Article Text

Abstract
Objective: To provide an extensive and up to date database for specific running related injuries, across the sexes, as seen at a primary care sports medicine facility, and to assess the relative risk for individual injuries based on investigation of selected risk factors.
Methods: Patient data were recorded by doctors at the Allan McGavin Sports Medicine Centre over a two year period. They included assessment of anthropometric, training, and biomechanical information. A model was constructed (with odds ratios and their 95% confidence intervals) of possible contributing factors using a dependent variable of runners with a specific injury and comparing them with a control group of runners who experienced a different injury. Variables included in the model were: height, weight, body mass index, age, activity history, weekly activity, history of injury, and calibre of runner.
Results: Most of the study group were women (54%). Some injuries occurred with a significantly higher frequency in one sex. Being less than 34 years old was reported as a risk factor across the sexes for patellofemoral pain syndrome, and in men for iliotibial band friction syndrome, patellar tendinopathy, and tibial stress syndrome. Being active for less than 8.5 years was positively associated with injury in both sexes for tibial stress syndrome; and women with a body mass index less than 21 kg/m2 were at a significantly higher risk for tibial stress fractures and spinal injuries. Patellofemoral pain syndrome was the most common injury, followed by iliotibial band friction syndrome, plantar fasciitis, meniscal injuries of the knee, and tibial stress syndrome.
Conclusions: Although various risk factors were shown to be positively associated with a risk for, or protection from, specific injuries, future research should include a non-injured control group and a more precise measure of weekly running distance and running experience to validate these results.
- retrospective review
- running injuries
- risk factors
- multivariate regression
- patellofemoral pain syndrome
- BMI, body mass index
- PFPS, patellofemoral pain syndrome
- ITBFS, iliotibial band friction syndrome
Statistics from Altmetric.com
During the mid-1970s the public enthusiastically began participating in increasing amounts of exercise in response to the merits of activity being realised. This “exercise boom” continued well into the 1980s: between November 1984 and November 1986, about 25 million Americans started to exercise for the first time.1 Running was, and continues to be, the sport of choice for many, because of its convenience, health benefits, and economical nature. However, the potential for running injuries has been well documented in the literature. Macera et al2, in their review of the literature, reported annual rates of running injuries of 24–65%.
Many believe that running injuries result from a combination of extrinsic factors (training errors, old shoes, running surface) and intrinsic factors (poor flexibility, malalignment, anthropometry, previous injury, running experience).1–10 Although extensive research into the causes of running injuries has been carried out over the last 20 years, this work has predominantly focused on injuries occurring in a general sense. Large databases of specific running injuries have been relatively scarce. Although they are unable to accurately determine incidence or prevalence per se, such extensive collections prove useful in providing a measure of frequency of occurrence of specific injuries. Potential risk factors may be analysed and odds ratios computed, based on data provided through retrospective chart review. These data may be compared with similar analyses at the same sport medicine centre to monitor potential changes in the frequency of occurrence of certain injuries over time.
Initially, Clement et al11 studied retrospectively 1819 injuries in 1650 patients seen at the Allan McGavin Sports Medicine Centre (AMSMC) at the University of British Columbia. This report was updated in 1991, when Macintyre et al10 examined 4173 cases seen at the same centre. The purpose of the present study was to provide an extensive and up to date database of running related injuries as initiated at AMSMC some 20 years ago. To the best of our knowledge, no studies of running injuries on a large scale within the general population have been performed in recent years. Furthermore, as suggested by Macintyre et al,10 certain factors may become more influential as a greater percentage of the population participates in running. Therefore, to better understand the current scope of the injuries that runners encounter, it is important to retrospectively review and analyse the profiles of runners seen in a sport medicine clinic.
A model was constructed of possible contributing factors using a dependent variable of runners with a specific injury compared with a control group of runners who experienced a different injury. A major drawback to the external validity of such regression modelling is the lack of differentiation between injured and non-injured runners. Nevertheless, we felt that the distribution of risk factors in the control group in this study would at least be comparable to that in a group of non-injured runners. Moreover, one of the major strengths of this analysis is the introduction of the concept of relative risk for specific injuries. Given the diverse nature and scope of injuries affecting runners, determination of risk factors may be more informative when examined in this fashion rather than from a general context.
METHODS
Patients
A total of 2002 patients with running related injuries were investigated at the AMSMC, a referral facility located on the campus of the University of British Columbia. The patient charts were extracted from a the period 1998–2000, ensuring that the diagnostic criteria were up to date.
Injury definition
Patients were classified as having a running injury if:
-
they had pain or symptoms during or immediately after a run
-
they had pain or symptoms within the approximate time span of beginning a running programme
-
the injury was felt to be related to running
-
the injury was significant enough to force them to stop running or significantly reduce their running mileage and seek medical assistance.
Patient assessment
Patients were referred from their family doctors to the clinic. Sport medicine doctors performed all clinical examinations. Medical consultations typically consisted of an investigation into the nature and history of the injury. This was followed by a physical examination and biomechanical assessment.
Appropriate diagnostic modalities (x ray examination, bone scan, computed tomography scan, magnetic resonance imaging, vascular assessment, and compartment pressure reading) were incorporated as required. In certain cases, referrals were made to specialists in the corresponding field of the injury for further examination and possible surgery. All patients gave consent for their injury profile to be used in the research.
Standard personal data were obtained from each patient during the medical consultation, including activity history (years), weekly hours of activity, height (cm), weight (kg), age (years), and sex. Activity history is a measure of how long the patient has been active on a regular basis (defined as about 60 minutes a week) and was self reported by the patient.
Biomechanical assessment included the following measurements: leg length inequality (>0.5 cm) determined by measuring the distance from the anterior superior iliac spine to the medial malleolus on the supine patient; leg alignment determined by inspecting the distance between the lateral femoral epicondyles with the medial malleoli touching or by inspecting the distance from the medial malleoli with the lateral femoral epicondyles touching for genu varum and valgus alignments respectively; Q angle (defined as >16°) measured as the angle between the line connecting the centre of the patella to the anterior superior iliac spine and the line connecting the tibial tuberosity to the centre of the patella; patellar position—that is, patellar squinting through femoral anteversion—determined by inspection; arch position determined by inspection and classified as low, normal, or high.
History of previous injury to the same anatomical area was recorded. Patients were asked to indicate their running ability based on level of competition entered: recreational, or competitive at provincial, national, or international level. Other concurrent physical activities were noted.
Analysis
Basic descriptives were used for anatomical classification and analysis of biomechanical and baseline characteristics. κ2 2 × 2 contingency tables were used to analyse the sex discrepancy between the 27 most common injuries, with significance set at p<0.05. Multivariate analysis was performed with forward stepwise multiple Wald regression, with selected injury as the dependent variable and all other non-selected patients acting as the control for that analysis. Regression calculation was performed in this manner for each of the 10 most common injuries, across the sexes. Contributing variables included in the model were: height, weight, body mass index (BMI), age, activity history, weekly activity, history of injury, and calibre of runner. In particular, height, weight, BMI, activity history, and weekly activity were categorised with respect to a patient being above or below the respective overall variable mean for the patients in this study (height, 157 cm; weight, 60 kg; BMI, 21 kg/m2; age, 34 years; activity history, 8.5 years; weekly activity, five hours). p<0.05 was used to enter the model. Statistics were compiled using the Statistical Package for Social Sciences (SPSS version 10.0).
RESULTS
Descriptives
In this study of 2002 patients examined at the AMSMC, 926 (46%) were men and 1076 (54%) were women. The most common overuse injury was patellofemoral pain syndrome (PFPS) seen in 331 patients, followed by iliotibial band friction syndrome (ITBFS) (168 cases), plantar fasciitis (158), meniscal injuries (100) and patellar tendinopathy (96). The distribution of injuries was not uniform across the sexes. In fact, there was a statistically significant sex difference in the number of patients experiencing PFPS, ITBFS, plantar fasciitis, meniscal injuries, patellar tendinopathy, Achilles tendinopathy, gluteus medius injuries, gastrocnemius injuries, adductor injuries, osteoarthritis (knee), and sacroiliac injuries (table 1).
Frequency and sex distribution of the 26 most common injuries
The most common site of injury was the knee (42.1% of the total injuries). Other common sites were the foot/ankle (16.9%), lower leg (12.8%), hip/pelvis (10.9%), Achilles/calf (6.4%), upper leg (5.2%), and lower back (3.4%) (table 2).
Breakdown of injury location
Table 3 shows the baseline characteristics for the 10 most common injuries. The mean age ranged from a low of 30.7 years for tibial stress syndrome to a high of 43.2 years for patients experiencing meniscal injuries. Patients with tibial stress syndrome reported the least number of years of regular activity (5.1), while those with Achilles tendinopathy were active for the highest mean number of years (14.5). Mean weekly hours of activity did not vary appreciably between patients with these common injuries, with a mean (SEM) of 5.4 (0.66) reported.
Mean baseline characteristics for the 10 most common injuries
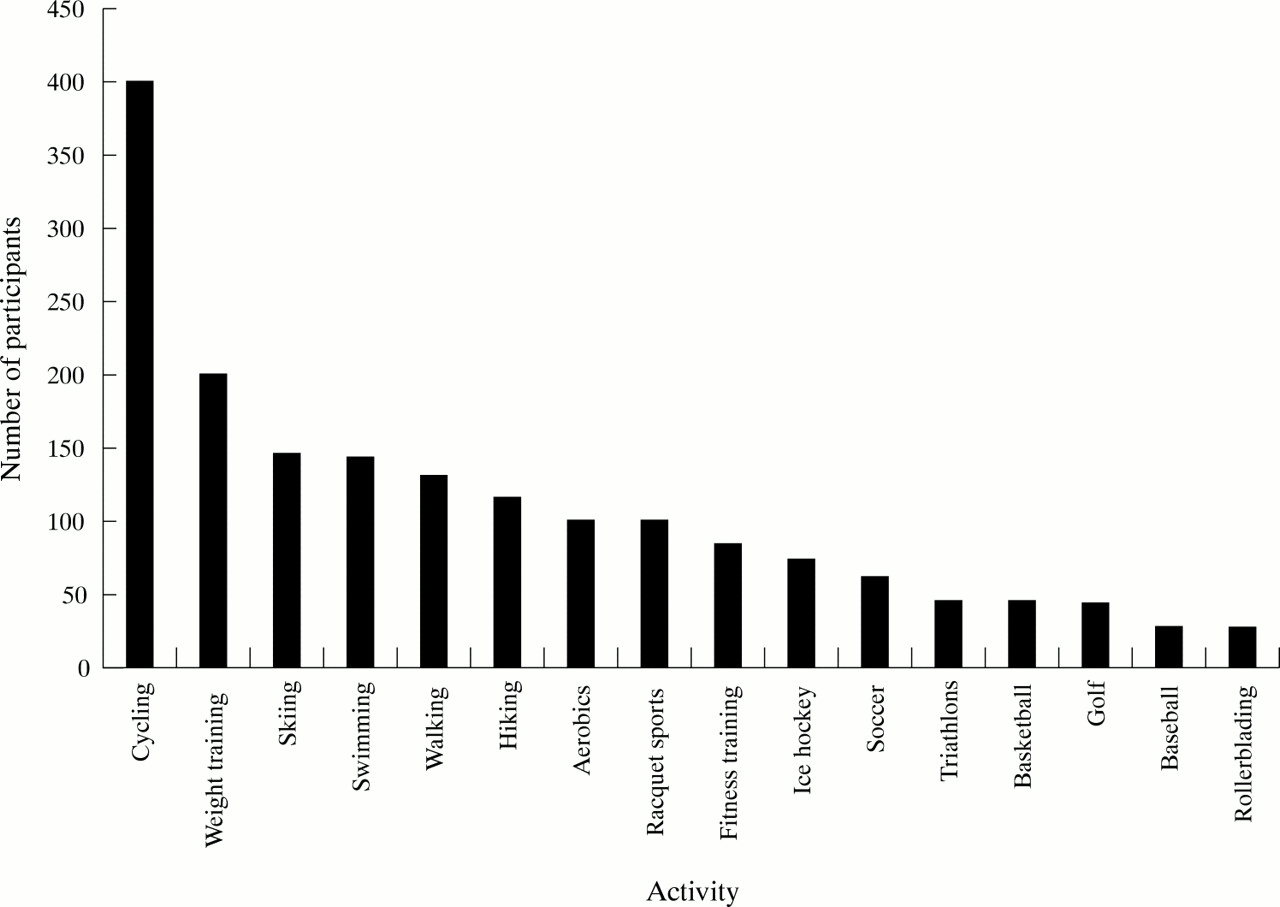
Figure 1 shows patient participation in alternative activities/sports other than running.

{kind=link}
Patient participation in alternative activities/sports.
Biomechanical assessment
Table 4 shows the frequency and types of biomechanical variables seen with the 10 most common injuries. Varus knee alignment was seen in 32% of the patients presenting with PFPS, 33% of those with ITBFS, and 30% of those with tibial stress fracture. Only 18% of plantar fasciitis cases and 16% of spinal injuries were associated with this alignment. Some 29% of the patients presenting with PFPS and 27% of those with patellar tendinopathy had recorded genu valgus, and 19% of the patients with PFPS had patellar squinting resulting from femoral anteversion. One quarter of the patients with patellar tendinopathy had a low arch (pes planus) classification. A high Q angle was found in 6% of patients with PFPS and patellar tendinopathy, and 10% of patients with ITBFS had a pronounced leg length inequality (>0.5 cm).
Biomechanical variables for 10 most common injuries
Multivariate analysis
Table 5 shows factors present in the final models after forward regression. For both men and women, using height, weight, BMI, age, activity history, weekly hours, history of injury, and calibre of runner as possible predictor variables, regression yielded a final model of younger age as a risk factor for PFPS. In addition, women of below average height (mean <157 cm) were at a significantly higher relative risk for patellofemoral pain in this study. On the other hand, increasing calibre and recording low weekly hours of activity (mean less than five hours) were protective against this injury for women.
Multiple Wald regressions: odd ratios (OR) for associated risk factors (95% confidence interval (CI)) for the 10 most common injuries across sex
For ITBS, the final model included lower age (mean <34 years) as a considerable risk factor for men. No variables survived for women with this injury after the regression model.
For patients with plantar fasciitis, the final model showed a lower age as being a protective factor for men, and a lower weight (mean <60 kg) was found to reduce the risk for women. Men of below average height had considerable relative risk of experiencing plantar fasciitis.
For meniscal injuries, lower age appeared as a protective factor for both men and women after regression modelling.
On the other hand, men less than 34 years old were at considerable relative risk for patellar tendinopathy. There were no factors that remained in the analysis for women with this injury.
For tibial stress syndrome, the final regression model yielded men with a below average activity history (<8.5 years) and lower age as relative risk factors for this injury. Women with a below average activity history also had a higher relative risk.
Being less than 34 years old was shown to be a protective factor for men with Achilles tendinopathy. No variables survived for women with this injury after the regression model.
A lower than average BMI (mean <21 kg/m2) in this study was determined to be a risk factor for women for tibial stress fractures and spinal injuries. No variables survived for men with either of these injuries after the final model was calculated.
No significant factors remained in the regression model for gluteus medius injuries.
DISCUSSION
Injury summary
PFPS was the most common injury in the study population. This is supported by other studies.9–12 Of greater interest is the considerably higher incidence of meniscal injuries reported here compared with the study of Clement et al,11 who found only two cases of partial medial meniscal tears in 1819 injuries. The higher incidence in the present study may be due to the increase in the participation of older runners (runners with meniscal injuries reported the highest mean age of 43.2 years), or degenerative changes in the meniscus with prolonged years of running. Alternatively, an increase in diagnostic accuracy in identifying meniscal injuries may be attributed to the greater availability of magnetic resonance imaging.
There is a higher incidence of ITBFS in this study compared with previous years at the AMSMC (4.3% in 198111, 7.5% in 1991,10 and 8.4% 2000). This trend may be a continuation of the hypothesis of Macintyre et al10 which states that changes in footwear construction (such as medial posts or varus wedges) cause runners to adopt a relatively greater degree of supination. However, the recent evidence of Nigg et al13,14 has prompted re-examination of the concept that certain shoe designs, and even shoe inserts and orthotics, have a significant effect on “alignment of the skeleton”. Further research is required to understand the effect of shoes, shoe inserts, and in-shoe orthotics on the incidence of specific running injuries.
Injury breakdown with respect to anatomical location yields the knee as the most commonly injured site (42.1%), with 46% of these injuries being due to PFPS. The incidence of knee injury is similar to previous results: Pinshaw et al9 reported that 44% of all injuries were to the knee (50% were runner's knee), and Clement et al11 found that 42% of running injuries affected the knee, with 60% of these being due to PFPS.
Personal profile data
The sex discrepancy in this study (54% female, 46% male) presents an interesting reversal of injury distribution between men and women since the first retrospective study.11 There has been no change in either the referral structure or the number of women presenting at the AMSMC in the past 20 years. Macintyre et al10 reported the sex distribution to be 56% males and 44% females. Possible explanations for the higher number of female referrals to AMSMC in recent years could be increased participation of women runners and/or women being more inclined than men to seek medical advice. In fact, the figures from the 2000 Vancouver Sun Run 10 km race with 43 998 registered runners (41% male, 59% female) appear to contradict the notion that running is still a predominantly male sport. Regardless of this apparent sex discrepancy in the referrals to this medical clinic, a proper epidemiological analysis comparing injury incidence between men and women cannot be performed with this information. As a result, we are unable to conclude that, overall, women are experiencing more running injuries than men. Marti et al5 and Macera et al2 both conclude, on the basis of population studies in which the type, duration, and intensity of running activities are controlled for, that men and women have similar injury rates.
The considerable differences in sex distribution between certain individual injuries in this study mean that the sex differences are better interpreted on an injury by injury basis. Although there were more women than men in our study, a significantly higher percentage of men experienced plantar fasciitis (54%/46%), meniscal injuries (69%/31%), patellar tendinopathy (57%/43%), Achilles tendinopathy (58%/42%), gastrocnemius injuries (70%/30%), adductor injuries (68%/32%), and osteoarthritis of the knee (71%/29%). On the other hand, certain injuries were significantly more prevalent in women: PFPS (62%/32%), ITBFS (62%/32%), gluteus medius injuries (76%/24%), and sacroiliac injuries (91%/9%). There is a possibility of a distinct trend exhibited by these results. Unfortunately, few published studies have differentiated specific injuries by sex. Macintyre et al10 reported very little difference in the anatomical site of injuries between men and women. This 1991 study also reported that PFPS and ITBFS accounted for more of the injuries in women than in men. Future studies are needed to examine the sex discrepancies for specific injuries. Such research could ultimately increase the efficacy of preventive measures for selected populations.
Patients were asked to indicate if they participated in any other activities/sports on a regular basis apart from running. For certain injuries, some patients participated more in selected alternative activities than others. However, because of the possibility of recall bias, self report bias, and inconsistent patient commitment to these activities, it is difficult to draw any direct conclusions from the data. It is recommended that further research be undertaken to ascertain any statistical significance between participation rates with certain other activities and selected running injuries.
Biomechanical assessment
The results from our biomechanical assessments show higher incidence of specific biomechanical variables for specific injuries. Unfortunately, the same data for a corresponding uninjured population are not available. In addition, it was deemed inappropriate to include the biomechanical measurements in the regression model because of the possibility of examiner bias with respect to a particular injury. As such, the relative risk associated with a given biomechanical variable—for example, varus knee—cannot be appreciated in this analysis. A subjective comparison of certain biomechanical variables across injuries recorded in this study may still be appropriate. There were 17% more observations of pes planus in patients with patellar tendinopathy than in runners with meniscal injuries, and 20% more leg length inequalities recorded for gluteus medius injuries than for tibial stress syndrome.
Multivariate analysis
Being less than 34 yeas old was a risk factor for patellofemoral pain in both sexes and in men with ITBFS, patellar tendinopathy, and tibial stress syndrome. An age below the mean was calculated as a protective factor across the sexes for meniscal injuries and in men with plantar fasciitis and Achilles tendinopathy. The younger patients seen at this clinic may have a higher propensity to be involved in activities that can contribute to the excessive loading of the knee extensor mechanism—for example, soccer and hiking. Unfortunately, the interpretation of this inconsistency is limited by the absence of certain factors that were unavailable during the period of this chart review. Variables such as quantification of the number of sports/activities undertaken by each patient and intensity and frequency of those activities over the period of review may influence the effect of age for a given subject.15 In addition, certain patients may have developed an anatomical adaptation to running and thus may be able to avoid overuse injuries to a larger extent. On the other hand, other patients may experience an injury as a result of the musculoskeletal decay associated with age. Jacobs and Berson8, Macera et al2, and Walter et al16 all report that age was not significantly related to the incidence of running injuries. However, studies of basic military recruits, whose training is relatively uniform and who have little choice about the type and frequency of activities undertaken, show a positive trend for injury with increasing age.15
Patients with a below average activity history (<8.5 years) were found to be at least 2.5 times more likely to experience tibial stress syndrome, independent of the other factors included in the model. However, because the variable activity history is a general measure of activity and does not indicate the amount of time spent specifically running, we are unable to conclude whether the higher relative risk is due to training errors in the inexperienced runner—for example, too much volume before anatomical adjustment to running stress—or participating in some other activity that may confound this analysis. Although this variable may only loosely be associated with running experience, other studies have reported that increasing number of years running is negatively associated with the incidence of injuries.2,5
Being involved with activity for less than five hours a week was found to be a protective factor for women with patellofemoral pain. Again, as we cannot distinguish how many of those hours were spent running (actual time at risk), interpretation of this analysis is difficult. Van Mechelen17 and Brill and Macera18 both concluded, after their respective literature reviews, that increasing weekly mileage is one of the strongest risk factors for injury in runners.
It may be argued that taller or heavier subjects are at a greater relative risk for injury because of the greater forces acting on the bones, muscles, and connective tissue.17 However, it was reported that height did not significantly contribute to the injury rate in an analysis of participants in a community road race.16 We report that men who were shorter than our study average (157 cm) were at a higher relative risk of experiencing plantar fasciitis. While this result takes into account both weight and BMI in the regression model, there may be a correlation between shorter height and musculoskeletal malalignment in these patients. Commonly cited anatomical factors associated with the incidence of plantar fasciitis include leg length inequality, valgus alignment of the subtalar joint, and pes cavus foot type.19,20 In addition, excessive pronation increases the tension placed on the plantar fascia during the stance phase of running.19 Wen et al21 concluded that minor variations in alignment of the lower extremities do not appear conclusively to be major risk factors for overuse injuries in runners.
Women with a body weight of less than 60 kg were at reduced risk of experiencing plantar fasciitis in this study. This is probably explained by the reduced stress/force applied to the foot musculature during running with a lower body weight. However, Walter et al16 did not find a significant association between body weight and running injuries.
Women with a BMI less than 21 kg/m2 were at a higher relative risk of experiencing tibial stress fractures and spinal injuries according to our final regression model. Neely15 suggested that runners with a low BMI may have insufficient lean body mass to compensate for the stresses involved with running, and further points out that women with a low percentage of body fat are prone to amenorrhoea and low oestrogen levels, predisposing them to osteoporosis and reduced elasticity of collagen, thus further increasing their risk of injury. Although BMI is considered a valid estimate of body composition for the general public, its validity becomes uncertain when used for athletes because a larger proportion of their total mass can be attributed to lean tissue. Nevertheless, in a review of risk factors for injury among army basic trainees, it was reported that those within the lowest BMI quintiles had an increased risk of 1.5–2.3.15 Marti et al,5 in their survey of participants in a 16 km road run, found that runners with a BMI of less than 19.5 and greater than 27 were at greater risk of running injuries. Studies by Macera et al2 and Walter et al16 incorporating univariate and multivariate regression, however, reported that BMI was not related to the incidence of injury in runners.
Take home message
The most common overuse running injury 20 years ago was patellofemoral pain; this is still the case today. Iliotibial band friction syndrome is now the second most common injury. Overuse injuries result from a complex of training errors (including lack of specific strength and flexibility), inappropriate surface and terrain, biomechanical lower extremity malalignment, and inappropriate footwear.
Having a prior history of injury has been associated with an increased risk of injury in previous studies.2,5,16 It has been suggested that those with a previous injury may be more likely to experience reinjury because the original cause may remain, the repaired tissue may function less well or be less protective than the original tissue, or the injury may not have healed completely.22 A positive history of injury in the same anatomical area was not found to independently contribute to any of the injuries in this investigation.
Similarly, being documented as a “high calibre” runner was not a significant contributor to injury, after accounting for age, weekly hours, and number of years of activity. The relation between running calibre and the incidence of specific running injuries has not been well investigated, perhaps because of the subjective nature of the definition of “running calibre”. In their retrospective analysis, Macintyre et al10 investigated injury rates between three groups of runners: elite middle distance, marathon, and recreational. Recreational runners had the highest incidence of knee injuries (PFPS), whereas lower leg and foot injuries (tibial stress fractures) were more prevalent in the elite middle distance class, and marathon runners had the highest rate of ITBFS.
Running calibre in this study was designated according to whether the patients ran recreationally and locally or competed in provincial, national, or international competition. It is not unreasonable to assume that runners of higher calibre typically run at a higher intensity, over a greater weekly distance, and have a prior history of injury, thereby predisposing them to further injury.2,, 3,, 5––7 However, Macera et al2 concluded that high calibre runners probably have more running experience and a greater ability to “listen to the language of their body”, both of which are thought to contribute negatively to the incidence of running related injuries. Owing to the conflicting opinions on how running calibre influences injury patterns, further investigation into the possible relation between running calibre and injury is advocated.
Conclusion
The knee was the most common injury location in this retrospective survey analysing injury patterns among 2002 patients seen at the AMSMC. The five most common injuries were PFPS, ITBFS, plantar fasciitis, meniscal injuries, and patellar tendinopathy. In addition, certain injuries occurred with a statistically significant higher frequency in one sex than the other. The higher incidence of meniscal injuries in this study compared with two previous studies carried out at the AMSMC over the last 20 years is noteworthy. Being less than 34 years old was reported as a risk factor across the sexes for PFPS, and in men for ITBFS, patellar tendinopathy, and tibial stress syndrome. Being active for less than 8.5 years was positively associated with injuries in both sexes for tibial stress syndrome; and women with a BMI less than 21 kg/m2 were at significantly higher risk for tibial stress fractures and spinal injuries. A past history of injury and increasing calibre of runner were not significantly associated with any injury in this investigation. Although men shorter than 157 cm were at a considerably higher relative risk of experiencing plantar fasciitis, it is our opinion based on prior research that this variable probably correlates with another pathological variable not included in the model, such as malalignment or weekly running volume.
Acknowledgments
The authors would like to acknowledge the Nike Research Foundation and the BC Sport Medicine Research Foundation for their support.