in previous studies to have comparable efficacy to cortisone.41 ,42
Limitations to this systematic review
(1) We did not include the range of motion data in the meta-analysis. The authors had reached this decision based on the following: (A) Some studies did not clearly specify if they assessed active or passive ROM. (B) Studies used different follow-up intervals. (C) The functional improvement represented an overall better indicator of efficacy of treatment compared to ROM. (2) There was marked variation for functional scales used between studies, and therefore we used SMD for all functional scores. (3) We pooled results for rest/night time pain on a 10-point scale, but we also added unspecified pain for those articles that did not specify. (4) There were varied definitions of accuracy in the included articles. Ideally, accuracy should be confirmed by the accurate placement of the needle tip using arthrography under fluoroscopy or by MR arthrography, which was not always the case in the reviewed studies.11 ,43 Some papers only looked at whether the injectate reached the structure of interest, but did not note if it had tracked into adjacent structures.
Implications for clinical practice
US-guided injections have gained widespread use over the last few years, particularly in the hands of non-radiologists, replacing the traditional ‘blind’ approach.14 Although some of the literature has noted concerns about the lack of efficacy to justify the substantial increased cost, no study has yet performed a cost-effective analysis to investigate this further.15 ,19 Until such an analysis has been completed, the argument of US-guided injections versus Landmark-guided injections should be solely based on the efficacy analysis. Our data clearly support the superiority of US-guided injections of the shoulder girdle over landmark-guided injection with the use of corticosteroids. Furthermore, if orthobiological medication has no systemic effect—only local—then accuracy will be even more important.
Conclusion
US-guided injections showed improved accuracy compared with landmark-guided injections for all shoulder girdle injections, with the exception of the subacromial space. In addition, there was significantly greater improvement in pain and function scores for subacromial space and biceps tendon sheath injections. There was also a trend towards less side effects in the US-guided injection groups. Unfortunately, there was insufficient information for us to comment on whether these advantages would be cost-effective or not.
Key messages
A recent Cochrane review has suggested that there was insufficient improved efficacy or advantages to justify the added cost for US-guided injections.
This systematic review and meta-analysis showed that US-guided injections provide superiority in accuracy and efficacy for most of the shoulder girdle regions.
There was insufficient information for us to comment on whether these advantages would be cost-effective or not.
References
Footnotes
Contributors A-RA planned the study, performed the search strategy, selected the eligible trials, extracted the data, performed the critical appraisal, performed the meta-analysis and prepared and modified the manuscript. SR planned the study, performed the search strategy, selected the eligible trials, performed the critical appraisal, and reviewed and modified the manuscript. NA planned the study, reviewed the selected trials and the critical appraisal, performed and reviewed the meta-analysis, and reviewed and modified the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.