Article Text

Abstract
Objective: To review the diagnostic tests and investigations used in the management of sports concussion, in the adult and paediatric populations, to (a) monitor the severity of symptoms and deficits, (b) track recovery and (c) advance knowledge relating to the natural history and neurobiology of the injury.
Design: Qualitative literature review of the neuroimaging, balance testing, electrophysiology, blood marker and concussion literature.
Intervention: PubMed and Medline databases were reviewed for investigations used in the management of adult and paediatric concussion, including structural imaging (computerised tomography, magnetic resonance imaging, diffusion tensor imaging), functional imaging (single photon emission computerised tomography, positron emission tomography, functional magnetic resonance imaging), spectroscopy (magnetic resonance spectroscopy, near infrared spectroscopy), balance testing (Balance Error Scoring System, Sensory Organization Test, gait testing, virtual reality), electrophysiological tests (electroencephalography, evoked potentials, event related potentials, magnetoencephalography, heart rate variability), genetics (apolipoprotein E4, channelopathies) and blood markers (S100, neuron-specific enolase, cleaved Tau protein, glutamate).
Results: For the adult and paediatric populations, each test has been classified as being: (1) clinically useful, (2) a research tool only or (3) not useful in sports-related concussion.
Conclusions: The current status of the diagnostic tests and investigations is analysed, and potential directions for future research are provided. Currently, all tests and investigations, with the exception of clinical balance testing, remain experimental. There is accumulating research, however, that shows promise for the future clinical application of functional magnetic resonance imaging in sport concussion assessment and management.
Statistics from Altmetric.com
Concussion in sports is common in the adult and paediatric populations. A recent report indicates that 207 830 patients per year with sports related traumatic brain injuries are treated in US emergency departments.1 However, it has been estimated that only 8–19% of sports related head injuries involve loss of consciousness, and the true incidence of sports related head injuries resulting in concussion is probably 1.6–3.8 million people per year in the USA.1 This report estimates that the 5–18 years age group accounts for an estimated 65% of emergency department visits for sports-related traumatic brain injuries.
The overall management of sport-related concussion includes preventive measures, diagnosis, treatment, return to school/work/activity and return to play decisions. The diagnosis of concussion is complicated because many concussions are unrecognised or not reported, especially when there is no loss of consciousness. In cases of uncertainty, additional investigations may be required to assist with the diagnosis. In recognised and documented cases of concussion, sideline assessment can involve the Sports Concussion Assessment Tool (SCAT)2 or the Standardised Assessment of Concussion (SAC).3
However, to monitor concussion severity and recovery, and to assist with prognostication in the concussed athlete, other tools and investigations are required. The use of symptom monitoring and neuropsychological testing, and the return-to-baseline paradigm, is now well established.2 4 However, a multi-faceted approach using additional investigations can be helpful for a thorough management of the injured athlete.
Despite the prevalence of sports concussion in children, most of the research has been directed at the management of young adults, particularly collegiate and professional athletes. Children are different from adults, not only in size, but also biomechanically, pathophysiologically, neurobehaviourally and developmentally.5 6 It follows that a diagnostic test developed and validated in adults may or may not be applicable to the child. The child’s developing brain, and his/her physical, academic, and emotional development, are factors that might influence the neurobiology of the injury, recovery time and management strategy. Moreover, access to immediate assessment in children’s sport is uncommon because the presence of trained medical personnel on the sideline to assess and manage concussion is rare. This situation is considerably different in collegiate and professional sports.7
This review focuses on investigations carried out in research and in specialised clinical management programs. It does not address symptom scales, sideline assessment or neuropsychological testing. These assessment techniques are examined elsewhere within this supplement. Investigations reviewed include structural and functional imaging, spectroscopy, balance testing, electrophysiological tests, genetics and blood markers.
The definition of concussion used in this review is that of the concussion in sport group.2 8 It should be noted that in many of the studies referred to in this review, authors have used the terms “concussion” and “MTBI” (mild traumatic brain injury) interchangeably. The focus of this review is on concussions in athletes; for those other head trauma studies in the literature, we have used the term MTBI to differentiate injuries sustained by civilians. Thus, the reader should note that in this review, when a referenced study examined a civilian trauma sample rather than an athlete sample, the term MTBI is used.
METHODS
The Medline and PubMed databases up to September 2008 were searched using the term “concussion” with each of the following terms: structural imaging (computerised tomography, magnetic resonance imaging, diffusion tensor imaging), functional imaging (single photon emission computerised tomography, positron emission tomography, functional magnetic resonance imaging (fMRI)), spectroscopy (magnetic resonance spectroscopy, near infrared spectroscopy), balance testing (Balance Error Scoring System (BESS), Sensory Organization Test (SOT), gait testing, virtual reality), electrophysiological tests (electroencephalography, evoked potentials, event related potentials, magnetoencephalography, heart rate variability), genetics (apolipoprotein E4, channelopathies) and, blood markers (S100, neuron-specific enolase, cleaved Tau protein, glutamate). The review identified major and seminal publications that focused on diagnostic tests and investigations used in concussion in sport. For those diagnostic tests lacking valid published data in sport-related concussion, relevant publications from the MTBI literature were analysed.
The studies for each diagnostic test and investigation were reviewed and analysed to assess the validity of the diagnostic test and investigation in each of the adult and paediatric populations, as they relate to concussion in sport. For each diagnostic test or investigation, a summary of the data was synthesised for the adult and paediatric populations.
RESULTS
Structural imaging
Computed tomography
By definition, sport-related concussion is associated with normal imaging studies, including computed tomography (CT).2 However, in some individuals CT helps differentiate sport-related concussion from a more serious MTBI. For example, following a head injury, an individual may have a normal neurological examination, yet may be harbouring an intracranial haemorrhage or contusion. For those at risk of intracranial haemorrhage, CT is the investigation of choice. Published recommendations describe risk factors for intracranial pathology in both adults9 10 and children.11 Although CT is essential in the diagnosis of intracranial haemorrhage, it should be noted that it has no utility in diagnosing or assessing concussion per se. Given that a paediatric head CT exposes the child’s brain to 30 millisieverts of radiation,12 it should only be used when clinically indicated.11
Magnetic resonance imaging
Conventional magnetic resonance imaging (MRI) includes T1-weighted, T2-weighted, and fluid attenuated inversion recovery images. These images provide exquisite detail of intracranial and cerebral structure, and can identify occult lesions not visualised on CT, such as small cerebral contusions.13 14 MRI has some advantages over CT, such as multiplanar imaging, better lesion detection, and it does not expose the patient to ionising radiation. Concussion is defined as a functional disturbance rather than a structural injury, and as such, structural lesions identified on MRI help to distinguish concussion from more serious MTBIs.15 Although there are a number of publications evaluating the sensitivity of MRI in MTBI,13 14 16–18 no study has addressed the role of MRI in the management of paediatric or adult sport-related concussion. This explains the absence of guidelines for using MRI as a routine tool in the investigation of concussion. Furthermore, many children, and some adults with claustrophobia may require sedation or general anaesthesia while undergoing MRI and others who have any metal parts in their body cannot undergo this type of examination. In many countries, routine use of MRI for sport-related concussion is not practical or feasible, given the number of available machines, waiting lists and costs.
Diffusion tensor imaging
The movement of water molecules within white matter can be measured by MRI, and diffusion tensor imaging (DTI) exploits the fact that myelin sheaths and cell membranes of white matter tracts restrict the movement of water molecules. Water molecules diffuse in various directions in the brain, but often travel along the length of axons which enables this technique to create images of axons by analysing the direction of water diffusion. DTI provides detailed structural images of white matter tracts in the brain.19 20
DTI has been used primarily in research relating to brain structure and function following civilian TBIs of all severities. It has been used to assess white matter abnormalities following MTBI,21 the length of white matter changes in patients21 with MTBI, and the correlation between white matter damage and simple reaction time.22 These studies revealed that MTBI can affect the structural integrity of axons within the genu of the corpus callosum, resulting in reduced functional anisotropy (FA). Proposed causes of the decreased FA include misalignment of fibres, oedema, fibre disruption or axonal degeneration. These abnormalities correlate with increased reaction time at three months post injury, which is consistent with studies revealing correlations between white matter changes and the persistent concussive symptoms in patients with a history of MTBI compared to controls.23 Although DTI is being used more commonly, its utility in adults has not yet reached the level of diagnostic capabilities.
In a study of children aged 10–18 years with mild and moderate TBI, changes in FA were identified 6–12 months post injury.24 Wilde et al19 assessed adolescents aged 14–17 years with MTBI and normal CT and conventional MRI scans and found altered FA on DTI within 6 days of injury, which they attributed to cytotoxic oedema. Although DTI can be used to identify changes associated with MTBI in some patients, no study has assessed its role in concussion in children, and it therefore remains a research tool. The technique is currently being utilised in prospective studies of acute concussion in high school athletes (University of Pittsburgh), collegiate athletes (University of North Carolina-Chapel Hill, University of Pittsburgh and McGill University) and long-term effects of concussion in retired professional football players (University of North Carolina-Chapel Hill and National Football League MTBI Committee). These studies will attempt to identify the clinical correlates of DTI.
Functional imaging
Single photon emission computerised tomography
Single photon emission computerised tomography (SPECT) involves intravenous injection of a radioisotope (eg, technetium-99m) followed by acquisition of brain images from a scintillation gamma camera. Essentially, SPECT measures regional cerebral blood flow. Some preliminary work in adults with MTBI identified SPECT abnormalities in the medial temporal lobe,25 and a small study on children (ages 2–18) with MTBI suggested that medial temporal hypoperfusion on SPECT was associated with persistent post-concussion syndrome.26 This latter study with children had many scientific limitations, including the lack of clinical data, small numbers, and no neuropsychological assessment. A methodological problem with SPECT is that analyses are typically done by comparing a region of interest in the brain to another part of the same brain that is believed to be normal in function (such as in stroke or brain tumour research). The problem, of course, with traumatic brain injury is that the brain can be affected diffusely. When considering the use of SPECT in children, one must be cognisant of the fact that it does expose the child to a radioisotope, and as such, this limits its use as a widespread routine diagnostic tool. The therapeutics and technology assessment subcommittee of the American Academy of Neurology has cautioned against the routine use of SPECT for the evaluation of patients with mild traumatic brain injury or post-concussion syndrome.27
Positron emission tomography
Positron emission tomography (PET) can be used to measure aspects of cerebral metabolism, including blood flow and metabolic rate for oxygen. PET relies on radionuclides (eg, 2-(F-18) fluoro-2-deoxyglucose (FDG)), produced from a cyclotron, that have very short half lives. Following intravenous injection of FDG, the radionuclide crosses the blood-brain barrier and is taken up by brain cells. The patient is then imaged within the PET scanner and the images display regions of brain metabolism. Preliminary data in adults with MTBI and persistent symptoms up to seven years post injury suggested an area of medial temporal hypometabolism.25 Chen and colleagues28 used PET to study five adults with MTBI and persistent symptoms at rest and during a spatial working memory task. They found normal regional cerebral FDG uptake at rest; however, minor differences emerged during the visual-spatial working memory task. PET does require the use of a radio labelled tracer, limiting its use in children with concussion. Moreover, PET is very expensive and time consuming; it is still a research tool in the field of MTBI.
Functional magnetic resonance imaging
Dynamic techniques, such as fMRI, can offer insights into the pathophysiological and functional sequelae of concussive injuries.29 fMRI studies are non-invasive and do not require the use of a radioactive tracer. fMRI detects the consequence of neuronal activation in cortical matter by observing regional changes in either T1 from increased blood perfusion or T2 from reduced paramagnetic deoxyhaemoglobin levels. The most common approach is based on blood oxygenation changes, and the signal contrast generated has been termed BOLD, for blood oxygenation-level dependent.30
Abnormalities on fMRI have been associated with the presence of post-concussion symptoms (PCS),31 32 and the severity (mild, moderate, severe) of these symptoms.33 Chen et al31 compared brain activations of 16 (15 symptomatic, one asymptomatic) concussed athletes with a group of eight normal controls using working memory tasks. All the athletes but one had subjective complaints of PCS at the time of the functional imaging study. The one symptom-free athlete showed an activation pattern similar to that of the control group, and all the symptomatic athletes displayed a different activation pattern, regardless of whether they experienced loss of consciousness at the time of the injury. Jantzen et al34 performed baseline BOLD activity in eight college football players; four concussed players repeated the fMRI within one week of injury. They found that concussed players had increased BOLD activity during a finger-sequencing task.
Recovery and compensatory patterns may also be seen on fMRI when serial follow-up is available.35 Some researchers have correlated fMRI abnormalities with cognitive test results. Lovell et al32 presented fMRI results for 28 concussed athletes. They performed a measure of working memory (N-back task) using fMRI soon after concussion, and then repeated the fMRI following clinical and neuropsychological recovery. Those athletes with hyperactivation on fMRI at the time of their first scan had a more prolonged clinical recovery than those who did not have hyperactivation.
Normative data is being collected and can now be used to determine whether the BOLD signal change of a concussed individual deviates from the normal pattern, based on the methodology of Chen and colleagues.31 This might be useful for evaluating clinical outcome, especially in cases where symptoms persist and morphological imaging results are normal. In addition to somatic symptoms (eg, headaches and fatigue) and cognitive deficits (eg, concentration, memory and executive functioning), there can be psychiatric complications, such as anxiety, irritability and depression. Most studies on sport concussion have focused on the somatic and cognitive aspects, while the psychiatric dimension remains largely unexplored. Chen et al36 compared fMRI between 24 athletes with concussion who complained of depression, 16 athletes with concussion who did not complain of depression and 16 non-injured control athletes. They found that in athletes with symptoms of depression fMRI results are similar to functional neuroimaging findings in major depression, suggesting that depression following sport concussion may share similar underlying neural mechanisms as major depressive disorder.
Although fMRI has yielded important information relating to neurobiology and recovery in adults with concussion, no study has specifically addressed its use in children. The utility of fMRI depends not only on the technological capabilities of the MRI machine, but also on the paradigms utilised in performing fMRI such as finger sequencing techniques, N-back memory assessment, and other verbal and visual memory tasks. The interpretation of these paradigms in children at different stages of development, and the resultant fMRI correlates, is yet to be established. Furthermore, the paradigms used in fMRI assess focal regions of the brain, and are taken as surrogate measures of global function. To what extent this is true in the developing brain is unknown.
fMRI is relatively expensive and inaccessible for most clinical needs. The BOLD signal is an indirect measure of neural activity, and is therefore susceptible to influence by non-neural changes in the body. Other variables that are difficult to control for such as medications, fatigue, substance use, and pain may play a role and should be taken into consideration when interpreting results.37 fMRI remains at this time a research tool, although its future as a useful diagnostic technique is promising.

Review of serial fMRI studies. (a) Group average serial activation maps from 4 healthy normal athletes with no post-concussive symptoms (PCS). Note: Similar areas of activation suggest reasonable stability of fMRI findings from Baseline Study 1 to Baseline Study 2; (b) Group average activation maps (n = 8) for working memory tasks, superimposed on the group’s average MRI, at baseline (PCS score = 4) and after concussion (<72 hrs; PCS score = 27). Note reduced activations correlate with presence of symptoms immediately after concussion; (c) Group average serial activation maps from another group of four concussed athletes whose symptoms improved from Study 1 to Study 2 compared to five concussed athletes whose symptoms did not resolve. Note: emerging task-related brain activities in the frontal region are observed only in those athletes whose symptoms improved; a lack of activity in the frontal region remains in those with persistent symptoms.
Spectroscopy
Magnetic resonance spectroscopy
Whereas MRI detects signal from water and lipids, magnetic resonance spectroscopy (MRS) detects signals from individual chemicals in tissue. There are two commonly used types of MRS: proton and phosphorus. In proton MRS the four major compounds present are N-acetyl aspartate (NAA), creatine, choline and myo-inositol. NAA, creatine and choline are found in neuronal and glial cells. Myo-inositols are found predominantly in glial cells. Creatine is involved in cellular energy metabolism, myo-inositol is an organic osmolyte, choline is a constituent in the cytosol and cellular membranes and NAA’s function is unknown.38 Lactate, which is used as a marker for anaerobic metabolism, is present in very low levels in control individuals but may be elevated in diseased states. Phosphorus MRS identifies peaks of ATP, phosphocreatine and inorganic phosphate, all of which are involved in the high-energy metabolism of the cells.
Changes in NAA, choline and creatine have been identified on MRS in individuals following traumatic brain injury.39 40 However there is no study examining the use of MRS in concussion. MRS remains a research tool.
Near infrared spectroscopy
Near infrared spectroscopy (NIRS) can be used to detect changes in blood haemoglobin concentrations associated with brain activity. NIRS can be used as a non-invasive technique for evaluating cerebral blood volume and oxygenation, and it has been used to monitor cerebral haemodynamics during exercise following a sport-related concussion.41 When a particular cerebral area is activated, the local increase in oxygenated blood is greater than the amount of oxygen that can be extracted by the brain tissue, such that the proportion of oxygenated and deoxygenated blood changes in the localised region of the brain.42 Blood volume changes using NIRS can be used to provide an estimate of blood flow.43 NIRS remains a research tool in adults and no data are available pertaining to its use in children.
Balance testing
Traumatic injuries to the head and brain can result in temporary or permanent deficits in static or dynamic balance.44–50 In sports medicine, balance testing has been used to document the presence of concussive brain injury and to track recovery.50–53
Balance Error Scoring System
A commonly used measure of static balance and postural stability is BESS.50 51 53 54 The test is rapid, easy-to-administer, and inexpensive. A combination of three stances (narrow double leg stance; single leg stance; and tandem stance) and footing surfaces (firm surface/floor or medium density foam) are used for the test (fig 2). Each stance is held, with hands on hips and eyes closed, for 20 seconds. “Error” points are given for specific behaviours, including opening eyes, lifting hands off hips, or stepping, stumbling or falling.

Balance Error Scoring System (BESS) performed on firm surface (A-C) and foam surface (D-F).
McCrea and colleagues50 reported that BESS scores in concussed college football players changed from baseline on average by 5.7 points, when measured immediately following the game or practice in which the injury occurred. Notably, however, at 1 day post injury, their average BESS score was only 2.7 points greater than baseline. For most athletes, BESS performance returned to preseason baseline levels (average 12 errors) by 3–7 days post injury. These modest changes in BESS performance and rapid recovery of static balance have been reported in other studies with athletes.51–53 In a large study of American collegiate football players, impairment on the BESS was seen in 36% of injured subjects immediately following concussion, compared to 5% of the control group. Of the injured subjects, 24% remained impaired on the BESS at 2 days post injury, compared to 9% by day 7 post injury. Sensitivity values for the BESS were highest at the time of injury (sensitivity = 0.34). Specificity values for this instrument ranged from 0.91 to 0.96 across post-injury days 1–7.55
Significant correlations between the BESS and force platform sway measures with normal subjects have been established for five static balance tests (single leg stance-firm surface, tandem stance-firm surface, double leg stance-foam surface, single leg surface-foam surface, and tandem stance-foam surface), with inter-rater reliability coefficients ranging from 0.78 to 0.96.56 Researchers have reported that BESS performance can be influenced by a number of factors, including the type of sport played,57 a history of ankle injuries and ankle instability58 and exertion and fatigue.59 60 Healthy athletes typically demonstrate a subtle learning (ie, “practice”) effect on the BESS when it is administered over brief retest intervals.61 62 This should be considered when interpreting post-injury results during serial testing.
Several studies have identified BESS deficits ranging from 3–5 days post concussion when compared to baseline and control subjects.50 51 53 The BESS is sensitive to the effects of concussion with and without the use of other brief screening instruments such as a graded symptom checklist and the SAC.55 However, when used in combination with a graded symptom checklist and the SAC, the BESS is more sensitive and specific for accurately classifying injured and non-injured athletes during the acute post-injury phase.50 55 As of 2004, approximately 16% of certified athletic trainers in the USA reported using the BESS to evaluate a concussion.63 Other research has suggested that the test has clinical utility across many age groups.63 64
Sensory Organization Test
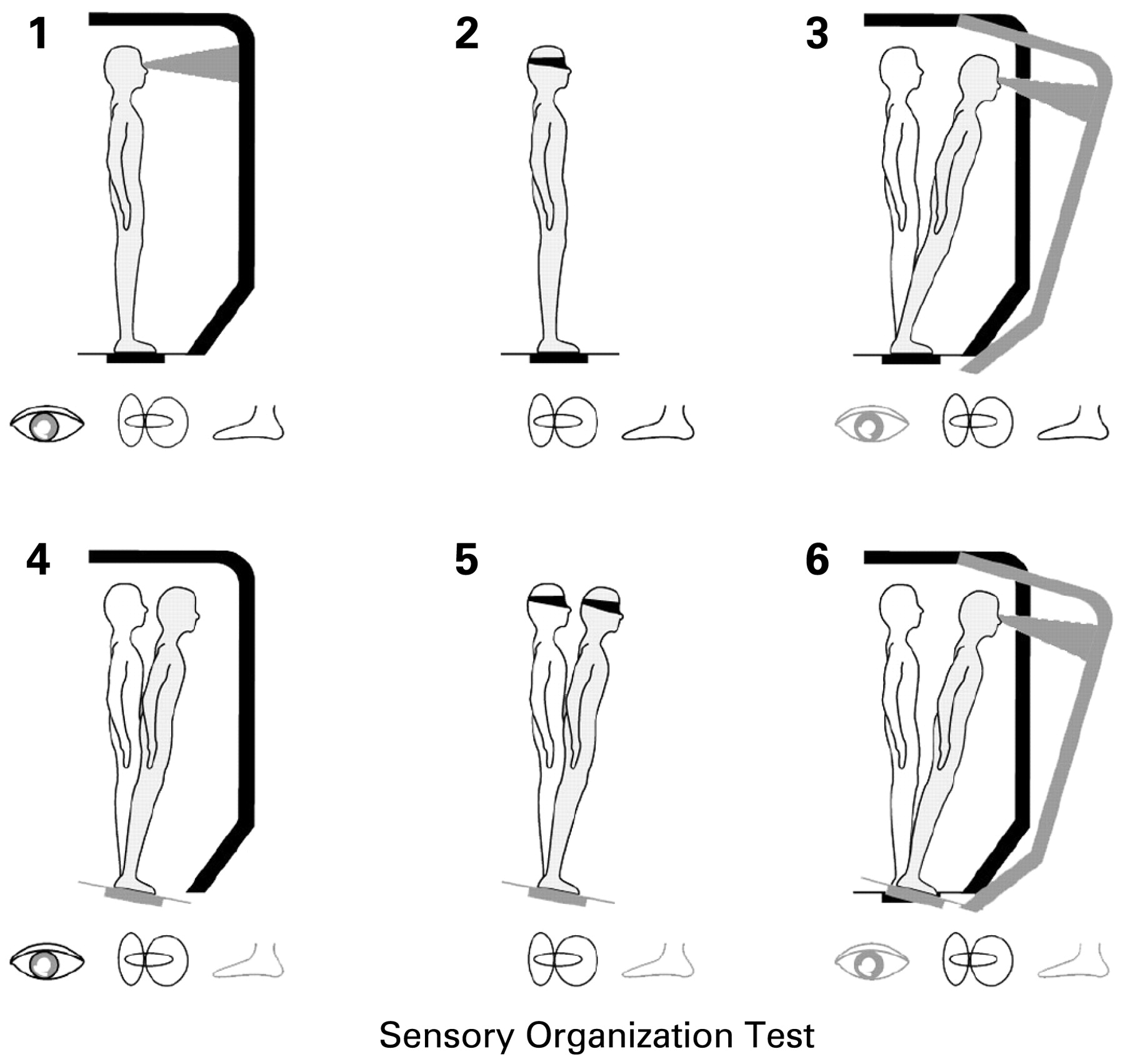
The SOT (NeuroCom International, Inc., Clackamas, OR, USA) is a technical force plate system used to assess balance following concussion.51 65 66 The SOT systematically disrupts the sensory selection process by altering the orientation information available to the somatosensory and/or visual inputs while at the same time measuring the subject’s ability to maintain a quiet stance. Sway referencing is used throughout the test because the movement of the platform beneath the patient’s feet and the environmental surround move in response to the athlete’s anterior/posterior sway. The SOT uses six different conditions; each is performed three times to assess balance (fig 3).

{kind=link}
{kind=link}
{kind=link}
Six testing conditions (1–6) for the Sensory Organization Test used with NeuroCom’s Smart Balance Master.
The SOT appears to be a useful clinical tool for detecting sensory interaction and balance deficits following concussion.51 66 67 Similar to the studies involving clinical balance tests, those using the SOT have identified deficits averaging about 3 days post injury.51 56 These studies indicate that the centres of the brain responsible for coordinating the sensory modalities (thalamus and its interconnective pathways to the cerebral cortex) may be disrupted for periods lasting up to 3 days post-injury. There is a subtle practice effect with both the BESS and SOT, so the absence of this improvement in concussed athletes with repeated testing should be carefully monitored. These studies also suggest that the sensory system most often affected following concussion is the vestibular system and that the system most relied upon by healthy individuals is the somatosensory system.51 More recently, Broglio et al68 illustrated the usefulness of using the SOT as the balance portion of a dual task with attention divided between the balance task of the SOT and another cognitive task. The use of the SOT is mainly confined to a clinic or a laboratory setting because of its technology needs and size; however, it can be useful in difficult cases following a concussive injury and utilised as a more technical and refined measure of balance performance.
One recent study suggested that the test-retest reliability of the SOT in normal controls is low to moderate,65 raising an issue with regard to serial testing. Furthermore, the SOT is not a functional balance task in that it uses a double leg stance throughout. Despite the benefit of altering sensory feedback and detecting sensory interaction deficits, it may not be as sensitive as a more difficult task performed on foam with a single leg.
Gait testing
Parker et al69 examined 29 college athletes (mean age 21 years) who had sustained a concussion and performed neuropsychological testing and gait stability testing on days 2, 5, 14 and 28 post injury. Gait was tested as a single-task, and then while completing a simple mental task (dual-task). A persistent significant difference was noted in the dual-task gait assessment at day 28, although not in the single-task or neuropsychological assessment. Additional research in this area with children and adults is warranted.
Virtual reality
Slobounov et al70 tested balance in eight concussed athletes (age 18–25 years) at days 3, 10 and 30 post injury. Subjects were exposed to a virtual reality image of the room moving. They found that standard balance testing recovered by day 10, but responses to visual field motion remained abnormal at day 30. In all eight athletes, symptoms and neuropsychological testing had returned to baseline. The clinical significance of altered response to virtual reality, rather than to static balance, is yet to be established.
Electrophysiology
Electroencephalography, evoked potentials and event-related potentials
Electroencephalography (EEG) records the electrical properties of neurons by placing electrodes on the scalp. Although EEG has revealed abnormalities post-concussion, its clinical significance is uncertain. Thompson et al71 evaluated 12 male athletes (age 18–25 years) who had sustained MTBI (70–131 days pre-testing) with EEG in four ways: (1) eyes open-seated; (2) eyes closed-seated; (3) eyes open-standing; (4) eyes closed-standing. They found under each condition an overall decrease of EEG amplitude, especially during standing postures, and postural instability was greatest when eyes were closed. The significance of these changes in adult and paediatric sport-related concussion is yet to be established.
Evoked potentials (EP) and event-related potentials (ERP) represent the averaged EEG signal in response to a given stimulus, with EP thought to represent processing in the primary sensory pathways, and ERP being associated with cognitive processes.72 The best known among ERP studies is the P300 component.73–76 Although ERP has good temporal resolution, this technique has poor spatial resolution, which makes it more difficult to localise the brain region responsible for the abnormal activity. Recent studies have reported good sensitivity of ERP for measuring the impact of concussions on cognitive functions in athletes.77–81 In athletes, the presence of symptoms and the number of concussions previously sustained appear to predict the P300 characteristics in oddball paradigms.78–81 The use of ERP in the paediatric population has not been established.
Magnetoencephalography
Due to the current flow within the dendrites, neuronal dendrites oriented parallel to the skull surface produce a magnetic field. This magnetic field can be measured outside the head using supercooled sensors connected to superconducting quantum interference devices. This is the basic principle of magnetoencephalography (MEG). In a retrospective review of 30 adults with persistent (>1 year) symptoms following non-sport-related MTBI (predominantly motor vehicle accidents), Lewine et al18 used MEG, MRI and SPECT imaging, and reported abnormalities in 73% of the patients. They found that MEG findings did not correlate well with psychiatric or somatic symptoms, but there was an association between MEG and cognitive problems.18 However, the lack of baseline neuropsychological data limits the interpretation of these results. There is no data available for use of MEG in paediatric concussion.
The use of MEG is limited because it is expensive and requires installation in magnetic-shielded rooms. Presently there are fewer than 25 whole-head MEG systems in the USA. MEG remains a research tool.
Heart rate variability
Numerous factors play a role in the minute-to-minute changes in cardiac function, including the balance between the sympathetic and parasympathetic nervous systems. During the day, there is greater sympathetic influence on heart rate, while at night there is increased parasympathetic influence. Greater sympathetic activation has at least two effects on cardiac functioning: increased heart rate and decreased heart rate variability. Increased parasympathetic activity that occurs during the night has the opposite effect: decreased heart rate and increased heart rate variability.82
Researchers have examined heart rate variability in children and adults who have sustained severe or catastrophic brain injuries from trauma or other causes.83–87 Power spectral analysis of heart rate variability diminishes in proportion to the degree of neurological injury.88 There appears to be a physiological uncoupling of the autonomic and cardiovascular systems following acute brain injury.88 89
There have been two published studies of cardiac functioning following concussion in athletes. Gall, Parkhouse and Goodman90 examined heart rate response in 14 concussed athletes after they were asymptomatic at rest in comparison to 14 healthy controls. Athletes who had missed playing time had elevated heart rates in response to an exercise protocol on a cycle ergometer relative to control subjects. No significant differences in subjectively reported post-concussion symptoms were noted, however. The differential heart rate response occurred in the absence of obvious changes in post-concussion symptoms, and may reflect a subtle and lingering neuroautonomic cardiovascular effect. These same researchers analysed heart rate variability in these subjects.91 There were no differences in heart rate variability associated with concussion when the athletes were at rest. However, heart rate variability differences emerged following exercise testing. They concluded that the pathophysiology of concussion might not be reflected in neuroautonomic cardiovascular dysfunction at rest, but might be elicited through exertion protocols.
Heart rate variability analyses, in concussed athletes, merits further study. The clinical use of measures of heart rate variability is yet to be established in adult and paediatric concussion.
Genetics
Aolipoprotein E gene
Studies in severe traumatic brain injury have shown that possession of the e4 allele of the apolipoprotein E gene (ApoE4) is associated with worse outcome. Subsequently, the question has been raised as to whether ApoE4 predisposes to worse outcome in concussion. Kutner et al92 examined 53 active American professional football players and performed cognitive testing and ApoE genotyping on each player. They found that those older players who possessed ApoE4 exhibited lower than expected cognitive performance. However, those younger players with ApoE4 did not have a significant reduction in cognitive performance.
Kristman et al93 examined the rate of sustaining a concussion in 318 university athletes and found no significant association between carrying ApoE4 and the rate of injury. Smith et al94 examined fatal cases of traumatic brain injury and found a greater incidence of moderate/severe contusion and ischaemic brain injury in those with ApoE4. They suggest that ApoE may play a role in blood vessel wall integrity and coagulation of blood. This may explain the association of ApoE4 with poor outcome in severe traumatic brain injury, but its role in concussion is yet to be determined.
Terrell et al95 performed a retrospective review of 196 college athletes who completed a concussion history questionnaire, and found an association between the ApoE promoter TT genotype and a history of concussion.95 However, the group with a self-reported history of concussion reported participating in sport for more years than those without a history of concussion.
If ApoE4 does predispose an athlete to a more severe concussion for a given injury, or, as Kutner et al92 suggest, long-term cognitive decline, then ethicists may assert that a child who possesses ApoE4 should be precluded from participating in contact sports. At this time, no study has examined ApoE4 status in children and prospectively observed them during and following their sporting careers.
Channelopathies
Channelopathies are disorders caused by inherited mutations of ion channels.96 A number of channelopathies have been described affecting brain and muscle. For example, the three types of familial hemiplegic migraine are associated with gene mutations on chromosomes 19p, 1q and 2q respectively.96 The possibility that a channelopathy could predispose an individual to more severe forms of concussion or post-concussive migraine is open to conjecture, and could be the subject of future research.
Blood markers
S100 proteins, neuron-specific enolase and cleaved Tau protein
There is considerable interest in blood-based biomarkers of traumatic brain injury in the civilian trauma literature.97–104 Brain serum S-100 protein is a mixture of S-100A1 and S-100B proteins; the S-100B immunoreactivity most commonly cited in the literature refers to the summed concentrations of the S-100B monomers in S-100A1B and S-100BB.105 This protein is found in astroglial and Schwann cells. It is believed to be a fairly sensitive blood marker for brain damage.
Researchers have reported that S100B is elevated following traumatic brain injury of all severities in civilian trauma patients.98 101 104 106 107 There is an association between elevated S100B and structural abnormalities detected on CT scan.98 103–105 107–109 In one study, elevated S100B was associated with lower return to work rates at one-week post MTBI.110 Other researchers, however, have reported weak or no clear relation between S100B levels and neuropsychological outcome.111–113
S100B testing is not widely available in emergency departments. As a blood-based biomarker, it is not very practical to use in sport concussion clinical management or research because it needs to be collected as soon as possible after the injury, ideally within 4 hours. Moreover, there is evidence that S100B (in lower concentrations) can be detected in the serum of athletes engaged in sporting activities114–116 and in civilians with soft tissue or orthopaedic injuries.105 117
A detailed review by Begaz et al118 summarised studies examining S100 proteins, neuron-specific enolase and cleaved Tau protein, and concluded that no biomarker had consistently demonstrated the ability to predict post-concussion syndrome after MTBI. Therefore, these blood markers remain as research tools in the management of adult and paediatric concussion.
Glutamate
Research into excitatory neurotransmitters (eg, glutamate) is proceeding. In a study of autoantibodies to glutamate receptors in children aged 7–16 years with chronic post-traumatic headache, hyper-stimulation of glutamate receptors was reported.119 However, some of these children had sustained cerebral contusions and the application of this testing to paediatric sports concussion has not been established.
Conclusions & directions for future research
Significant developments in the past decade have advanced research into sport-related concussion. This review has examined the use of some diagnostic tests and investigations that can be utilised in a return-to-baseline paradigm similar to neuropsychological assessment. Advanced applications have developed with fMRI and balance testing for assessing concussed athletes with a multi-faceted approach. At this time, all tests and investigations, with the exception of clinical balance testing, remain experimental. There is accumulating research, however, that shows promise for the future clinical application of fMRI in sport concussion assessment and management.
There are several directions for research with fMRI. Important research questions include: (1) Which symptoms are most important and are there particular ones that correlate with fMRI activation patterns? (2) Is there evidence for residual injury after symptoms have resolved, the athlete has returned to play, and he/she is presumed recovered? (3) What is fMRI’s contribution in the paediatric population and will those findings be similar to those obtained in adults? (4) Are there important sex differences?
Balance testing has been examined using different paradigms, such as BESS, SOT, gait testing and virtual reality. Although the BESS is not a truly functional task, it can be administered rapidly, inexpensively and it has evidence to support its validity and clinical use, especially during the acute post-injury period (1–5 days). The BESS is a standardised and objective measure of postural stability and coordination following injury, and can be used as an additional outcome measure when considering return to play. Whether the addition of more complicated balance testing involving dual tasks or virtual reality will improve clinical decision-making is yet to be established. Further research should focus on interpretation of balance testing following concussion within the setting of athlete fatigue, musculoskeletal injury, medication use, different sports, age groups and gender.
Although not appropriate for use in the general clinic, electrophysiological research may provide significant mechanistic understanding in sport-related concussion, in particular the use of MEG combined with other modalities, such as fMRI. At a cellular level, further research into genetics or ion-channels may provide concussion risk-stratification of athletes.
The developing brain in the paediatric population necessitates careful analysis of each test as it applies to the concussed child, with a clear understanding that the child athlete faces the challenge of return to school and learning, in addition to return to sport. Sports-related injury in the child may disrupt already established cerebral functions, and could possibly affect brain development. Research into paediatric sport-related concussion must examine the impact of brain development on diagnostic test interpretation.
This review has described many significant research achievements in the development of diagnostic tests and investigations in sports concussion. A tremendous amount of research and technological advancement will be necessary before most of these investigations have practical clinical value in the day-to-day management of athletes with concussions. Researchers should continue to strive to identify tests that are reliable in the early diagnosis of concussion, that predict concussion severity and duration, that monitor progress and recovery, and provide results that enhance return-to-play decision-making. Such tests must be widely available in the general community, affordable, and be appropriate for use in both adult and paediatric sports concussion.
What is already known on this topic
The current recommendations for assessment of concussion are predominantly clinical, requiring resolution of all symptoms and signs, and the use of return-to-baseline neuropsychological assessment. While anecdotal relationships have been reported between symptomatology and diagnostic tests, many of these relationships are unsubstantiated in the literature. Therefore, the application of diagnostic tests and investigations to the clinical domain is uncertain.
What this study adds
The use of clinical balance testing has developed increasing acceptance in the management of concussion. fMRI and DTI are presently research tools, but demonstrate great potential as clinical tools. Genetic testing and blood markers are yet to demonstrate clinical utility. Electrophysiological research may provide significant insights into the neurobiology of sports-related concussion. The utility of some tools may be less sensitive for diagnostic purposes in the paediatric population compared to the adult population.
REFERENCES
Footnotes
Competing interests: None.