Article Text

Abstract
Background: The Active Script Programme (ASP) aimed to increase the number of general practitioners (GPs) in Victoria, Australia who deliver appropriate, consistent, and effective advice on physical activity to patients. To maximise GP participation, a capacity building strategy within Divisions of General Practice (DGPs) was used. The objectives of the programme were to (a) train and support GPs in advising sedentary patients, and (b) develop tools and resources to assist GPs.
Objective: To evaluate the effectiveness of the ASP.
Methods: A systems approach was used to promote capacity in Victorian general practice. Economic analyses were incorporated into the programme’s evaluation. Participants were selected DGPs and their GP members. The programme worked with DGPs to train GPs and provide relevant resources. The main outcome measures were (a) changes in GP knowledge and behaviour and (b) cost effectiveness, based on modelled estimates of numbers of patients advised and adopting physical activity and gaining the associated health benefits.
Results: GP awareness and provision of physical activity advice increased. Although the programme’s reach was modest, based on actual GP involvement, the cost effectiveness figures ($138 per patient to become sufficiently active to gain health benefits, and $3647 per disability adjusted life year saved) are persuasive.
Conclusions: The ASP increased DGPs’ capacity to support GPs to promote physical activity. There is a strong economic argument for governments to invest in such programmes. However, caution is warranted about the maintenance of patients’ activity levels. Programme refinement to encourage GPs to use community supports more effectively will guide future development. Further research on long term patient adherence through a multisectorial approach is warranted.
- physical activity
- exercise
- general practitioners
- population health
- ASP, Active Script Programme
- DALY, disability adjusted life years
- DGP, Division of General Practice
- GP, general practitioner
Statistics from Altmetric.com
- ASP, Active Script Programme
- DALY, disability adjusted life years
- DGP, Division of General Practice
- GP, general practitioner
The Active Script Programme (ASP) was established in 1999 to increase the number of Victorian general practitioners (GPs) who deliver physical activity advice to their patients in a consistent, appropriate, and effective manner. The ASP was initially developed and implemented across eight Divisions of General Practice (DGPs) (phase I, 1999–2000).1 In phase II (2000–2001), the programme was maintained in six of these DGPs and rolled out to a further three. DGPs used matched funding to employ part-time divisional liaison officers, who worked closely with a centralised team to implement the programme’s strategies. Liaison officers usually conducted their ASP role in conjunction with other divisional responsibilities, both related and unrelated to physical activity promotion.
Physical activity can modify risk factors for a range of conditions including cardiovascular disease, diabetes, arthritis, stroke, cancer, mental illness, and falls injury and promote general wellbeing.2 In Australia, direct healthcare costs attributable to inactivity are conservatively estimated as $377 million per year.3 In Victoria alone, physical inactivity is estimated to be responsible for 6.6% of the disease burden.4 Previous economic evaluations of physical activity interventions suggest that programmes conducted in general practice can be cost effective.5–8 It was the aim of this study to assess the success and cost effectiveness of the ASP among GPs in Victoria, Australia
METHODS
The programme used a systems approach,9 engaging GPs through existing infrastructure (DGPs) to develop a multifaceted, effective, sustainable public health strategy. It maximised the efficiencies of a centralised expert team in disseminating the programme, while being sufficiently flexible to accommodate cultural and contextual differences across different DGPs. It aimed to build the capacity of both GPs and DGPs10 to enable sustainability of the interventions. This emphasis on capacity building extended the programme’s scope beyond that of its contemporaries in New South Wales (Active Practice) and New Zealand (Green Prescription).
Participants
All Victorian DGPs (31) were invited to submit expressions of interest, outlining how the ASP’s goals linked to their strategic plans, a measure of existing capacity. Suitable DGPs were selected. Sixteen DGPs responded in phase I, and eight were selected on the basis of criteria showing that they were focused on areas relevant to physical activity in their current strategic plans. Similarly, in Phase II, three further DGPs were selected following expressions of interest from seven of the 23 remaining DGPs.
Design
The programme was developed and implemented using an action research approach. Independent evaluators assessed achievement of programme objectives. Cost effectiveness analyses were used to compare the programme’s effectiveness with routine care. These analyses provided a longer term view of the impact of physical activity advice on health gain and cost effectiveness based on elements of a real programme (ASP); other studies have focused on short term gains and estimates from the literature.
Intervention
Capacity building was underpinned by elements of leadership from the central management and the establishment of a working partnership with divisions. Resources and interventions were developed in consultation with participating DGPs, using the best available evidence. Workforce development, organisational development, and resource allocation subsequently occurred. To influence GPs’ behaviour, attitudes, skills, and knowledge, a range of resources was produced. An ASP kit, disseminated to all GPs, incorporated a GP information folder, script pad, assessment tool, surgery poster, and patient record stamp. Awareness was raised through newsletters, supplemented by local media exposure. GPs were trained through seminars and individual practice visits. Practice visits followed a formal structure to disseminate information and resources; they were supplemented by phone calls or revisits as appropriate. Participating GPs could opt to conduct a clinical audit. The programme also endeavoured to establish referral and collaboration systems between GPs and community providers of physical activity—for example, local government, leisure centres, allied and community health services, and peak organisations such as Bicycle Victoria and Parks Victoria.
Evaluation method
To assess changes in GPs’ behaviour, attitudes, skills, and knowledge, GP fax back surveys were sent to participating GPs at the start of phase I and completion of phase II. These data were triangulated with patient feedback data. The patient sample was recruited through the GPs who participated in the programme’s clinical audit. In depth telephone interviews were conducted to ascertain patients’ views on the role of GPs in promoting physical activity, the utility of written scripts, and the impact of the advice on their activity levels.
Assumptions for the economic analyses
Programme effectiveness assumptions
-
52% of the GPs who became involved in the ASP provided advice more frequently or systematically (based on GP self report)
-
20% of patients advised by the above GPs would become active in the short term, with 50% of the advised patients becoming sufficiently active to accrue a health benefit in the long term
(In real terms this meant that a conservative estimate of 10% of patients who had seen trained GPs and been advised would be active in the long term.)
Modelling assumptions
-
The ASP programme is evaluated in a “steady state” of operation—that is, the year evaluated is representative of a fully functioning and effective ASP
-
The “routine care” comparator assumes that GPs are not providing advice in a systematic way; that they advise only 10% of their patients and that only 5% of these advised patients become more active. The comparator also assumes that 50% of these patients remain active
-
A “standardised approach to GP activity”. This means that all GPs are assumed to provide “routine care”—that is, advise 10% of sedentary patients—and that GPs in the ASP were assumed to increase advice at two levels: “more frequently” (advised 30% of sedentary patients) and “systematically” (advised 45% of sedentary patients)
-
The “average” GP is full time and has a practice population of 916 patients, of whom 290 are in the age range 20−75 and are sedentary—that is, not active enough to accrue a health benefit
-
The government expenditure (State and Commonwealth) is taken as the economic cost for one year (July 2000–June 2001)
-
The cost offsets are calculated for the six major diseases for which a clear and substantial causal relation is associated with increased physical activity levels14,15
-
The total catchment population in the nine DGPs is 1 379 634,16 and the number of adults (20–75 years old) who were not active enough to accrue a health benefit was 410 32316,17
-
The total number of non-specialist medical practitioners in the nine divisions (1998–1999) was 1548. (The Commonwealth Government Health Insurance Commission data on GP activity in the 1998/1999 period for these nine DGPs totals 1548. This figure includes full time, part time, and casual GPs. The corresponding previous year period has the same number of GPs, indicating a stable population.) Non-vocational registered GPs are excluded from this population.
Data analysis
The programme’s overall achievements were evaluated using a public health promotion evaluation model (RE-AIM)11 to assess the programme’s reach, efficacy, adoption, implementation, and maintenance at DGP and GP levels. Findings using this model have been published elsewhere.12 The framework incorporated five domains:
-
Reach—the proportion of the target population that participated in the intervention;
-
Efficacy—the impact of an intervention, positive or negative;
-
Adoption—the proportion/representativeness of settings that have adopted the intervention;
-
Implementation—the extent to which the intervention is implemented as intended;
-
Maintenance—the extent to which the intervention is institutionalised at individual and systems level.
The economic evaluation focused on cost effectiveness rather than efficacy per se. A cost effectiveness analysis using a modelling approach was developed to compare the ASP (an organised approach to exercise counselling) with routine GP care (based on BEACH data13). It was exploratory in nature, for two reasons: (a) the ASP was in a formative stage of development; (b) the results relied on a variety of programme effectiveness assumptions to model long term health outcome. A literature review on the cost of illness attributable to inactivity and past economic evaluations of physical activity programmes in primary care settings guided this cost effectiveness analysis. Increased GP screening and provision of advice to patients were used as key indicators of cost effectiveness.
The focus was on health sector costs at governmental level, which included ASP running costs and GP consultation costs paid by government (Medicare). Private sector costs, particularly those of patients and their families, were excluded. Allocative efficiency—that is, whether the programme was worth while (“value for money”)—was examined. The cost effectiveness analysis model used assumptions derived from the ASP and evidence from the literature (see the box). Two activity levels were identified for this study: (a) patients not active enough to accrue health benefits (<3.3 MJ (800 kcal) expended a week); (b) patients active enough to accrue health benefits (>3.3 MJ expended a week). The cost effectiveness analysis was thus able to identify the level of change required for health benefits across the population.
The outcome measures for the economic evaluation were the number of: patients screened; patients who become active; patients who accrue a health benefit; disability adjusted life years (DALYs) averted; premature deaths averted. The direct healthcare costs accruing from a reduced prevalence of sedentary people were estimated and deducted from the programme cost to provide an estimate of the programme’s net cost. Opportunity costs, net financial cost saving, and health benefits were estimated using the proportional attributable risk approach, plus epidemiological data on the six diseases most closely associated with physical inactivity (coronary heart disease, non-insulin dependent diabetes, colon cancer, breast cancer, stroke, and depression).14,15 Routine care associated with the identified health benefits was also costed. These costs and benefits were deducted from the ASP. Time lags were incorporated assuming that, for all diseases, a protective effect occurs after two years.18,19 Cost per DALY averted and cost per premature death averted were estimated.
A univariate sensitivity analysis was conducted on key areas of uncertainty (based on assumptions of numbers derived from ASP experience): number of GPs involved, the number of patients screened, the percentage of patients to become active in the short term, and the percentage of patients to accrue a health benefit. There was no evidence available on longer term benefit,18,19 thus uncertainty arose in modelling the longer term health gain. To address this, the potential cost effectiveness was modelled assuming a 50% attrition rate over time in patients sufficiently active to accrue a health benefit. This estimate was based on previous published studies in the primary care setting with a follow up beyond 12 months20–22 and could potentially be improved by establishing effective referral linkages to community providers of physical activity such as those of the Green Prescription Programme in New Zealand.23
RESULTS
Reach of programme
Phase I involved 338 GPs, approximately one fifth of all GPs within participating DGPs. In phase II, 332 additional GPs (a further 23% of GPs) were involved in the programme’s activities, totalling 670 GPs for phases I and II. GP involvement included two components: attending training seminars or receiving an individual practice visit for academic detailing by a liaison officer (table 1).
Number of general practitioners involved in Active Script Programme activities
Adoption, implementation, and maintenance of the programme
Copies of actual scripts written (628) from 83 of the phase I GPs were available for analysis at the end of phase I. This figure represents about 60% of the 1035 scripts returned. The remainder were received after the phase I evaluation period and were thus not available for analysis.
Table 2 illustrates characteristics of the scripts’ usage by the GPs. Weight control was the most commonly nominated reason for GPs to prescribe physical activity in this sample.
Characteristics of scripts written by phase I general practitioners (GPs) (n = 628 scripts)
GP impact
Knowledge and confidence
The response rates to the fax back survey sent to GPs were 33.5% (n = 560; start of phase I) and 45% (n = 299; end of phase II). Respondents were mainly male (66% and 62% respectively). On average they had been in practice for 17 years and saw 121 patients a week. GP knowledge was assessed using four questions to which they responded with agreement or disagreement (table 3). Over the two year period of phase I and phase II, GPs became more knowledgeable about the duration (48% v 70%, p<0.05) and type of activity (47% v 68%, p<0.05) to recommend to their patients. GPs’ confidence in their ability to provide physical activity advice to their patients also increased during this period (69% to 90%, p<0.05).
Results from general fax back survey
Self reported practice
At the end of phase II, participating GPs who responded (n = 299) were aware of physical inactivity as an independent risk factor and the value of providing advice patients. About two thirds of GPs thought that more than half of their patients could benefit from physical activity advice. Most (85%) advised all inactive patients to be more active, particularly those with other risk factors, with 53% stating that they now routinely assessed activity levels of new patients.
A subsample of participating GPs who had received the intervention in phase I (total = 269) were also surveyed to ascertain changes to their practice since 1999. A total of 117 responses (43%) were received, and most GPs (74%) stated that they now advised patients to be active more often as a result of participation in ASP. Many (66%) also reported that they were assessing their patients’ physical activity levels more often, and 43% reported that they were providing advice more systematically. Only 15% were referring patients to outside agencies to support their advice, and 8% reported recalling their patients more often for review. These findings indicate positive behaviour change that has been maintained over the two years of ASP, based on self reports by GPs and summarised in table 3. These results were used to guide the development of the cost effectiveness analysis model.
Patient feedback
Fifty four patients were interviewed by telephone. They were nominated by five GPs who undertook the programme’s clinical audit component. The patient sample consisted of 35 women and 19 men aged 19–91 years. Patient interview findings confirmed the GP findings. Patients perceived the role of GPs in promoting physical activity as appropriate. Patients were aware of the health benefits of physical activity and the amount of activity required to achieve them. They were positive about written scripts; these helped patients remember what to do. Most (52) recalled receiving advice to be more active from their GPs, although a greater proportion recalled receiving verbal (32) rather than written (20) advice. They were more motivated to be active as a result of the advice—most reported a moderate increase in activity levels as assessed by number of minutes of moderate activity—largely by taking up walking.
Economic evaluation
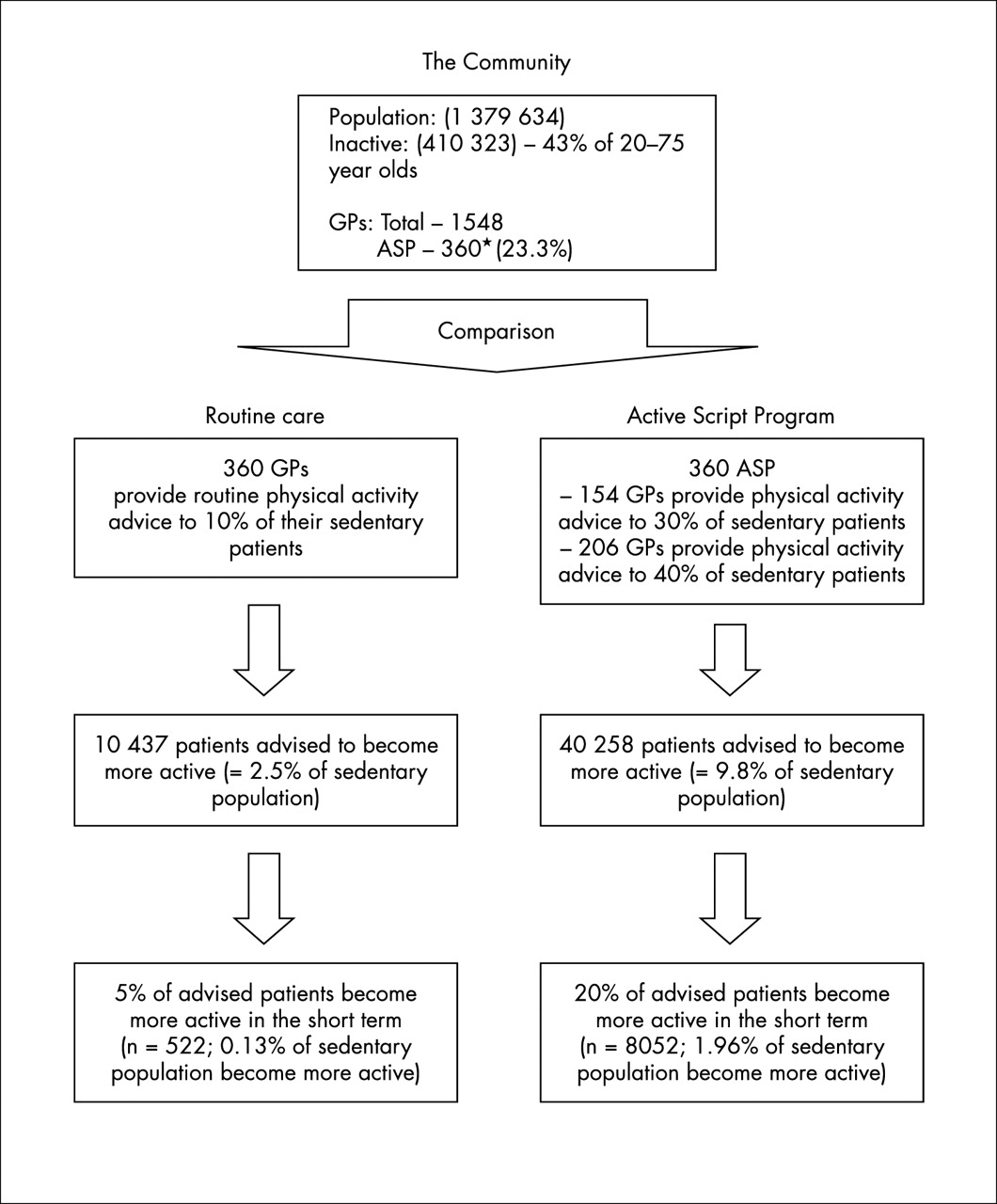
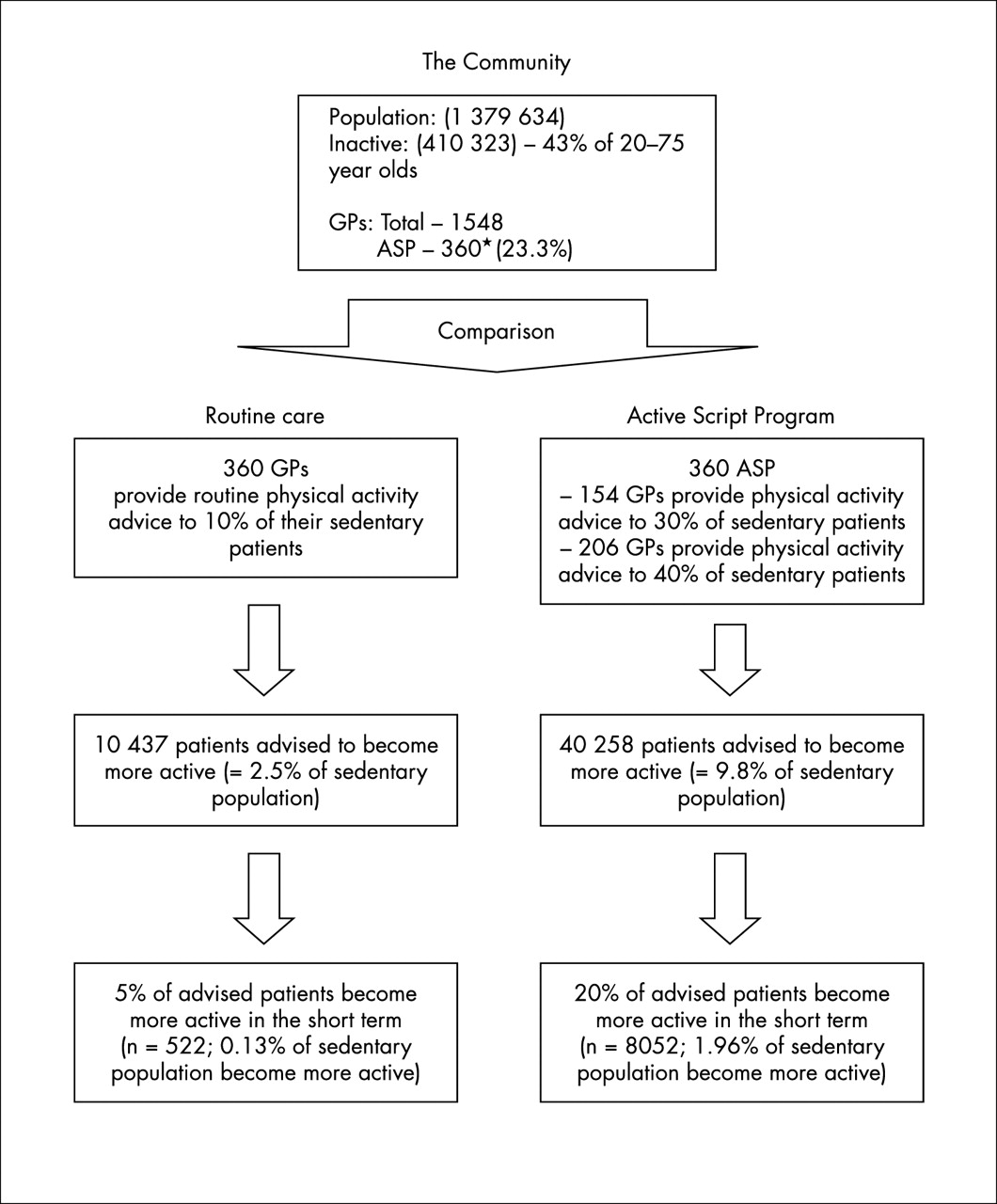
Figure 1 and the box summarise the assumptions made in the economic modelling for evaluation. These assumptions were that 23.3% of GPs (n = 360) would be recruited to the programme for one year within a hypothetical community with a population of 1 379 634 (based on Australian Bureau of Statistics data for all eight participating DGPs in phase I). Of the 360 GPs, 48% (154) would provide “frequent advice” to 30% of their sedentary patients, and 52% (206) would provide “systematic advice” to 40% of their sedentary patients. (The terms relate to the extent to which GPs provide advice to their patients. “Frequent” is defined as GPs advising 30% of their inactive patients. “Systematic” is defined as GPs advising 40% of their inactive patients.) These estimates were derived from the self reported practice of GPs as part of the ASP evaluation. All dollar estimations are for the reference year of 1996 (the most recent available data for burden of disease). The total costs to government were estimated to be $552 845 (made up of $209 254 from ASP, $45 000 as contributions from divisions, and $298 591 as the cost of estimated GP consultations, where the cost of GP consultations is based on an average of four minutes per patient at a cost of $24.50 per consultation with four consultations being conducted in an hour).
{kind=link}
Assumptions of economic modelling of a hypothetical community. *The total number of general practitioners (GPs) trained over the two year period was 670. Two groups of GPs were excluded to establish the number of GPs who were providing advice more frequently or in a systematic way. The first group was the total number of GPs from the two DGPs who did not participate in the second year of the programme. (These GPs from the two DGPs were excluded because of no follow up mechanism to identify their level of involvement.) The second group was the 30% of the GPs from the nine remaining DGPs who indicated no change in their behaviour after the training. A total of 360 (54%) of GPs were included as providing advice more frequently or in a systematic way.28
Based on the specified assumptions, the health savings for six relevant diseases that would result from a 1% reduction in number of sedentary people was estimated to be $564 199 (discounted). The health benefits were 155 DALYs (discounted). The programme would prevent 12 premature deaths. The cost effectiveness ratios for the ASP were: $69 per patient to become more active in the short term; $138 per patient to accrue a health benefit; $3647 per DALY saved; $48 924 per premature death averted. Cost effectiveness results below $30 000 per DALY saved would generally be regarded as favourable in Australia, and cost effectiveness results below $10 000 per DALY saved would be regarded as excellent value for money compared with how resources are currently being deployed in the healthcare sector.
To achieve the results identified above, the average GP needed to advise 2.5 patients a week to become more active. The economic modelling indicated that, for 112 patients advised per GP, 22 patients would increase their activity level in the short term (20%), and half of these (11 patients or 10%) would maintain their activity level to accrue a health benefit over time. This estimate was based on an analysis of potential for benefit of brief counselling conducted by Bull in 1999.24 Its impact was also addressed through the sensitivity analysis, which varied this to 5% or 2.5%, and still showed a positive economic effect. The annual average opportunity cost to the GP in spending an additional four minutes (non-reimbursed time, fewer patients seen, or longer hours worked) advising patients was $829 (frequent GPs $644 and systematic GPs $967).
The sensitivity analysis compared the net costs and benefits of routine care with that of the ASP. Based on GP reach, the results showed that even with a reduction of GP involvement from 23.3% (current model) to only 5%, the cost would be $3921 per DALY saved, and 865 patients would accrue a health benefit over time as a result of achieving a 1 percentage point reduction in the sedentary population. Similarly, using the percentage of patients becoming more active in the short term as a result of GP advice, if this was decreased from 20% (current model) to only 5%, the programme cost per DALY would be $9248. If the percentage of these patients who maintained their activity levels over time to accrue health benefits were varied from 50% (current model), the programme could still be considered cost effective at 10% maintenance ($12 778 per DALY) but probably not at 2.5% ($63 754 per DALY).
DISCUSSION
Efficacy
The findings show that the programme affords a net health gain. The ASP can be viewed as a valuable programme, particularly compared with the costs of other lifestyle modification programmes.6,25,26 In economic terms, it would be referred to as a “dominant” programme—that is, one where the total costs to government are less than the cost offsets (health savings). The assumptions for the economic analyses conducted drew not only on the evidence base, but also on the experiences of actual implementation of the ASP in Victoria. Based on the ASP experience to date, together with the assumptions used in the modelling, the economic appraisal suggests that the programme has the potential to be highly cost effective. The five key contributory features are:
-
The high prevalence of physical inactivity as a modifiable risk factor in the population
-
Strong epidemiological evidence that associates a number of important diseases with inactivity.
-
Good evidence indicating GP effectiveness to promote patient change in the short term.
-
The potential reach of GPs to a high proportion of the exposed population.
-
The use of divisions to engage and influence GPs.
Our use of the RE-AIM framework in its totality to evaluate the programme was limited by the primary focus of ASP being on effectiveness rather than efficacy. Nevertheless, the findings support the programme’s cost effectiveness. This exploratory study of GPs systematically advising patients to be physically active offers a strong economic argument for government investment in such programmes. The ASP exemplifies how State government funding can enhance and refine the focus of Commonwealth government dollars spent in general practice for the benefit of the state’s community.
Reach
The ASP recruited a fifth of the GPs across the participating divisions. Thus, for the reach component of the RE-AIM model,11 the ASP has been modestly successful in targeting DGPs and their GPs. Community reach was less successful. The development of effective community linkages is a system-wide issue in primary care. In Victoria, the state government’s Primary Care Partnership (PCP) initiative, which aims to link primary care agencies to enable integrated healthcare management, is addressing this. Schemes such as ASP stand to benefit from the divisions’ involvement in the PCP’s GP engagement strategy. Further work is required to assess patient reach.
Take home message
GPs clearly have a role in providing brief advice on physical activity promotion. The Active Script Programme increased the capacity for DGPs to support GPs in promoting physical activity. The economic appraisal suggests that the programme has the potential to be highly cost effective. However, maintenance of activity levels is more complex and will require an integrated multisectorial approach beyond general practice.
Adoption, implementation, and maintenance
The programme has been adopted across general practice in representative settings. The programme’s capacity building framework, incorporating centralised management and support combined with a local delivery model, enabled a reasonable level of adoption and implementation at the divisional and practitioner level. The programme led to self reported improvements in knowledge and frequency of advice provision, but was less successful in getting GPs to implement the ASP as intended. GPs’ knowledge of the benefits of physical activity promotion increased significantly from the programme’s outset (phase I). GPs generally agreed that they had a role in patient assessment and provision of physical activity advice. Most thought that ASP had afforded them skills to provide effective advice on physical activity. Improved competence was reflected in the regularity of GPs using ASP resources, promoting physical activity, and incorporating advice routinely into their practice. The generalisability of the findings is limited by the low response rate. Corroborating evidence was obtained from the patient interviews, albeit it was a small sampling frame. Many patients confirmed that they had received verbal advice on physical activity from their GP, in some instances supported by receipt of a written assessment of physical activity level.
At the consultation level, lessons have been learnt that will assist future fulfilment of the implementation and maintenance criteria. There were no short cuts to GP engagement. In line with the literature,27 divisions found that one-off continuing medical education events and practice visits were insufficient to maintain GPs’ use of ASP resources and physical activity promotion; follow up reminders were required.
There is some evidence that programme maintenance is occurring at divisional level, with ASP principles beginning to be incorporated into divisional programmes and business plans. Some caution is warranted with regard to the maintenance of patients’ activity levels. Trials in the available evidence base provide limited evidence for long term health gain.25 GPs clearly have a role in providing brief advice and can achieve high patient reach. Ensuring that patients maintain their activity levels is more complex and will require an integrated multisectoral approach to facilitate patient adherence. Indeed, multifaceted strategies at policy, structural, funding, and systems levels to involve GPs and other allied health professionals are indicated. Encouraging GP referrals to established community organisations that promote continuing physical activity seems prudent.
The ASP was implemented as a service delivery model, thus the associated data collection was not as detailed as that required by a research intervention. Nevertheless, the model has benefited from being tested “in the field”, enhancing the generalisability and reproducibility of its findings within general practice. The programme’s scope is likely to be extended after the recent introduction of an electronic form of the script, available in the major GP software packages. This could serve as a platform for further research, in particular to assess the extent of the programme’s impact on patient behaviour and health status. We endorse the recent call from the US Preventive Services Task Force for further studies of the effects of such clinician interventions on physical activity levels in all sectors of the community.28
We conclude that the ASP acted as a catalyst for DGPs to support GPs to promote physical activity. The ASP delivered a popular programme to DGPs and GPs which built the capacity of DGPs to support GPs to promote physical activity to their patients, and increased awareness among GPs to assess and provide physical activity advice. The cost effectiveness results of the ASP indicate that divisional funding support could usefully be supplemented by funding to assist in the maintenance of patients activity levels in the community.
Acknowledgments
We acknowledge the support of the Victorian Department of Human Services in funding the Active Script Programme. We express our thanks to all the participating DGPs and their GP members for their involvement in the programme.
REFERENCES
Supplementary materials
Publisher Correction
Please note that the author list order is incorrect. The author list is shown here:
Huang N, Pietsch J, Naccarella L, Sims J
The error is much regretted.
Linked Articles
- Correction