Article Text

Abstract
Aim To summarise the current evidence regarding the effectiveness of physical therapy on pain, function and range of motion in individuals with subacromial pain syndrome (SAPS).
Design Systematic review.
Data sources PubMed, Web of Science, CINAHL, Cochrane, Embase, Lilacs, Ibecs and Scielo databases.
Eligibility criteria for selecting studies Randomised controlled trials (RCTs) investigating physical therapy modalities for SAPS on pain, function/disability or range of motion were included.
Results 64 high-quality RCTs were included. Exercise therapy provided high evidence of being as effective as surgery intervention and better than no treatment or placebo treatment to improve pain, function and range of motion in the short, mid and long terms. The combination of mobilisation and exercises provided high evidence to decrease pain and improve function in the short term. There is limited evidence for improvements on the outcomes with the isolated application of manual therapy. High level of evidence was synthesised regarding the lack of beneficial effects of physical resources such as low-level laser, ultrasound and pulsed electromagnetic field (PEMF) on pain, function or range of motion in the treatment of SAPS. There is limited evidence for microwave diathermy and transcutaneous electrical nerve stimulation. There is moderate evidence to no benefits with taping in the short term. Effects of diacutaneous fibrolysis and acupuncture are not well established yet.
Conclusions Exercise therapy should be the first-line treatment to improve pain, function and range of motion. The addition of mobilisations to exercises may accelerate reduction of pain in the short term. Low-level laser therapy, PEMF and taping should not be recommended.
- Shoulder
- Scapula
- Exercise rehabilitation
Statistics from Altmetric.com
Introduction
Shoulder impingement syndrome is one of the most common causes of shoulder pain and accounts for 44–60% of all shoulder-related symptoms.1 This terminology is currently under discussion because the prevalence of a compression mechanism for the rotator cuff tendons is less frequent than initially proposed, and not likely the predominant mechanism.2–4 Many factors have been associated with this condition, including alterations in glenohumeral and scapulothoracic kinematics,5–7 degeneration and inflammation of the tendons or bursae, weakness or alterations in activity of the rotator cuff and scapular muscles6 ,8 ,9 and capsular laxity or tightness.10 Therefore, we use the term subacromial pain syndrome (SAPS) to describe the condition. SAPS is characterised by pain and functional deficits that are exacerbated with repetitive work performed at or above shoulder level and participation in sports involving frequent overhead motions.6 ,11
Conservative interventions to treat patients with subacromial pain include stretching and strengthening exercises,12–16 joint mobilisation and manipulation,17–20 scapular and proprioceptive training,21–23 taping,24 ,25 acupuncture26 ,27 and many physical modalities.28–30
In a recent systematic review with meta-analysis, Dong et al31 have demonstrated the best treatment options for SAPS. However, most comparisons were performed based on only one randomised controlled trial (RCT). In addition, trials that were analysed included patients diagnosed with calcific tendinitis and rotator cuff tears, which is a different clinical presentation that may occur as a consequence of SAPS, trauma or degenerative changes.32 These facts may have incorporated bias.
Other systematic reviews of physical therapy strategies for SAPS33–35 have included trials independently of the methodological quality and evaluated individuals with other causes of shoulder pain. In one of the reviews,35 only 24% of the trials had a low risk of bias and, therefore, the conclusions were based on low-to-moderate quality of evidence. We aimed to summarise the high-quality evidence of conservative interventions to treat SAPS aiming to provide better guidelines for clinical practice. To achieve this goal, the following criteria need to be met: (1) application of consistent diagnostic criteria for SAPS to exclude other shoulder conditions; (2) inclusion of the available types of isolated or combined physical therapy approaches to treat SAPS; (3) inclusion of high-quality RCTs only and finally, (4) the synthesis of evidence must be based on an updated literature review, using a consistent tool to synthesise the evidence.
This review aims to summarise and analyse the current evidence regarding the effectiveness of physical therapy to improve pain, function and range of motion in individuals with clinical signs of SAPS.
Methods
We used the PRISMA statement and checklist to guide this review. Recommendations from the Cochrane Collaboration for systematic reviews were also followed.36
Selection criteria for including studies
Types of studies
RCTs and quasi-RCTs that compared different modalities of physical therapy were included. Articles in English, Spanish and Portuguese were accepted.
Types of participants
Primary studies which evaluated individuals, males or females aged 18 years or older, diagnosed with SAPS through medical, imaging or clinical diagnosis with at least one of the tests positive, including painful arc, Neer test,37 Hawkins test,38 Jobe test,39 pain with passive40 or isometrically resisted41 ,42 shoulder external rotation, were included in this review.
Articles were excluded if the authors studied individuals with other shoulder conditions (calcific tendinitis, partial or full rotator cuff tears, adhesive capsulitis, osteoarthritis and unspecific shoulder/neck pain) or addressed postoperative management.
Types of intervention
All types of active or passive physical therapy interventions with high methodological quality RCT were included. The experimental group could have been compared with no intervention, placebo or sham treatment, other physical therapy procedures or even with surgical intervention or injection. The intervention could be the only treatment or an add-on treatment. If a combination of therapies was applied, the main intervention and the co-interventions must have been clearly defined to assign the study to a specific comparison group. Non-physiotherapeutic techniques such as surgery, injections and extracorporeal shock wave therapy were excluded.
Types of outcome measures
A study was included if it analysed at least one of the primary outcome measures of interest: pain, function/disability or range of motion.
The duration of the follow-up was defined as: immediately post-treatment (≤1 day); short-term follow-up (1 day to 3 months); midterm follow-up (between 3 months and 1 year); long-term follow-up (≥1 year).
Search methods for identification of studies
Electronic searches
The following databases were searched electronically: PubMed/MEDLINE, Embase, CINAHL, Lilacs, Cochrane and Web of Science from their inception up to April 2015. A Cochrane highly sensitivity search strategy43 was used, that is, all keywords were searched independently and then combined using relevant Boolean terms. Therefore, we used the following Medical Subject Headings terms and key words: shoulder impingement syndrome, shoulder joint, shoulder pain, tendinopathy, rotator cuff, bursitis, physical therapy specialty, physical therapy modalities, rehabilitation, ultrasonic therapy, laser therapy, electric stimulation therapy, massage, soft tissue therapy, acupuncture, dry needling, cryotherapy, taping, tape, pain, pain measurement, range of motion, kinematics, questionnaires, disability evaluation, outcome assessment and quality of life.
Searching other resources
We also screened reference lists from included full-text articles and retrieved systematic reviews for additional relevant publications.
Data collection and analysis
Selection of the studies
All identified studies were initially assessed for eligibility by title to exclude those that were clearly not related to our purpose. Then, abstracts of the selected titles were analysed to determine whether studies met the inclusion criteria regarding study design, participants, interventions and outcomes. Full texts of the potentially relevant articles were retrieved for final assessment and the reference lists were screened for identification of additional relevant publications not retrieved during the electronic search. Data collection was performed through a standardised form. Two independent reviewers (MNH and EDP) performed the selection process and a third reviewer (RFCM) was consulted for final consensus in case of disagreements.
Methodological quality assessment
All studies were scored with the PEDro, which is a critical appraisal tool for experimental studies in physical therapy (http://www.pedro.fhs.usyd.edu.au) based on the Delphi list.44 PEDro is a reliable tool45 and contains eight criteria for assessing internal validity of a study and two criteria for assessing sufficiency of the statistical information displayed. Each criterion can be answered with ‘yes’ or ‘no’. Each item satisfied contributes with 1 point to the final rating scale. Thus, the possible maximum score is 10 points. If a criterion was not described or unclear, no points were awarded.
Methodological assessment of indexed articles presenting the PEDro score was maintained. Methodological quality assessment of no indexed articles was performed by two independent reviewers (MNH and EDP), and inconsistencies of the rating were solved by a consensus with a third reviewer (RFCM). According to Maher et al,45 due to the difficulty of achieving certain conditions, such as blinding of therapists or participants in interventional studies, the maximum achievable score for this type of study would be 8 or 9 out of 10. Then, in order to improve the validity of the evidence and to draw conclusions based on moderate-to-high-level evidence, only studies with a high methodological quality, defined as a minimum PEDro score of 5, were considered on the final summary evidence.44 ,46 ,47
Data extraction and management
Two independent reviewers (MNH and EDP) extracted data regarding participants, settings, interventions, care providers, trial methods, types of outcome measures, frequency of the intervention, duration of follow-up, loss to follow-up, outcome measures and results using a standardised data extraction form adapted from the Cochrane Collaboration model. Disagreements were resolved through consensus. Missing data were either requested from the authors or calculated from mean change, graphical data, SE or baseline SD.36
The included outcome measures were categorised as follows: pain (scores of pain during movement were used when global pain score was not available); function, including function measures with different questionnaires (Shoulder Pain and Disability Index—SPADI, Disabilities of the Arm, Shoulder and Hand—DASH score, Western Ontario Rotator Cuff—WORC index, Shoulder Disability Questionnaire—SDQ, Constant-Murley Shoulder—CMS score or University of California at Los Angeles—UCLA score) and range of motion (flexion, abduction or total range of motion including available range for all shoulder motions).
Data synthesis and analysis
Outcome measures are presented separately. Owing to heterogeneity in the outcomes of the primary studies, it was not possible to perform a meta-analysis. To compare treatment effect, the effect size (ES) of each intervention was calculated with 95% CI for continuous outcomes in each comparison group, considering the values before and after intervention. Treatment effects were further classified as small (<0.20), moderate (between 0.21 and 0.79) and large (>0.80), according to Cohen's criteria.48
Quality of the body of evidence was determined using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach that analyses the following domains: trial design limitations due to risk of bias (using the PEDro score), inconsistency of results, indirectness, imprecision of results and publication bias.43 Ultimately, the quality of evidence for each outcome was presented on a rating system with four categories: high, moderate, low or very low evidence, according to GRADE.49
Results
Description of studies
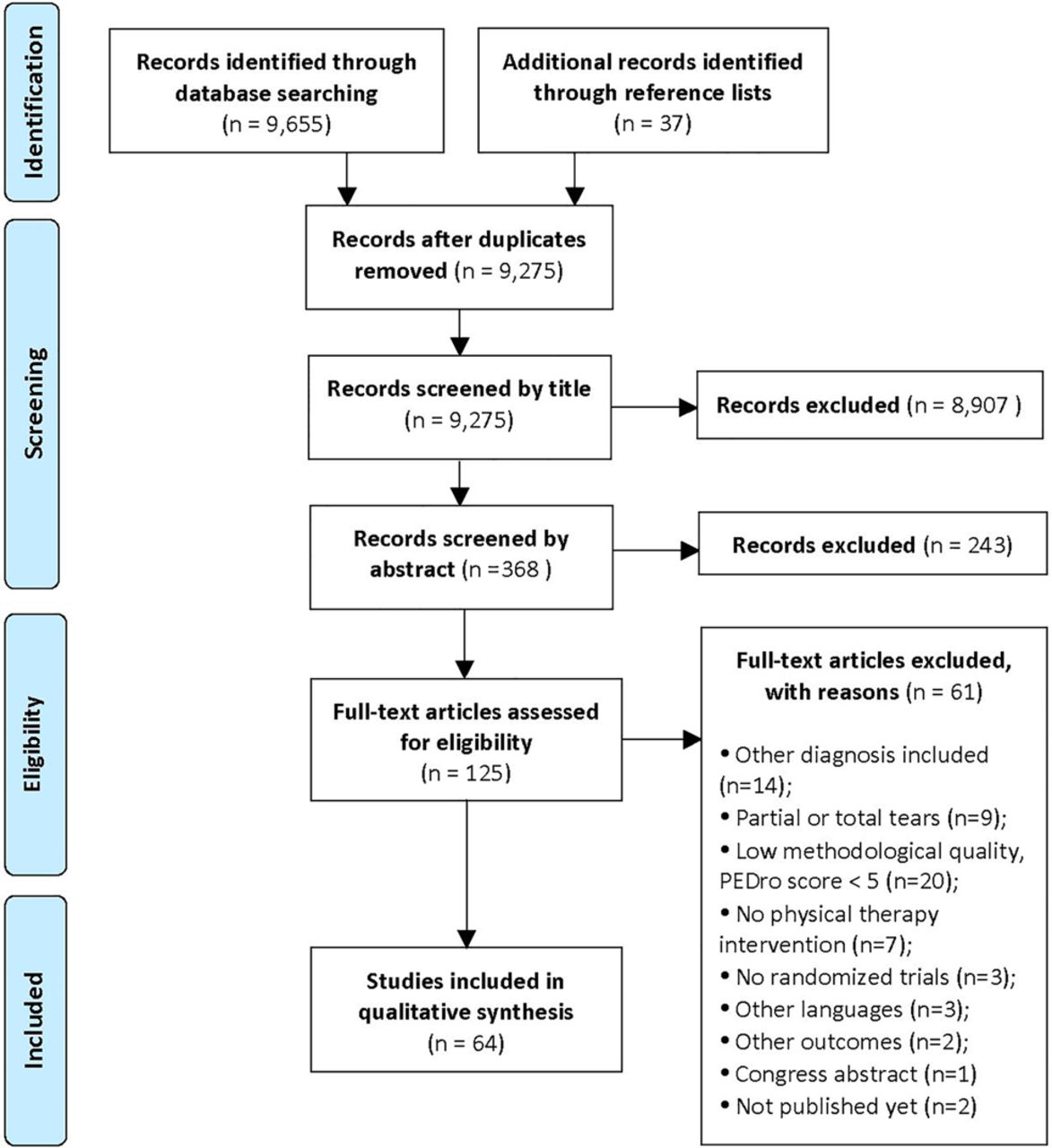
The literature review considered titles published until April 2015. Sixty-four studies fulfilled the criteria for inclusion. Of these, three studies50–52 were follow-ups of the initial studies. A flow chart of the search process with the main reasons for exclusion is shown in figure 1.

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 flow diagram for literature search results.
Quality assessment
Among 64 included studies, six were not indexed in the PEDro database. The quality of these studies was evaluated by consensus of two reviewers (MNH and EDP), using the PEDro scale. A mean PEDro score was 6.9 (range 5–9), which demonstrates high-quality level of the studies. Scores of each study are shown in online supplementary appendix 1.
Supplemental material
The most critical criteria to be satisfied were blinded therapists (92.2%), blinded individuals (64.1%), concealed allocation (46.9%) and intention-to-treat analysis (46.9%). Different specific methods to generate the random allocation sequence such as computer randomisation, random number tables and randomisation cards were used. Only two studies53 ,54 used less appropriate randomisation methods such as allocation based on the order of admittance in the rehabilitation programme.
The quality of the evidence for each intervention analysed according to the GRADE approach is presented in tables 1⇓⇓–4. Reasons for downgrading the quality of the body of evidence are cited in the legends of each table.
Overview of GRADE results for group comparisons concerning intervention with physical resources
Overview of Grading of Recommendations, Assessment, Development and Evaluation (GRADE) results for group comparisons using exercise therapy
Overview of Grading of Recommendations, Assessment, Development and Evaluation (GRADE) results for group comparisons with manual therapy techniques
Overview of Grading of Recommendations, Assessment, Development and Evaluation (GRADE) results for group comparisons using taping
Characteristics of the included studies
Online supplementary appendix 2 shows the characteristics of the included studies and a summary of the results in relation to pain, function and range of motion outcomes. For interpretation of the results, outcomes of interest were categorised as follows. Studies in which the experimental group demonstrated statistically significant results compared with the control group and moderate/high ES of the change compared with the control group were considered as positive results. Investigations that showed no significant result after the intervention, those in which a significant reduction occurred in both groups or those in which ES of the change was equal in both groups were classified as non-effect. When authors described the results as positive based on trends or positive interpretations and results were not accompanied by numerical values of the outcome, these were also considered as non-effect in this review.
Supplemental material
Effectiveness of interventions
Included studies investigated physical resources (n=11 for laser therapy,28 ,55–64 n=5 for pulsed electromagnetic field (PEMF),30 ,52 ,65–67 n=5 for ultrasound,29 ,62–64 ,68 n=2 for microwave therapy,29 ,69 and n=1 for transcutaneous electrical nerve stimulation70), exercise therapy (n=20),15 ,16 ,21–23 ,50 ,51 ,53 ,71–82 manual therapy (n=14),17–19 ,33 ,74 ,83–91 taping (n=6)24 ,25 ,54 ,92–94 and acupuncture (n=4).26 ,27 ,95 ,96 GRADE analysis and synthesis of evidence for physical resources, exercise therapy, manual therapy and taping are presented in tables 1⇑⇑–4, respectively.
Studies that applied therapies in combination and that were described in the primary studies as ‘usual treatment’, ‘conventional treatment’, ‘control therapy’, ‘conservative therapy’, ‘traditional therapy’ or ‘routine therapy’ were labelled in this review as ‘mixed therapy’. These approaches consisted of different combinations of the following: electrotherapy, thermotherapy, phototherapy, massage, strengthening and stretching exercises, scapular and glenohumeral mobilisations and advices to the patients. Interventions that were based on a combination of manual therapy and exercises were labelled as ‘combined therapy’.
Treatments reported in studies were combined into five main clusters: (1) physical resources, (2) manual therapy, (3) taping, (4) exercises and (5) acupuncture. Subsequently, distinctions were made according to the outcomes and comparison groups.
Effects of physical resources The effects of physical resources are presented in table 1.
Laser therapy versus placebo: Six studies compared laser protocol to placebo laser protocol of 6–16 sessions with follow-up of 2–8 weeks.28 ,56 ,58–61 All studies assessed pain, four functions, and four ranges of motion. Pain decreased after laser therapy in three studies28 ,56 ,59 and after both interventions in the other three studies.58 ,60 ,61 Moderate evidence was identified towards a lack of benefit of laser therapy to reduce pain. Laser therapy and placebo improved function and abduction range of motion providing high evidence towards no additional effects over one intervention to another. There is moderate evidence concerning no effect of laser therapy compared with placebo laser on flexion and external rotation range of motion.
Exercises and laser therapy versus exercises only: Three studies added laser therapy to an exercise protocol of 3–12 weeks.55 ,57 ,64 Moderate evidence was found towards no additional benefit of laser therapy to reduce pain or improve function. In the short term, an exercise protocol with or without laser therapy improved pain and function.
Laser versus ultrasound: Two studies62 ,64 compared laser with ultrasound combined with exercises in a follow-up of 2–3 weeks. Both modalities reduced pain and improved function providing moderate evidence towards no additional effects over one therapy to another. Only one study compared 10 sessions of laser and ultrasound therapies in isolation63 in a follow-up of 2 weeks and showed that low laser therapy was better than ultrasound to reduce pain and improve function.
Ultrasound versus placebo: Two studies investigated the effects of ultrasound compared with placebo ultrasound.29 ,68 Moderate evidence was provided for no additional effect of ultrasound over ultrasound placebo on pain and function.
PEMF versus placebo: Five studies compared PEMF with placebo or low dosage of PEMF.30 ,52 ,65–67 There is high evidence of no greater effect of PEMF on pain reduction and moderate evidence of no greater effect of PEMF on improvement of function.
Microwave diathermy versus placebo: Two studies investigated the effects of microwave diathermy compared with placebo treatment.29 ,69 There is low evidence regarding the effectiveness of microwave diathermy compared with placebo to improve pain and function.
Transcutaneous electrical nerve stimulation (TENS) versus injection: Only one study70 compared TENS with intra-articular corticosteroid injection in a follow-up of 3 weeks. Fifteen sessions of TENS or one intra-articular corticosteroid injection improved pain, function and range of motion when associated with an exercise therapy protocol. Therefore, there is limited evidence for the effectiveness of TENS compared with corticosteroid injection.
Effects of exercise therapy Results concerning the effects of exercise therapy are shown in table 2.
Exercise versus placebo or no treatment: Five studies15 ,16 ,50 ,72 ,74 investigated the effects of exercise therapy compared with no treatment or placebo in a follow-up of 6 weeks to 2–8 years. There was high evidence that exercises aiming to restore scapular and shoulder motions are more effective than placebo or no treatment concerning pain reduction and function improvement in the short, mid and long terms. There is moderate evidence that exercise therapy is better than placebo or no treatment to improve range of motion.
Exercises versus arthroscopic surgery: Two studies72 ,73 investigated midterm effects of supervised exercises compared with arthroscopic surgery on pain, function and range of motion. For all outcomes, there is moderate evidence that 2–6 months of supervised exercises were as effective as the arthroscopic surgery after 6 or 12 months. Other two studies with longer follow-ups50 ,51 provided moderate evidence that benefits from both approaches on pain and function were maintained after 2–8 years.
Scapular training versus mixed therapy protocol: Three studies21 ,22 ,77 investigated the effects of scapular focused training compared with mixed therapy protocol using shoulder stretching, strengthening and electrotherapy to improve pain, function and/or range of motion in a follow-up of 1.5–3 months. Low evidence was synthesised towards greater benefits of scapular training over mixed therapy protocol to improve pain, function and range of motion.
Proprioceptive training versus mixed therapy protocol: Six studies23 ,53 ,71 ,75 ,80 ,82 investigated the effects of adding a proprioceptive training to a mixed therapy protocol with shoulder stretching and strengthening on pain, function and/or range of motion in a follow-up of 1–6 months. There is very low evidence for no difference in pain and range of motion results when proprioceptive training was compared with a mixed therapy protocol. There is low evidence that adding proprioceptive training to exercises protocol is more effective than mixed therapy protocol to improve function in the short-term follow-up.
Eccentric training versus rotator cuff strengthening: The effect of adding eccentric training to rotator cuff strengthening exercises was investigated after a follow-up of 12 weeks.76 There is limited evidence regarding the ineffectiveness of eccentric training to improve pain and function when compared to traditional rotator cuff training after 12 weeks.
Self-managed loaded exercise versus mixed therapy protocol: One study79 compared a self-managed loaded exercise programme to a mixed therapy protocol in a follow-up of 3 months. There is limited evidence that self-managed loaded exercise has a similar effect on pain and function when compared with a mixed therapy protocol.
High dosage versus low dosage of exercises: The effects of high dosage exercise therapy compared with a low dosage of exercise therapy were investigated in the short-term, midterm and long-term follow-up.81 There is limited evidence that the high dosage exercise protocol is more effective to reduce pain and improve function 12 weeks, 3 and 6 months after the treatment.
Workplace-based versus clinical-based rehabilitation: One study78 compared a workplace-based rehabilitation programme with a clinical-based rehabilitation in a follow-up of 1 month. There is limited evidence that workplace-based exercises are more effective to improve function than the clinical-based exercises.
Effects of manual therapy techniques
Manipulation versus sham manipulation: Three studies18 ,19 ,91 compared thrust manipulation with sham manipulation in a short-term follow-up (table 3). Very low evidence was provided regarding benefits of thrust manipulations to reduce pain and improve function. Two studies showed no benefits immediately after only one single session of thoracic spine manipulations,19 ,91 whereas the other trial demonstrated that six sessions of shoulder joint manipulations significantly reduced pain and improved range of motion after 2 weeks.18
Mobilisations associated with exercises versus exercises only: Five studies17 ,33 ,74 ,86 ,88 ,88a compared mobilisations in the shoulder girdle, cervical and thoracic spine associated with exercises to exercises only in a follow-up of 3–8 weeks. High evidence was identified for mobilisation associated with exercises when compared with exercises only to decrease pain after 6–10 sessions. Moderate evidence was found towards no additional benefit of adding mobilisations to exercises only to improve function in the short term.17 ,33 ,74 ,88 ,88a It is important to highlight that all studies showed large ES for both approaches. Only two studies74 ,86 evaluated the range of motion and low evidence was identified regarding the effectiveness of mobilisations associated with exercises to increase the range of motion.
Manual therapy versus corticosteroid injection: Two studies83 ,87 compared manual therapy with corticosteroid injection. Low evidence was identified regarding the effectiveness of manual therapy to reduce pain.83 ,87 One study revealed that manual therapy is as effective as corticosteroid injection to improve function after 3 weeks of treatment even in a follow-up of 1 year.83
Manual therapy versus exercises: One study87 assessed pain and another85 investigated function and range of motion when comparing manual therapy with exercises. Additional effects of one therapy over the other were not observed with regard to pain reduction as well as to improvement in function and range of motion after 2–3 weeks of treatment.
Combined therapy versus placebo or no treatment: Two studies74 ,84 compared combined therapy using manual therapy techniques, exercises and scapular training with placebo or no treatment in a follow-up of 6–22 weeks. In the short term, high evidence was identified towards combined therapy to decrease pain when compared with placebo or no treatment. Moderate and high evidence was demonstrated towards combined therapy to improve function when compared with no treatment in the short-term and long-term follow-up, respectively.
Diacutaneous fibrolysis versus placebo or exercises: Only one trial compared diacutaneous fibrolysis with placebo diacutaneous fibrolysis or supervised exercises.89 Then, limited evidence was provided. In the short term of 3 weeks, supervised exercises associated with diacutaneous fibrolysis were more effective to improve function than supervised exercises alone. However, in the midterm of 3 months, both interventions were effective to improve function. Regarding pain and range of motion, supervised exercises alone, associated with diacutaneous fibrolysis or with placebo diacutaneous fibrolysis, demonstrated the same effectiveness to reduce pain and increase range of motion in the short term or midterm.
Effects of taping Results of the effects of taping are presented in table 4.
Kinesio taping versus placebo taping: Three studies24 ,25 ,93 investigated the effect of kinesio taping compared with placebo taping on pain, function and/or range of motion. There is moderate evidence towards no additional benefits of kinesio taping compared with placebo taping to improve shoulder pain, function or range of motion.
Kinesio taping associated with mixed therapy protocol versus mixed therapy protocol: One study54 investigated the effects of kinesio taping associated with mixed therapy based on exercises and electrotherapy compared to mixed therapy alone in a follow-up of 2 weeks. Therefore, there is limited evidence towards no additional benefits of kinesio taping to improve pain and function in the short term.
Kinesio taping associated with a mixed therapy protocol versus manual therapy associated with a mixed therapy protocol: Only one study94 compared kinesio taping associated with a mixed therapy protocol composed by exercise and cold packs with manual therapy associated with the same mixed therapy in a follow-up of 6 weeks. Limited evidence was identified regarding positive effect of the kinesio taping plus mixed therapy only for night pain. Pain at rest and during activity and function showed no differences between both groups.
Rigid taping associated with mixed therapy protocol versus mixed therapy protocol: Only one trial92 compared rigid taping associated with mixed therapy versus mixed therapy. Limited evidence was identified towards no effectiveness of rigid tape in a follow-up of 6 weeks, on pain, function or range of motion, when added to mixed therapy, compared with mixed therapy alone.
Effects of acupuncture
All comparisons below were performed in only one study each. Thus, limited evidence was synthesised concerning the effectiveness of acupuncture in the treatment of SAPS.
Acupuncture versus placebo needling: Only one study95 compared acupuncture with placebo needling in 52 participants with SAPS. Acupuncture was effective to improve shoulder function over the placebo in a follow-up of 4 months.
Acupuncture associated with home exercises versus corticosteroid injection: One study27 compared the effects of acupuncture associated with exercise therapy with injection of corticosteroid in 123 participants with SAPS. In a follow-up of 12 months, acupuncture associated with exercise therapy and corticosteroid injection was equally efficient to improve pain and function.
Acupuncture versus ultrasound: One study26 compared acupuncture treatment with ultrasound treatment in 85 participants in a follow-up of 12 months. Acupuncture was more effective than ultrasound to improve function after 5 weeks of treatment and in 1-year follow-up.
Acupuncture versus mixed therapy protocol: One study96 compared acupuncture associated with dietary advice and hydrolytic enzymes with a mixed therapy protocol in a follow-up of 12 weeks. Acupuncture applied during 30 min once a week was more effective than mixed therapy protocol to reduce pain and improve function after 12 weeks of treatment.
Discussion
This systematic review summarised the effectiveness of different physical therapy interventions in the treatment of SAPS with regard to shoulder pain, function and range of motion. Sixty-four high methodological quality RCTs were included. According to our best-evidence synthesis, rehabilitation based on stretching and strengthening exercises is as effective as arthroscopic surgery in all phases of the treatment, and manual therapy added to exercises is worthy to achieve better results with these patients. On the other hand, taping and physical resources such as laser, ultrasound or PEMF do not add significant contribution to SAPS rehabilitation. Few studies evaluated shoulder range of motion.
All primary studies included in this review had high methodological quality based on the PEDro scale. This fact incorporates significant internal validity and minimal methodological quality limitation based on GRADE analysis. A high level of directness among population, intervention and outcome measures was also present in the included studies. Although SAPS diagnosis is still controversial, studies were included only if all individuals were diagnosed with SAPS based on clinical symptoms or imaging tests. Also, individuals could not present signs of rotator cuff tear, calcific tendinitis, frozen shoulder or other shoulder pathologies. These aspects contributed to reinforce directness in the analysis. Strength of evidence was mostly downgraded to moderate due to imprecision among the comparison groups. Inconsistency and indirectness were the GRADE criteria mostly responsible for downgrading evidence to low or very low.
Exercises and manual therapy effectiveness
Among the five clusters of physical therapy treatments for SAPS identified through the literature search (physical resources, exercises, manual therapy, taping and acupuncture), exercises and manual therapy were the most effective to improve pain, function and range of motion.
Moderate evidence was synthesised towards the same effectiveness of rehabilitation based on exercises and arthroscopic surgery to reduce pain, improve function and increase the range of motion in the short, mid and long terms for patients with SAPS. These results are in agreement with those from Kromer et al33 and Lewis,97 and suggest that patients should not undergo surgery before treatment with exercise therapy aimed at restoration of muscle balance, flexibility and strength of the rotator cuff and scapular muscles. Moreover, rehabilitation with exercises is easy to apply, low cost and presents low risks to the patient since it consists of a non-invasive treatment. Surgery should be handled with care and indication needs to be better established.
Exercise therapy was also strongly recommended instead of no treatment or placebo treatment to improve pain, function and range of motion. This fact reinforces previous recommendations based on moderate evidence98 and also corroborates with Hallgren et al,99 which demonstrated that specific exercises reduce the need for surgery. Concerning types of exercises used in the treatment, there were some interesting findings. There was low evidence regarding the benefits of adding proprioceptive training to exercises protocol to improve shoulder function in the short term. When adding a specific scapular training to exercise therapy, low evidence was synthesised in favour of one or the other programme to improve pain and function. Nevertheless, it is important to emphasise that other outcomes as muscle strength and scapular motion were not included in this review but are usually focused in a rehabilitation programme for SAPS treatment. It should also be highlighted that some studies did not provide enough details regarding the programmes for strengthening rather than reporting target muscles involved in the treatment,73 ,74 while others were more specific in describing the exercise programmes.15 ,16 ,21 ,77 Therefore, consistent comparisons and conclusions about specific types of exercises are difficult to be established.
Different manual therapy techniques were used including mobilisation with movement, shoulder girdle, thoracic and cervical joint mobilisations, soft tissue techniques and neural mobilisations. In addition to the exercises, there was high evidence that manual therapy provides additional benefits in decreasing pain in the short term. Therefore, it can be used to optimise symptoms reduction. A previous systematic review98 and a recent systematic review with meta-analysis35 identified limited and low-level evidence, respectively, that manual therapy either used alone or associated with other interventions significantly reduces pain in individuals with rotator cuff tendinopathy. However, the authors did not rule out the possibility of a small but clinically relevant effect of this therapy.35 It is important to highlight that techniques of manual therapy for different regions (shoulder girdle, cervical and thoracic spine) could achieve different objectives and outcomes. Nevertheless, this was not considered in the current review. Two primary studies included in the review from Desjardins-Charbonneau et al,35 were not included in this systematic review due to low methodological quality,100 ,101 and one due to the presence of individuals with partial rotator cuff rupture.102 We included another clinical trial by Kardouni et al,91 not published at that moment, which strengthened our findings regarding manual therapy effectiveness on pain reduction.
Physical resources effectiveness
Moderate evidence concerning the ineffectiveness of laser therapy to decrease pain was identified. Heterogeneity in the protocols and equipments used has contributed to the differences in energy dosage applied in each trial, and therefore may explain the divergent results. It seems that the dose of energy applied directly contributes to pain reduction since three studies using higher total energy revealed effectiveness of the therapy to decrease pain. This suggestion is supported by a systematic review of low-level laser therapy on acute pain.103 It is important to emphasise that our conclusion was guided by GRADE analysis, in which <75% of the trials did not show additional benefits of laser over placebo laser in the treatment of SAPS. Moderate evidence was also observed towards no additional benefits from laser therapy to improve function and range of motion. A recent systematic review of different types of treatments for SAPS31 reached the same conclusion and did not recommend laser therapy to these patients. No additional benefits were observed with respect to pain or function in the short term when adding laser or ultrasound to the exercise therapy.
PEMF and ultrasound were not more effective than their placebo application to improve shoulder pain and function and should not be advised as part of the treatment based on moderate and high evidence, respectively. A previous review31 identified only a trend towards a benefit from these physical resources. However, few trials were analysed compared to the current review, which strengthened our results.
Microwave diathermy and TENS do not seem to be beneficial in SAPS treatment. The evidence is still low due to the low number of participants and studies available in the literature.
Taping effectiveness
There is moderate evidence that kinesio taping does not produce additional benefits over mixed therapy protocols or placebo taping to reduce pain, improve function or increase the range of motion. Kinesio taping is a widespread technique commonly used in rehabilitation protocols, but its effectiveness does not seem to be related with quantitative measures. Similar results were found following the kinesio taping application in the athletic shoulder. Zanca et al104 did not find changes in scapular kinematics in throwers after taping application, and Aarseth et al105 showed that joint position sense get impaired after kinesio taping in healthy athletes. Furthermore, rigid taping does not seem to be beneficial to any of the outcomes assessed. However, this evidence was based on only one trial.
Acupuncture effectiveness
There is very limited evidence concerning the effectiveness of acupuncture to improve pain and function in comparison with placebo needling, mixed therapy protocols or corticosteroid injection. It is difficult to draw conclusion as comparisons between interventions were made in only one study each. Thus, future studies investigating the effectiveness of acupuncture and dry needling interventions for the treatment of SAPS are still necessary.
Strengths of the review
One of the strengths of this review is the high methodological quality of the included RCTs and their homogeneity among participants. Moreover, the comprehensive search strategy and the best-practice guideline for review were followed as set down by the Cochrane and PRISMA recommendations. These facts have contributed to improved clinical recommendations for the treatment of patients with signs of SAPS.
Previous systematic reviews31 ,98 have shown moderate evidence on the effectiveness of exercise therapy. This review strengthens the clinical recommendations for the use of exercise therapy as the first-line treatment to improve shoulder pain, function and range of motion over surgery or no treatment. This review also provides high level of evidence to recommend exercise therapy combined with joint and soft tissue techniques in the shoulder girdle, thoracic and cervical spine as the best choice of treatment in the short and long terms to reduce pain and improve function in patients with SAPS. Therefore, these results also strengthen previous suggestions of some clinical benefit of manual therapy in SAPS.35 ,98
Finally, despite our strict quality criteria, a high number of studies (64) were analysed in the current review, which contributes to the high consistence of the body of evidence. Thirty-eight of these 64 studies have been published since 2009, the cut-off publication year of the included studies by Gebremariam et al,98 the latest systematic review that studied the effectiveness of physical therapy in SAPS.
Limitations
There was a large number of comparison groups to guarantee clinical homogeneity between most of them. Tools and methods used to measure the selected outcomes were also homogeneous between trials, except for the assessment of function. However, even facing different questionnaires to measure function among trials, the similarity between questionnaires was considered before downgrading a quality point for directness domain. Publication bias was present in only two comparison groups: combined therapy versus placebo/no treatment and scapular and shoulder exercises versus placebo/no treatment. Therefore, two of five GRADE criteria were more difficult to be fulfilled among comparison groups of interventions: consistency and precision. Most of the consistency problems among trials were observed in the statistical results and most of the precision deficits were due to sparse number of participants to draw some conclusion.
Conclusion
According to the body evidence synthetised, exercise therapy aimed at restoring muscle flexibility and strength of shoulder and scapular muscles should be used as the first-line treatment to improve pain, function and range of motion in individuals with SAPS before recommending arthroscopic surgery. There is high evidence regarding the effectiveness of exercises associated with mobilisations to optimise improvements in pain and function. Low-level laser therapy and PEMF are ineffective therapies to reduce pain and improve function in individuals with SAPS. There is no evidence to recommend the use of taping in isolation or combined with exercise to improve pain or function.
Future studies are necessary to better understand the specific effects of manual therapy techniques applied in isolation to enhance clinical recommendations for the treatment of SAPS. Also, future research should address evidence regarding the kind of exercise that should be used to improve specific movement patterns. Finally, more clinical trials are necessary to determine the effectiveness of diacutaneous fibrolysis, microwave diathermy, TENS and acupuncture for the treatment of SAPS.
What are the findings?
Exercise therapy is the best conservative therapy to reduce pain, improve function and increase range of motion in individuals with subacromial pain in all stages of treatment.
Exercise therapy based on stretching and strengthening of rotator cuff and scapular muscles is as effective as surgery intervention.
Exercise therapy associated with manual therapy based on joint and soft tissue techniques is more effective than exercises alone to reduce pain in the short term in patients with subacromial pain.
Low-level laser therapy and pulsed electromagnetic field are no better than placebo treatment or exercise therapy to improve pain or function in patients with subacromial pain.
How might it impact on clinical practice in the future?
Clinicians should prescribe stretching and strengthening of the rotator cuff and scapular muscles as the first-line treatment to improve pain, function and range of motion in individuals with subacromial pain.
Exercises associated with mobilisations may optimise improvements in pain and function.
Low-level laser therapy and pulsed electromagnetic field do not appear to reduce pain or improve function.
There is no evidence to recommend the use of taping in isolation or combined with exercise to improve pain or function.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 88a.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
Footnotes
Funding This work was supported by Grant # 2013/07120 -1 São Paulo Research Foundation (FAPESP).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.