Article Text

Abstract
Purpose To present an epidemiological study of injuries found among South Korea's National level Judo athletes as a foundation for future injury prevention and skill enhancement in this group.
Methods This study is a prospective study on a 4-year injury assessment held from January 2010 to December 2013 at the training centre in South Korea for National Level athletes. Athlete's weight class, gender, injury location and injury grade (grade I=1–3 treatment days, grade II=4–7 treatment days, and grade III ≥8 treatment days) were analysed.
Results There were a total of 782 injuries recorded during this period, equalling to four injuries per athlete annually. Almost half of these injuries (47%) were grade I injuries. Injury occurrence was the highest in the Lower body (44.2%). This was then followed by injuries in the upper body (29.8%), trunk (20.3%) and head and neck (5.6%). Men and women showed similar, non-significantly different trends in the proportion of body parts injured. Women experienced more grade III injuries than males (p=0.0228). Comparison between women in different weight classes also showed that heavyweights incurred more grade III injuries than lightweights (p=0.0087). Lightweights had a higher rate of injury than heavyweights in males and females, although this was statistically significant only among males (p<0.001).
Conclusions Many body regions are prone to injury in the elite judo population. Women, especially those in the heavyweight classification, were more prone to severe injuries. Lightweights experienced more injuries than heavyweights among male athletes. Specifically, further studies are needed to confirm these findings and to address the impact of rapid weight loss practices on injury risk to implement effective preventive measures.
- Epidemiology
- Judo
- Injuries
- Elite performance
- Martial Arts
Statistics from Altmetric.com
Introduction
The purpose of judo is to teach martial art discipline, control and respect.1 The International Judo Federation is very much global, with 200 affiliated countries.2 Since its participation in the Olympics, Judo in Korea has won a total of 40 medals: 11 Gold, 14 Silver and 15 Bronze, averaging over four medals per Olympic Games. The training in Korea for all the national level judo athletes is also unique as they train and prepare together at a specified location. Training among the athletes has also revealed that an injury in a judo athlete, although the sport of judo being an individual and not a team sport, can have a negative effect on all the athletes simultaneously as they train and practice together as a whole for their own personal development. 3
Recent studies in the 2008 Summer Olympic Games also identified that a high percentage of competition injuries occurred in Judo.4 Other findings from epidemiology studies in judo revealed that the associated risk in judo may be as large as, or even larger than, that in team sports such as soccer, volleyball and basketball.5–7 Also, a study from 1990–2003 in the USA witnessed significant annual increases in Emergency Room visits relating to judo and other martial arts injuries.1
Judo athletes are classified into respective weight classes. Different weight classes were intended to establish equality between opponents in mass and strength in sports such as judo, wrestling and tae kwon do.8 However, this categorisation has been of much concern as athletes take in extreme measures (fasting, laxatives, vomiting, sauna, etc.) to rapidly lose weight to be categorised into a lower weight class.9 , 10 This culture has also been the cause of multiple deaths throughout history. Some prime examples involved three US collegiate (NCAA) wrestlers in 1997 and Chung Se-hoon in 1996, a South Korean judo medallist.11
This practice of rapid weight loss (RWL) may even impair the performance of these athletes during competition.9 , 10 Various studies have revealed short-term and long-term bodily injuries due to this practice,9 , 10 and the concern is underscored by the fact that many judo athletes start this practice at a young age, leading to possible delayed pubertal development and bone growth retardation.12 Coaches, athletes and the medical team invest much time and energy to place their athlete into a lower weight class.
There have been various studies on the frequency and incidences of injuries in the sport of judo. However, epidemiological studies of the elite competitive judo population are rare.13 The present study evaluated the injury patterns of elite judo athletes with the purpose of reducing injuries and protecting the health of the elite judo population. It has been shown that elite athletes have a different Physiological Profile and Psychological mindset at multiple levels when compared to those participating at the collegiate or recreational level.14 , 15
For 4 years (January 2010–December 2013), an injury evaluation had been carried out at the training centre in South Korea for National Level athletes. This study is a prospective study analysing the results from this injury evaluation. The first goal was to compare the injuries among males and females in the elite judo population. The second goal was to compare the data between heavyweight and lightweight injuries, and to analyse if weight and the weight class system might have any role in injury causation.
Materials and methods
Subjects
A 4-year injury evaluation was held from January 2010 to December 2013 at the training centre in South Korea for National Level athletes. Consent was obtained from all subjects and was conducted according to the Declaration of Helsinki. These athletes were selected to train at the National training centre with an expectation of representing South Korea at international sporting events such as the World Championships and Olympic Games. On average, 24 male athletes and 24 female athletes trained and competed annually at the centre. The athletes were divided into two groups (lightweight and heavyweight) to compare injury trends between lighter and heavier athletes. The categories were set by dividing the weight classes in Olympic Judo. Of the 24 males, 10 were lightweight athletes and 14 were heavyweight athletes. Of the female athletes, 11 were lightweight and 13 heavyweight. Elite athletes were divided into Major (top-ranked) or Minor (possible candidate athletes). Annually, 25–30% of the athletes were in the Major category and most of them were at the facility during the 4 year surveillance. The Minor athletes, on average, stayed for a year at the facility if they did not qualify higher up in the ranking. Athletes trained on average 4.5 h per day, 5 days a week. Training during this time included strength and conditioning, and also judo-specific training. The athletes were present at the facility for 10 months (43.3 weeks) in of the year, totalling 975 h of training annually.
Data collection
For this study, an injury was defined as any musculoskeletal symptom, new or recurring, during their time of stay at the training centre, whether it was witnessed, or when the athlete sought medical attention.16 During the athlete’s stay at the training centre from January 2010 to December 2013, injuries witnessed or reported by the elite judo athletes were examined by the facilities’ Sports Physician or by an experienced Sports Physician of an outside hospital. Any athlete who chose to be examined at an outside hospital still had to report to the training staff and receive all physical therapy at the training centre facility. From 2010 to 2011, one physician was in charge of all the injury diagnoses. A new physician took over in 2012 and was present till the end of this study. After being diagnosed, the athletes received treatment from the physical therapists, where the plan and duration of treatment were recorded. On average, 8.5 physical therapists were at the medical/rehab centre of the facility during the 4 years. Two physical therapists left and were replaced by two other therapists during this study period. Data regarding the site of injury, the athletes’ weight class (light and heavy), gender and injury grade (grade I=1–3 treatment days, grade II=4–7 treatment days, and grade III ≥8 treatment days)17 were extracted and assessed. Injury site was set to the regions used by the IOC during the London Summer Olympic Games,18 and then subdivided into the head and neck, upper body, trunk and lower body regions.
Statistical analysis
Variables examined included gender, weight class, body regions and injury grade. Injury rate, injury frequency of each body region, and incidence of injuries were identified. Data were analysed using Microsoft Windows SPSSWINN 21.0. The χ2 test was used to test the statistical significance of categorical data. The Poisson Distribution was used to obtain the Z score by assessing the statistical significance of data when the average rate of injury in a fixed interval of time was compared within different groups. To calculate OR and 95% CI values of injury rates between gender and weight class, logistic regression analysis was performed. The level of significance in all statistical analyses was set at p=0.05.
Results
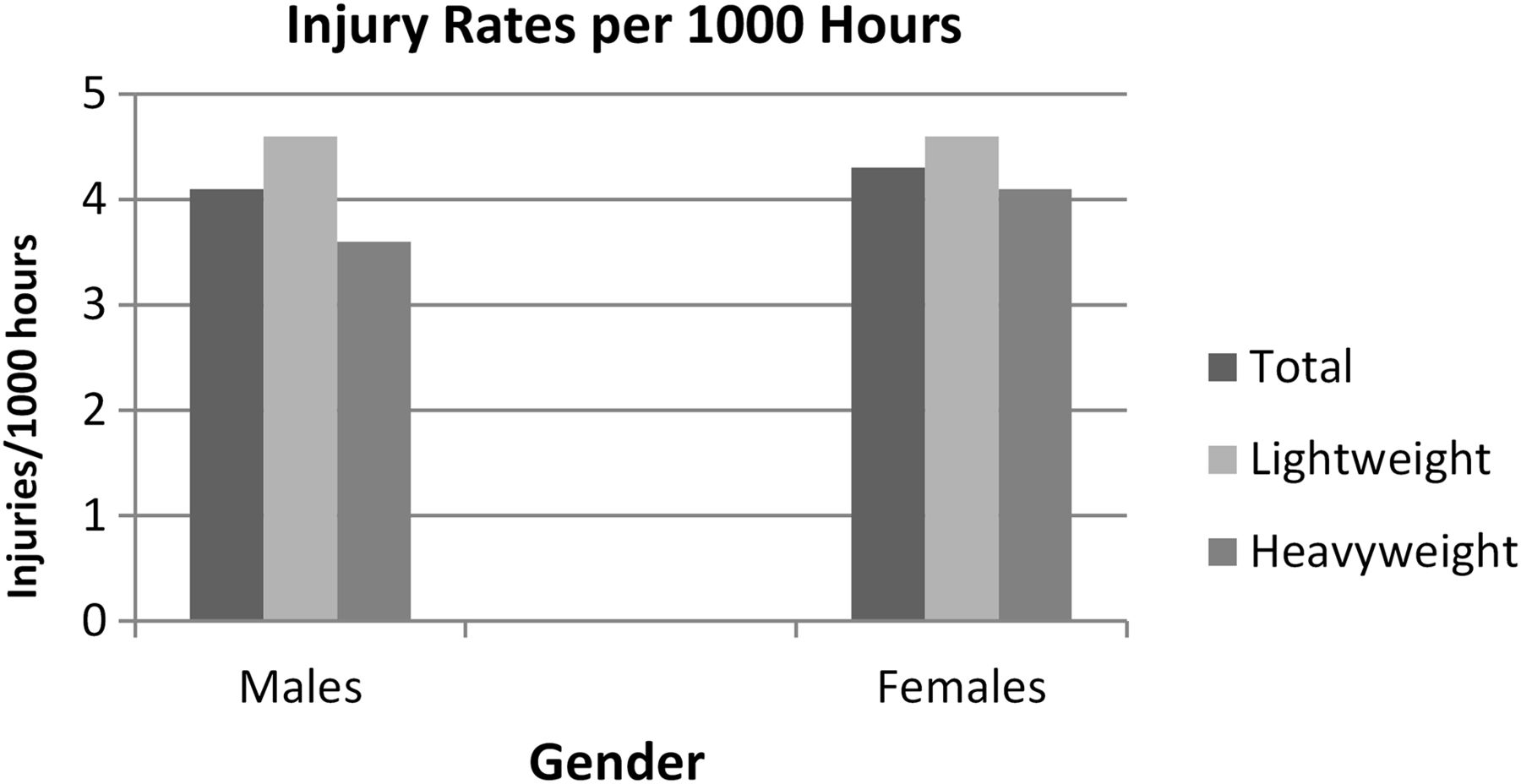
At the Training Center, there were a total of 782 injuries recorded during January 2010 until December 2013 (table 1). Around 95% of the total injuries occurred while training at the facility. The other 5% of injuries were treated at the training centre, but only after the athlete returned from competition and did not receive adequate treatment prior to arriving at the centre. Men had a total of 379 injuries during that time (181 lightweight injuries and 198 heavyweight injuries). Women had a total of 403 injuries (196 lightweight injuries and 207 heavyweight injuries). When comparing males and females in their respective weight categories, the OR (95% CI) value was found to be 1.04 (0.78 to 1.37), and the distribution of injury rate in the two categories was analogous to each other. Thus, the difference in this injury rate between sex and weight category was not statistically significant (p=0.8060). The total injury rate was 4.1 injuries/year for each athlete. For men, the annual injury rate was 4.0 injuries/male athlete (4.5 for lightweights and 3.5 for heavyweights). For women, the annual injury rate was 4.2 injuries/female athlete (4.5 for lightweights and 4.0 for heavyweights). As each athlete averaged 975 h of training annually, the injury rate was 4.2 injuries/1000 h of training per athlete at the centre. For men, the injury rate was 4.1 injuries/1000 h of training. When comparing men in their respective weight classes, the rates were 4.6 for lightweights and 3.6 injuries for heavyweights (z=4.7893, p<0.001). For women, the injury rate was 4.3 injuries /1000 h of training. The comparison of rates in women showed 4.6 for lightweights and 4.2 for heavyweights (z=1.9111, p>0.05) (figure 1).
Body region injuries: men and women

Injury rates per 1000 h of training in male and female judo athletes. In men, the rates were 4.6 for lightweights and 3.6 injuries for heavyweights (z=4.7893, p<0.001). In women, the rates were 4.6 for lightweights and 4.2 for heavyweights (z=1.9111, p>0.05).
Almost half of these injuries (47.1%) were grade I injuries (1–3 treatment days). Grade II injuries (4–7 treatment days) were 28.6% and grade III injuries (greater than 8 treatment days) were 24.4%. Injury proportions occurred in the order of the lower body (44.2%), upper body (29.8%), trunk (20.3%) and head and neck (5.6%). Men and women showed similar trends in body region injuries (figure 2), but this was not statistically significant (p=0.36). The knee, lower leg, ankle, lumbar spine/lower back, shoulder and elbow were the most common sites of injury (table 1).
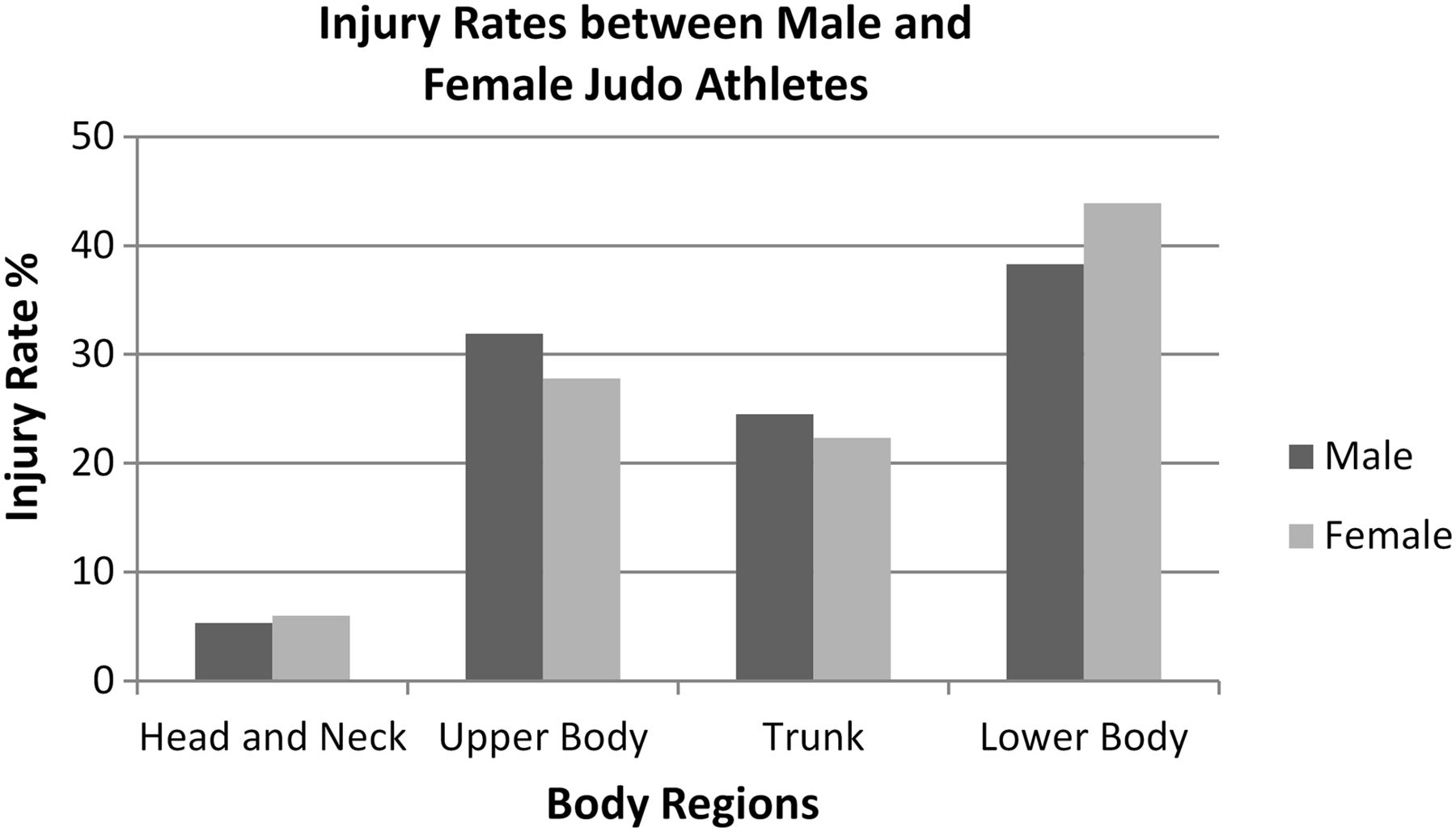
Comparison of male and female injury percentile at the National Training Center.
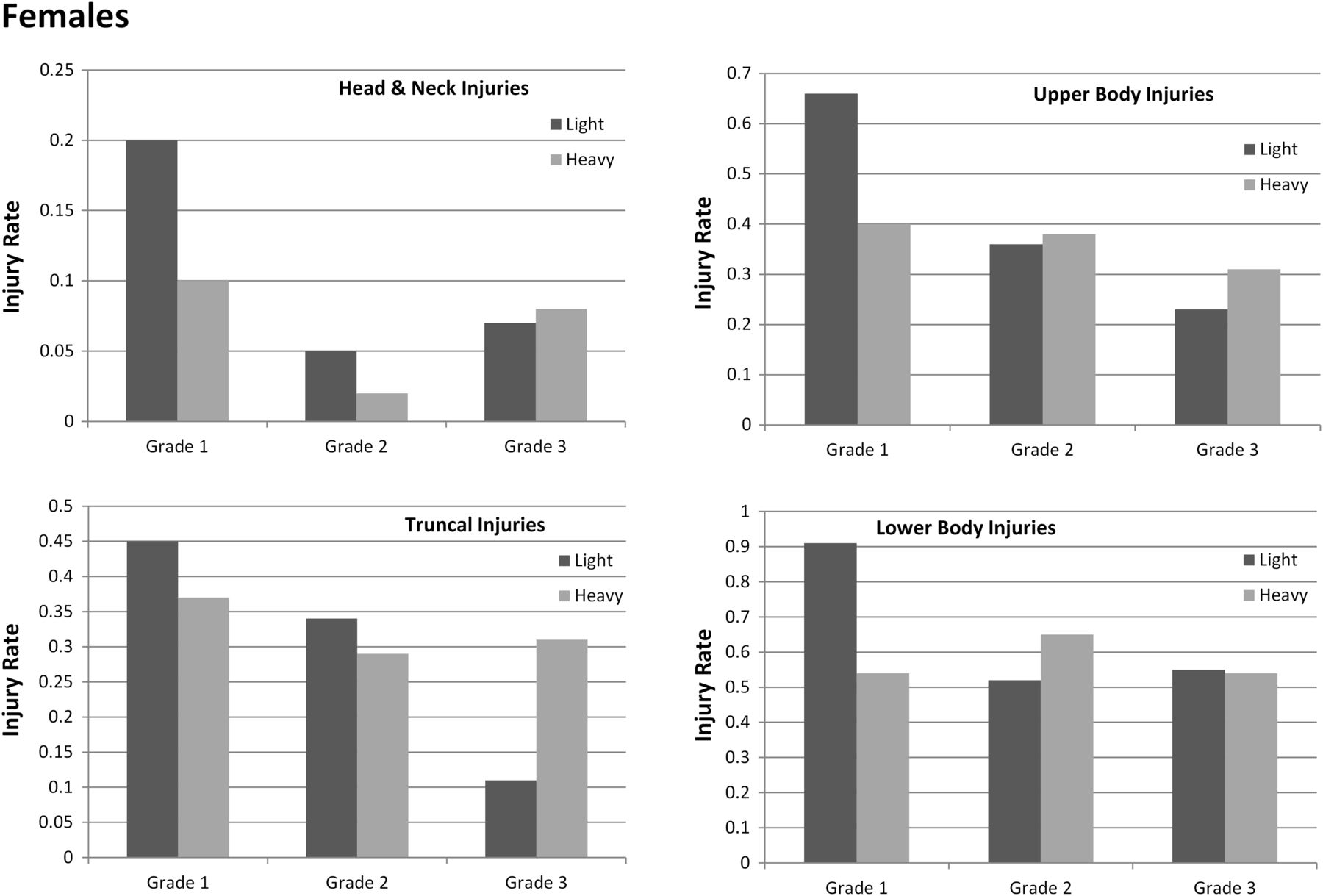
In tables 2 and 3, regarding the number of injuries athletes experienced, women experienced more grade III injuries than males (p=0.0228). However, this was significant only in a comparison between male heavyweights and female heavyweights (p=0.0041) but not between male lightweights and female lightweights (p=0.6347). Comparison between women in different weight classes also showed that women heavyweights incurred more serious injuries (grade III) than women lightweights (p=0.0087). Also, half of all injuries in the female lightweight category fell into grade I (similar to the male judo athletes), whereas only 35% of female heavyweight injuries fell into grade I. Total lightweights also incurred more mild grade 1 injuries than total heavyweights (p=0.0078) (see online supplementary tables S1 and S2). Figures 3 and 4 and tables 2 and 3 detail the rate of injury by body region, according to the athlete's injury grade and weight class. In both males and females, lightweights experienced more grade I injuries than heavyweights in all four regions. Female heavyweights had greater rates of grade III injuries than female lightweights on the head and neck, trunk and upper body regions (figure 3). Male heavyweights had greater rates of grade III injuries than male lightweights on the head and neck, upper body and lower body regions (figure 4).
Women heavyweight and lightweight: injury grade and values of injury region frequency
Men heavyweight and lightweight: injury grade and values of injury region frequency
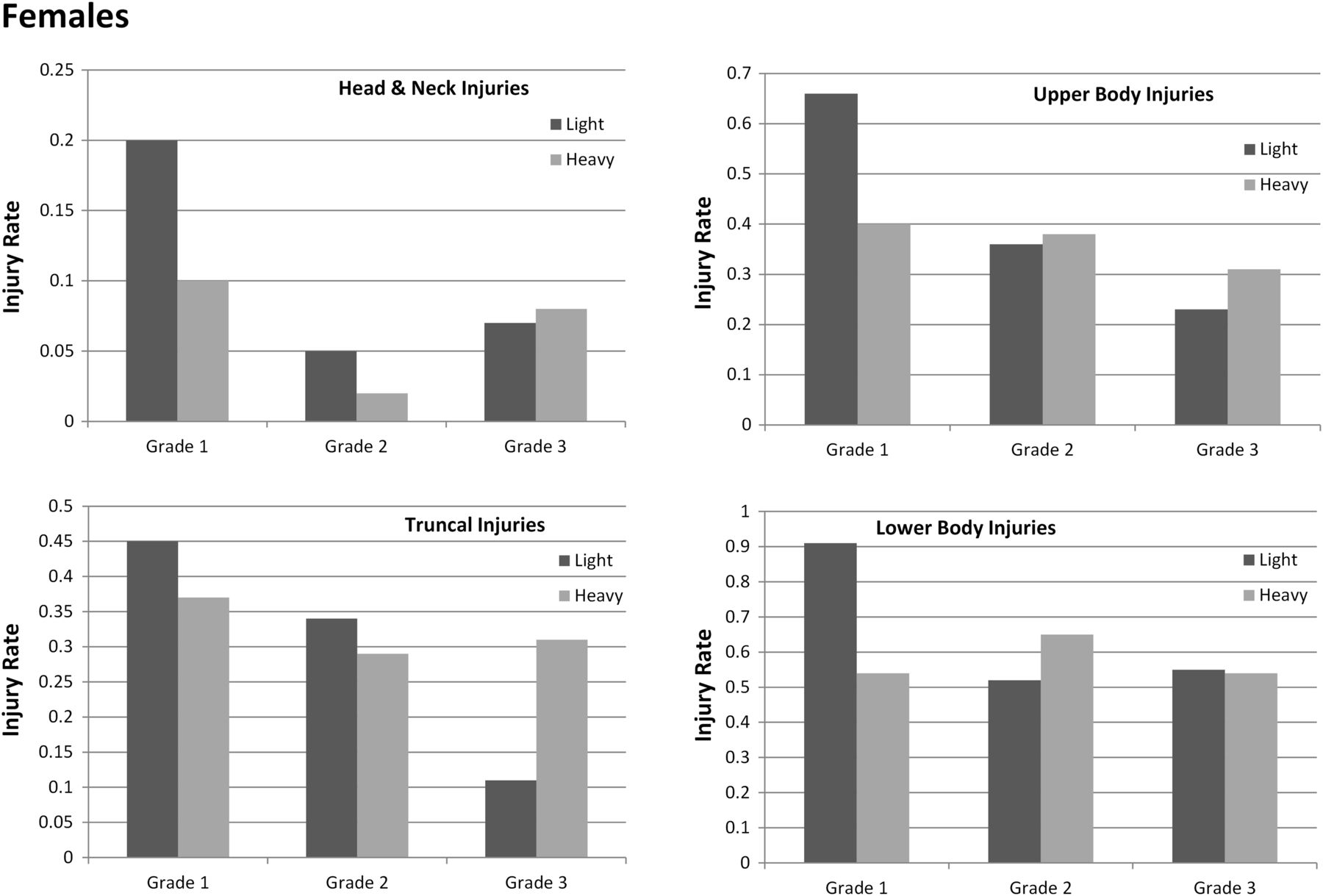
Rate of injury by weight class and injury grade according to the number of athletes over 4 years (women: 44 lightweights, 52 heavyweights). Regions of the head and neck/upper body/trunk/lower body.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rate of injury by weight class and injury grade according to the number of athletes over 4 years (males: 40 lightweights, 56 heavyweights). Regions of the head and neck/upper body/trunk/lower body.
Discussion
The purpose of this study was to evaluate long-term injury frequencies and trends among the elite National level judo population of South Korea. To date, there have been very few studies that have analysed health risks in the elite judo population. Comparing the results of this study with those of previous studies is difficult as the definition of an injury is not standardised, and the methodologies of the study design varied. However, comparison with previous studies will still provide perspectives to injury trends among the elite judo population.
A previous retrospective study was carried out at the same training centre in South Korea for National Level Athletes from November 1996 to December 2000. In total, the study had 172 injuries during that time period. The main difference in data recording between the two studies was that the previous retrospective study only included injuries which required greater than 1 clinic visit and/or required a minimum 3 days of treatment. Therefore, data from the 2010–2013 study was adjusted by excluding grade I injuries (1–3 days of treatment). Furthermore, only the total men’s and women’s data in this study were comparable, as the previous retrospective study did not differentiate between weight class or gender.
During 1996–2000, there were, on average, 28 male and female athletes training annually. The injury rate for the 1996–2000 study was 1.5 injuries/year for each athlete, whereas with the adjustment of the 2010–2013 study, it resulted in 2.2 injuries/year for each athlete. Trends were found to be similar between the two epidemiological studies, although the previous study showed greater injuries to the knee (24.6% vs 10.2%). In both studies, the order of injury proportion was similar: lower extremity (highest injury proportion), upper extremity, trunk, and head and neck (lowest injury proportion).
One possible explanation for the decreased knee injury rate but overall increased injury rate in this study is the training method. Current training methods emphasise more on personal skill enhancement than previously (learning and attempting new manoeuvres may broaden the types of injuries an athlete may experience). Also, an explanation of the increase in injury rate (from 1.5 to 2.2) may possibly be due to the difference in recording of the injury and/or a more meticulous data collection procedure in this study. The lower injury proportion found in the knee joint (from 24.6% to 10.2%) could be due to preventive/awareness measures that may have taken place, as knee joint injuries are more debilitating and also require longer periods of time off from injury.
Two prior studies on injuries among elite judo athletes were also compared with this study. The first study was a video analysis of 124 matches, fought by 83 different judo athletes, during four international judo tournaments held in 2006 and 2007.19 The second study was of data gathered from the London Summer Olympic Games.18 The first study only recorded data during competition, while the second study recorded injuries during competition as well as training activities during the 17 days of the Olympic Games.
A third study in England during three Senior Collegiate level judo tournaments in 200520 was also used for comparison. Although the participants were not all at the elite level, the data had good correlation with the previous two International studies.
All three studies had the injuries occur in the order of upper extremity > lower extremity > head and neck > trunk. This differed from the previous two epidemiological studies at the Korea National Training Center, as most injuries happened in the Lower extremity and the least in the Head and Neck regions. Another analysed difference was that injuries in the trunk were very rare in the three studies, with none during the 2006–2007 tournaments, only one recorded during the 2012 London Games, and only two injuries in total (1 male and 1 female) noted in the trunk during the three senior level tournaments in England. At the training centre, 20% of the injuries were in the trunk, most notably in the lumbar and thoracic spine.
Prior studies on injuries also noted major differences in injury trends when comparing training injuries versus competition injuries. Studies during the Summer Olympic Games 2008 and 2012 similarly found that injuries in training and in competition differed significantly in all injury characteristics.4 , 18
Since the most common site and mechanism of injury have been shown to vary in the literature,20 further studies are needed, especially in the elite athletes, to compare specific injury patterns from competitions versus in training to help prevent such injuries from occurring. Also, as practice sessions are quite longer than competition periods, understanding mechanisms of injury due to muscle fatigue and exhaustion may play a key role in having effective preventive measures.
In regard to spinal injuries, observance at the training centre showed that these spinal injuries usually occurred during weight training or with extreme rotations of the back while the athlete attempted throws. A study on lumbar spondylosis showed that judo players were significantly prone (20%) to suffer this type of injury.21 It frequently occurred in athletes with repetitive trunk movements. A biomechanical study by Sairyo et al 22 may explain this issue as it defines high stress occurring in the back during movements of extension and rotation.
The knee, lower back, elbow and shoulders were the main injured body regions found in our study. After much observation of the athletes, knee injuries happened frequently secondary to high valgus stress on the joint. The MCL and ACL were found to be the most common knee ligaments injured in judo athletes,23 as valgus force was found to be a common mechanism of injury to the MCL24 and ACL.25 Lower back injuries were found with extreme rotations and imbalance while attempting throws. Most of the spinal injuries also occurred secondary to weight training. Shoulder and elbow injuries frequently happened when colliding with the mat on the ground or attempting to defend against an attack. Also secondary to the arm bar manoeuvre, elbow injuries were common. It can be concluded that areas of the body most likely to come into contact with an opponent are most likely to sustain an injury in judo.20
Women displayed a higher annual injury rate than males (4.2 vs 4.0), and women also sustained more serious grade III injuries than males. This was significant when comparison was made between women and men in the heavyweight class but not between women and men in the lightweight class. In fact, the female lightweights had the same injury rate as the male lightweights. Green also found that the two most serious injuries in his study affected the heavyweight judokas.20
The incidence of injuries was found to be higher in the lightweight class than in the heavyweight class for both males and females (4.5>3.5 in males, and 4.5> 4.0 in females). Total lightweights also incurred more mild grade 1 injuries than total heavyweights (p=0.0078). Although the comparison of the rate of injuries in male lightweights versus male heavyweights was statistically significant (p<0.001), but not between female lightweights and female heavyweights (p>0.05), this may be a matter of concern as studies have shown that athletes in the lightweight category practise more extreme weight-loss behaviour than athletes in the middle and heavyweight categories.26 In the light of a recent death in 2014 of a middle school female judo athlete secondary to RWL in South Korea, and multiple studies showing increased risk of injury due to RWL, what percentage of injuries in judo can be attributed to this practice of RWL?
This practice of RWL is prevalent in sports with weight categories. Studies show that 90% of judo athletes have already rapidly reduced body weight before a competition, with another study finding showing 63% reducing weight rapidly on a regular basis.11 , 27 Many combat athletes have lost weight of up to 5–10%, with many also reporting a greater than 10% reduction of body weight.11 , 27 , 28 60% of judo athletes have also started this practice at an early age (12–15), and patterns also show that RWL among judo competitors are as inappropriate as those reported regarding wrestlers before the NCAA's weight control programme.11 This can negatively impact an individual's growth and development, and the rate of obesity was also found to be more prevalent in former combat athletes.29 Studies have also shown how RWL can have a negative impact on lean body mass (LBM), strength and performance.30–33
Hydration testing revealed that almost half of the athletes were seriously hypohydrated on the morning of competition day.8 These deficits are known to negatively affect thermoregulation, cardiovascular function and metabolism.34–36 One study showed that the likelihood of injury significantly increased as the body does not have enough time to recover from the dehydration.20
Dehydration secondary to RWL also affects the immune system. With reduced water in the blood, circulation of the immune system related substances was inhibited. Also, testing of neutrophils revealed cell dysfunction with dehydration.37 This may be significant as one in five illnesses during the London SOG resulted in absence from training or competition.18 Infection was the most common cause of illness, and women in particular had a higher incidence of illnesses compared to the male athletes.18 This factor may play a role in preventing the athlete from achieving their lifelong goal at the Olympics.18
Although weight divisions were initially intended to establish equality between opponents, the focus today seems to be more about being able to alter their power to weight ratio and gaining an advantage by classifying into a lower weight division.8 This strategy may work initially at the lower tiers of competition, but we question the effectiveness if almost all of the athletes practise RWL before the tournament and compete with each other. Athletes today may be moving up the ladder of competition not just for their physical athletic attributes but also because of their willingness to possibly sacrifice their long-term health. It should also be considered how many talented athletes fail to achieve success and continue in the sport secondary to their unwillingness to rapidly lose body weight within a short period of time, or even also due to their inability to lose weight and overcome extreme hunger and thirst.
In the NCAA weight certification programme, each athlete has to be evaluated for minimum weight at the beginning of the season; this would be used to determine the category the athlete will be able to compete in during the season.33 These regulations have been successful in the athletes’ weight management behaviour,33 and should also be considered in the sport of judo globally for the protection of the athletes.
In conclusion, nearly half of all injuries in the elite judo population were considered minor injuries. Many of the more serious injuries seem to occur more frequently among the heavyweights, especially the female heavyweight athletes. The total number of injuries occur at a more frequent level among the lightweight athletes. The exact cause is unknown, however, as lightweights are found to practise more extreme behaviour of RWL, future studies are necessary to establish if this may play a role in causation of more injuries. Also, a follow-up biomechanical study of movements among the elite judo population will be necessary for implementations of an effective injury prevention programme.
Limitations
We were not able to factor in the 1 athlete who left the centre on average annually midseason due to a severe injury or for personal reasons. However, every injury that did occur at the training facility had to be reported and seen within the facilities, which made for consistent data gathering. Our study also did not measure energy availability or record RWL practices and dynamic weight changes as that would have allowed us to address the issues of RWL. Menstrual history was also not recorded, which is a vital medical component for all young elite female judo athletes. There are also possibilities that injuries may have been unreported due to the athletes’ fear of having to lose time in competition if reported. This is a consistent issue faced regularly among the elite athlete population.
What are the new findings?
-
This study provides comprehensive data of injury rates and trends among the elite judo population.
-
Elite judo athletes average roughly four injuries annually.
-
Women athletes, especially the heavyweights, incur more severe injuries than male athletes.
-
Lightweights incur more injuries than heavyweights in the elite judo population.
How might it impact on clinical practice in the near future?
-
Trainers should be alerted to injuries among the women heavyweight judo athletes as there is a higher probability that it could be a serious injury.
-
Most injuries are of minor severity in the elite judo population.
-
Although many injuries are minor in nature, the Medical Team should be aware that serious long-term injuries do occur, such as in the knee, shoulder, cervical and lumbar spine.
-
Clinicians should address Guidelines and regulations, acknowledging the short-term and long-term harm of continuous rapid weight loss to the body.
Acknowledgments
The authors would like to acknowledge Dr Leisure Yu, MD, Ph D (Loma Linda, California, USA). His many years in the field of sports medicine as Team Physician for the US Figure Skating Association and time served in the Special Olympics has given us valuable insight and direction in the improvement of this paper.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online tables
Abstract in Korean
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Abstract in Korean - Online abstract
Footnotes
-
Contributors K-SK with the data obtained, the data were analysed with the team and K-SK was responsible for the review of all the articles mentioned in the reference section of the paper. K-SK was responsible for writing the paper and discussing with the overseer JKL if any issues were noticed while finalising the paper. KJP has been working with the athletes and speaking with them on a personal level about their injuries. KJP was responsible for the treatment phase of the injured athletes and recording data obtained as they received treatment. After spending many hours by the athletes’ side, KJP was able to obtain and share much information with the team regarding the cause and mechanism of injuries incurred by the athletes. JKL was responsible for overseeing the whole project and gathering the team to start and finish this article. JKL answered all questions any authors had. BYK: BYK was responsible for analysing the data and attempting possible comparisons to run the statistical tests. With the results of the statistical tests, BYK gave direction for the best application of the values to be incorporated into the study. BYK was also in charge of the graphs and tables of the article.
-
Competing interests None declared.
-
Provenance and peer review Not commissioned; externally peer reviewed.