Article Text

Abstract
Background: Despite the growing popularity of women’s football and the increasing number of female players, there has been little research on injuries sustained by female football players.
Purpose: Analysis of the incidence, characteristics and circumstances of injury in elite female football players in top-level international tournaments.
Study design: Prospective survey.
Methods: Injuries incurred in seven international football tournaments were analysed using an established injury report system. Doctors of all participating teams reported all injuries after each match on a standardised injury reporting form. The mean response rate was 95%.
Results: 387 injuries were reported from 174 matches, equivalent to an incidence of 67.4 injuries/1000 player hours (95% CI 60.7 to 74.1) or 2.2 injuries/match (95% CI 2.0 to 2.4). Most injuries (84%; 317/378) were caused by contact with another player. The injuries most commonly involved the lower extremity (n = 248; 65%), followed by injuries of the head and neck (n = 67, 18%), trunk (n = 33, 9%) and upper extremity (n = 32, 8%). Contusions (n = 166; 45%) were the most frequent type of injury, followed by sprains or ligament rupture (n = 96; 26%) and strains or muscle fibre ruptures (n = 31; 8%). The most common diagnosis was an ankle sprain. There were 7 ligament ruptures and 15 sprains of the knee. On average 1 injury/match (95% CI 0.8 to 1.2) was expected to result in absence from a match or training.
Conclusion: The injury rate in women’s top-level tournaments was within the range reported previously for match injuries in elite male and female players. However, the diagnoses and mechanisms of injury among the female players differed substantially from those previously reported in male football players.
Statistics from Altmetric.com
Football is played worldwide by more than 265 million players, of whom 26 million are female players. A survey by the Fédération International de Football Association (FIFA) in 2006 reported that there were over 7 million female football players in the USA, 1.8 million in Germany, 1 million in Mexico and 794 000 in Canada (FIFA, “big count”, 2007). In the Confederation of North, Central American and Caribbean Association Football (CONCACAF), 23% of all football players were women (USA: 40%; Canada: 33%) (FIFA, “big count”, 2007). Women’s football is continuing to grow in popularity—in the past 10 years the number of licensed female football players has increased by 210% in the USA, by 160% in Germany, and by more than 250% in Switzerland.1 The first women’s football World Cup was held in China in 1991, and since 1994 the Olympic Games has included a women’s football tournament. Since 2002, FIFA has organised a biennial U-19/U-20 World Championship for women.
Despite the growing popularity of women’s football and the increasing number of female players, there has been little research on female football players. Several authors have reported the incidence and characteristics of injuries experienced by male players (for a review see Dvorak and Junge2, Inklaar3 and Junge and Dvorak4), but only a few have reported epidemiological data on female football players.5,6,7,8,9,10 Almost all these studies focused on injuries in elite players during the season, with injuries occurring in tournaments mentioned occasionally.11–13
Five studies have reported exposure-related rates of injury in elite female players during the season,5–7,10,14 and one other study analysed leg injuries.8 Three studies were conducted among Swedish teams: Östenberg and Roos10 (123 senior players with different skill levels), Jacobson and Tegner14 (195 premier league players) and Engström et al5 (41 players from the premier league and the second division). Faude et al6 prospectively studied 165 players from nine teams in the German women’s football league over one season. Giza et al7 reported the lowest incidence of match injuries in an analysis of 202 professional female players from the Women’s United Soccer Association (WUSA) during the 2001 and 2002 seasons. They concluded that the rate of injury in WUSA was lower than in the corresponding male professional league. The overall incidence of match injuries in that study was similar to that reported by Östenberg and Ross10 and Jacobson and Tegner14 but substantially lower than the rates reported by Engström et al5 and Faude et al.6 The incidences of match injuries in the two latter studies are similar to those reported among male professional players from different countries15–17 but are still lower than the rates in players from the major US male football league.18
In a survey of injuries occurring during 12 major international football tournaments, Junge et al11 reported that the incidences of injury in female players in the 1999 FIFA Women’s World Cup and the football competition of the 2000 Olympic Games were considerably lower than the rates in the corresponding tournaments for male players. This difference was not observed during the 2004 Olympic Games.12 However, in an analysis of injuries occurring during 10 years of the USA Cup youth football tournament, Elias13 found a lower rate of injury in female compared with male U-19 players.
From the data available for male players, the incidence of injury in tournaments11,19–21 seems to be higher than in matches during the regular season.15–17 Therefore, we hypothesised that the incidence of injury and the cause of injury depend on the level of play. The present study aimed to analyse the incidence, characteristics and circumstances of injuries occurring in top-level international women’s football tournaments.
METHODS
The injury reporting system used in the present study was developed to document injuries during football tournaments.11 It has been implemented in more than 20 international football tournaments,11,20,21 as well as in 6 handball tournaments22 and 8 team sport competitions during the 2004 Olympic Games.12
At a pre-tournament instructional meeting, doctors of all attending teams were asked to report the details of every injury that occurred during a match in an injury report form. They were instructed in the use of the single-page form, on which all injuries during a given match or, when applicable, the non-occurrence of injury, were listed in tabular form.11 An injury was defined as any physical complaint during a match which received medical attention from the team doctor, regardless of the consequences with respect to absence from the rest of the match or training.23 For all injuries the following information was documented:
-
shirt number of the injured player;
-
time of injury (minutes into the match);
-
injured body part and type of injury;
-
circumstances (non-contact, contact, foul play);
-
consequences of injury (referee’s sanction, treatment, time lost in training or match).
The injury reporting forms were available in four languages (English, French, Spanish, German). In the first tournament (FIFA Women’s World Cup 1999) an earlier version of the form was used, which did not include the doctor’s judgment about foul play and the consequences of the injury. For each match, both the teams’ doctors were asked to return the completed form for their team to a medical officer of the FIFA Medical Assessment and Research Centre (F-MARC). Confidentiality of all information was ensured.
Calculation of the incidence of injuries and statistical analysis
The incidence of injury was expressed as the number of injuries per match and the number of injuries per 1000 player hours. The total player exposure hours was computed as11:
11 players/team × 1.5 h × number of returned team injury report forms
We analysed the data using frequency distributions, cross-tabulations, descriptive statistics and χ2 tests. For incidence rates, the 95% confidence intervals were calculated as follows:
95% CI = incidence ± 1.96 × (incidence/square root (number of incidents))
Significance was accepted at the 5% level.
Tournaments
We included seven international women’s football tournaments in the present study: the 1999 and 2003 FIFA Women’s World Cup, the 2002 and 2004 FIFA U-19 Women’s World Championship, the 2006 FIFA U-20 Women’s World Championship and the women’s football competitions in the 2000 and 2004 Olympic Games. These tournaments comprised 184 matches, equivalent to 6072 player hours. A total of 348 injury report forms, covering 5742 player hours, were returned to the F-MARC medical officers. On average, the response rate was 95%, ranging from 73% in the first tournament to 100% in the later tournaments (table 1).
Incidence and characteristics of injuries in major women’s football tournaments
RESULTS
A total of 387 injuries were reported in the seven tournaments, which is equivalent to an incidence of 67.4 injuries/1000 player hours (95% CI 60.7 to 74.1) or 2.2 injuries/match (95% CI 2.0 to 2.4).
The lower extremity was most commonly affected (n = 248; 65%), followed by the head and neck (18%), trunk (9%) and upper extremity (8%) (table 2). The body parts injured most often were the ankle (24%) and head (16%), followed by thigh (12%), knee (11%) and lower leg (11%). Most injuries were diagnosed as contusions (n = 166; 45%), sprains or ligament ruptures (n = 96; 26%), and strains or muscle fibre ruptures (8%). Twelve injuries were diagnosed as a concussion, 13 as a ligament rupture, 9 as a fracture, 8 as a dislocation and 2 as a lesion of the meniscus (table 2). The most common diagnosis was an ankle sprain (n = 61; 16%), followed by contusions of the head (n = 35; 9%), thigh (n = 27; 7%) and lower leg (n = 27; 7%), and by injuries of the knee ligaments (n = 23; 6%).
Diagnosis of injuries with and without time loss
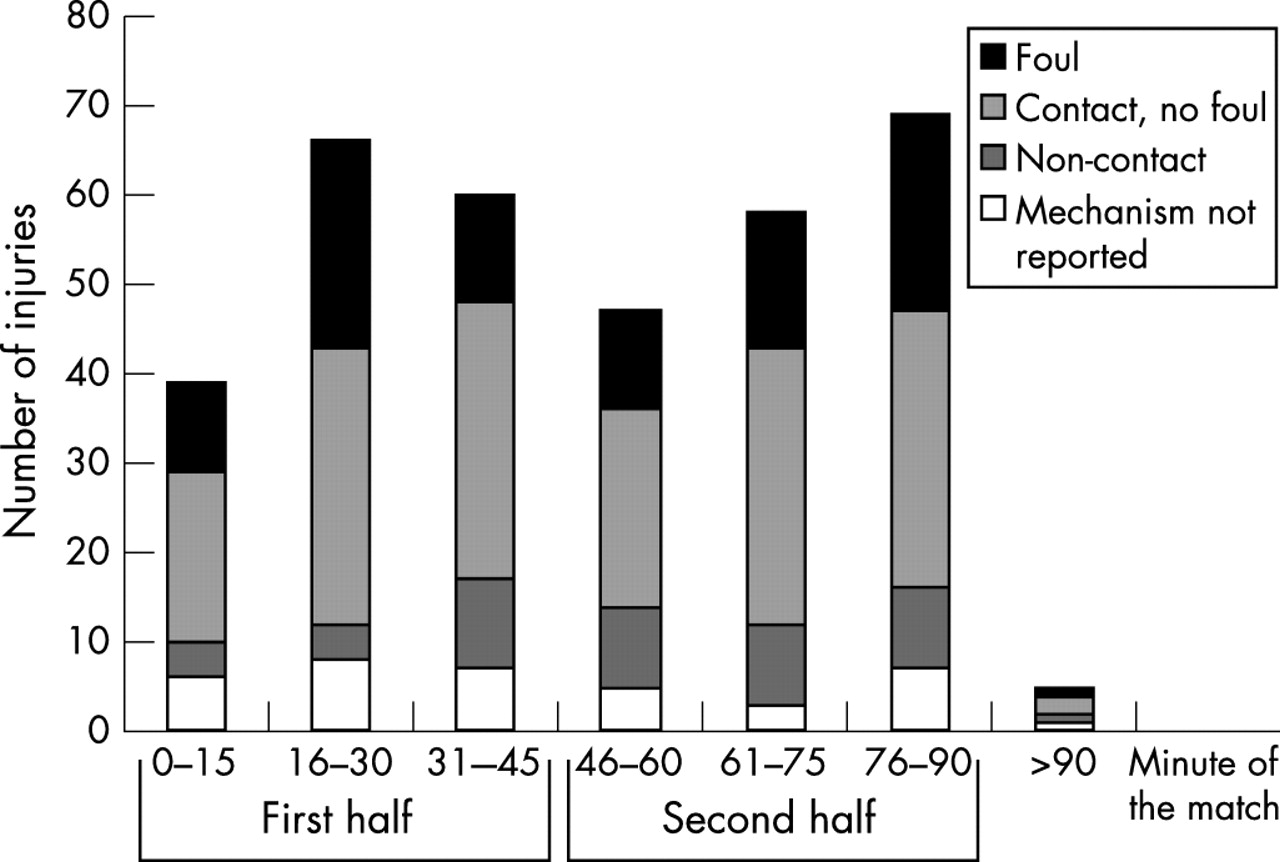
Most injuries were sustained during contact with another player with only 16% (61/378) of all injuries arising from non-contact activities. Of the contact injuries, 35% (97/275), or 29% of all injuries, were caused by foul play based on the judgment of the team doctor and the injured player, but only half of these (49/96) were followed by sanction by the referee. The number of injuries varied during the course of a match, with fewer injuries occurring in the first 15 min of each half than in the remaining time of the match (fig 1). We did not find any significant difference in this respect between the different causes of injury or between injuries with and without time loss.

{kind=link}
Numbers and mechanism of injuries in relation to time in the match.
Information regarding time loss from sport after injury was available for 309 (80%) injuries. Of these, 149 injuries (48%) were expected to prevent the player from participating in match or training. The incidence of time-loss injuries was 30/1000 player hours (95% CI 25.2 to 34.8) or 1 injury/match (95% CI 0.83 to 1.15). It was anticipated that 78% (116/149) of the time-loss injuries would prevent players from participating in a match or training for up to one week, 15 injuries for 8–28 days, and 9 injuries for more than 28 days (4 fractures (ankle, clavicle, wrist, finger n = 1 each), 2 ruptures of the anterior cruciate ligament, 1 rupture of the middle cruciate ligament, 1 patella dislocation, 1 ligament rupture in the lower leg). The expected duration of absence was not specified for 9 injuries (5 ligament injuries of the knee, 1 meniscus injury, 1 thigh strain, 1 fracture of the foot and 1 shoulder dislocation). Injuries with and without time loss differed significantly in terms of the injured body part (p<0.01) and types of injury (p<0.001) (table 2). Time-loss injuries most often affected the ankle (30%) followed by knee (15%), thigh (14%) and head (11%). The most prevalent diagnoses of time-loss injuries was ankle sprain (n = 37; 25%), sprain or ligament rupture of the knee (n = 16; 11%), contusion of the thigh (n = 12; 8%) and concussion (n = 10; 7%).
We did not find any significant difference in the proportion of non-contact injuries that did (20%; 29/148) and did not result in time loss (15%; 23/155), but significantly (p<0.01) more time-loss injures were caused by foul play than injuries that were not expected to result in absence from a match or training (35% v 23%). However, 50% (9/18) of injuries expected to result in absence of more than 28 days or a non-specified duration of time-loss were incurred without contact with another player, compared with only 17% (52/303) of all injuries. Furthermore, five of the seven knee ligament ruptures were non-contact injuries, and six of them occurred in just two of the tournaments (2002 FIFA U-19 Women’s World Championship and 2003 FIFA Women’s World Cup).
On comparing the incidence of injuries in the different types of tournament, we observed a trend towards an increasing rate of injuries from the world cups (1.5 injuries/match, 95% CI 1.2 to 1.9) to the Olympic Games (2.2 injuries/match, 95% CI 1.7 to 2.7) and to the U-19/U-20 world championships (2.7 injuries/match, 95% CI 2.3 to 3.0) for all injuries but not for time-loss injuries. The characteristics and circumstances of injury did not vary significantly among the three types of tournament.
DISCUSSION
The present study explored the incidence and characteristics of injuries during seven major international women’s football tournaments held between 1999 and 2006. The methods used in the study are well established and the strengths and weaknesses have been discussed previously.11,12,21
Incidence of injury
The average incidence of injuries reported in the present study is substantially higher than the incidence of match injuries in elite female players occurring during the season reported by Östenberg and Ross,10 Jacobson and Tegner14 and Giza et al.7 However, it is similar to the rates reported by Engström et al5 and Faude et al.6 Furthermore, it is also comparable with the incidence of match injuries reported for elite male players from different countries.15–19,24,25
What is already known on this topic
-
The popularity of women’s football is growing and the number of female players is increasing.
-
There are only a few published studies on the incidence and characteristics of injury among female players, and almost all of them focus on injuries during the season.
-
From the data available for male players, there seems to be a higher incidence of injuries in tournaments than in matches during the regular season.
In comparison with the injury rates in top-level men’s football tournaments, the incidence of injury reported here is substantially lower than the average incidence reported in 12 major international tournaments (including two for women),11 in the 2002 FIFA World Cup21 and the 2000 Asia Cup.20 Although the injury rates observed in all the seven tournaments analysed in the present study were not significantly different from each other, there was a trend towards an increasing rate from the world cups to the Olympic Games to the U-19 world championships. This could be interpreted as the younger or the less experienced players being more likely to be injured during a major international competition. A similar trend has been observed in men’s tournaments.11 Thus, in the rest of the discussion, the incidence of injuries in female and male football players will be compared with respect to the particular type of tournament.
The average injury incidence in the women’s 1999 and 2003 World Cup was lower than during the men’s World Cup in 1998 (2.4 injuries/match; 95% CI 2.0 to 2.8)11 and in 2002 (2.7 injuries/match; 95% CI 2.3 to 3.1).21 The sex-related difference in the incidence of injury was also observed during the 2000 Olympic Games in Sydney11 but not during the 2004 Olympic Games in Athens.12 This is because of a substantial decrease in the incidence of injuries among male players from 2000 to 2004. The incidences of injury in the U-19/U-20 women’s world championships varied substantially between the three tournaments surveyed, and the same applies to the 1999–2005 U-20 men’s world championships (data from 2003 and 2005 not published).11 However, the mean rate of injury in the four U-20 world championships for male players (3.4 injuries/match, 95% CI 3.2 to 3.7; data partly not published) was significantly higher than the mean of the three U-19/U-20 women’s world championships. Regarding time-loss injuries only, the results were the same, except for a similar mean incidence of injuries in the U-19/U-20 women’s world championships and the U-20 men’s world championships. In summary, the incidence of injury in top-level women’s football tournaments reported here are within the range of the incidence of match injuries during the season for men’s top-level teams, but partly lower than the incidence of injury in the equivalent men’s tournaments.
Location and type of injury
Most of the injuries reported in the present study affected the lower extremity, especially the ankle, knee and thigh, as reported previously for elite male17,18,24,26 and female5–7,10 football players. In accordance with other studies on female football players, ankle sprain was the single most often diagnosed injury.5,9,10,12
Almost all studies on injuries among female football players highlight the high rate of injuries to the knee and especially the anterior cruciate ligament.5–7,10,27 We identified seven ligament ruptures of the knee (including two ruptures of the anterior cruciate ligament), five of which were incurred without contact with another player. The risk of non-contact anterior cruciate ligament injuries in female athletes participating in pivoting sports such as football, handball and basketball is widely recognised28–31 and effective preventive programmes have been developed.32–34
What this study adds
-
The incidence of injury in top-level women’s tournaments in the present study was within the range of the incidence of match injuries during the season in men’s top-level teams but somewhat lower than the injury rate in the equivalent men’s tournaments.
-
Most of the injuries were incurred due to contact with another player as reported previously for match injuries in male players, but in contrast with the corresponding men’s tournaments, fewer injuries were caused by foul play.
-
Head injuries, and especially concussions, were more common in the women’s than in the men’s tournaments.
Head injuries were also a frequent finding in the present study and 12 concussions were diagnosed, which is substantially greater than the numbers reported in men’s tournaments.35 A detailed analysis of head injuries in top-level tournaments35 showed that concussions were more commonly diagnosed in female than in male football players. The authors hypothesised that either the diagnosis of concussion was more cautionary in women’s games or that some concussions in the men’s games were missed and/or were recorded as contusions. The severity of a head injury is not always obvious, therefore careful examination of a player with trauma to the head is highly recommended, and diagnosis and treatment should follow the recently published guidelines.36,37
Circumstances of injury
We found that incidence of injury was similar in both halves of a match but substantially lower in the first 15 min of each half than during the remaining time. Similar patterns, but with a greater increase in the rate towards the end of each half, have been observed during men’s elite matches.21,26,38 However, the injury mechanisms did not vary during the course of the match, as previously described for the 2002 FIFA World Cup.21
Most injuries in the present study were incurred following contact with another player as reported previously for match injuries in men.11,20,21 But in contrast with the corresponding tournaments for men, in which at least half of the contact injuries have been reported to be caused by foul play,11,12,21 only a third of the contact injuries in the present study were caused by foul play. Thus, it seems that the mechanisms of injury differ substantially between male and female football players. Future studies39 should investigate this important aspect, using video analysis of tackling behaviour and injury situations. This method has provided valuable information about injury mechanisms in professional male football players.40–45 Such analyses may provide data for sex-specific preventive interventions to reduce the incidence of injury in women’s football.
CONCLUSION
The incidence of injury in top-level women’s football tournaments in the present study is within the range of values previously reported for elite male and female club players, but partly lower than the rate observed in equivalent international men’s tournaments. However, the diagnoses and the mechanisms of injury differ substantially between male and female football players. Severe knee injuries and head injuries are of particular concern in women’s football. More information relating to injury mechanisms in women’s football is needed to develop specific preventive interventions.
Acknowledgments
The authors gratefully acknowledge FIFA (Fédération Internationale de Football Association) for the funding of this study. We thank Richard Charles, Sonja Schlumpf and Dr Katharina Grimm for their assistance with the data collection. The authors highly appreciate the cooperation of all the team doctors who volunteered their time to collect the data for this project.
REFERENCES
Footnotes
-
Guest editors: Jiri Dvorak, Astrid Junge, Collin Fuller and Paul McCrory