Article Text

Abstract
Background: The development of symptomatic hyponatraemia consequent on participation in marathon and ultraendurance races has led to questions about its aetiology and prevention.
Objectives: To evaluate: (a) the assertion that sweat sodium losses cannot contribute to the development of hyponatraemia during endurance exercise; (b) the adequacy of fluid replacement recommendations issued by the International Marathon Medical Directors Association (IMMDA) for races of 42 km or longer; (c) the effectiveness of commercial sports drinks, compared with water, for attenuating plasma sodium reductions.
Methods: A mathematical model was used to predict the effects of different drinking behaviours on hydration status and plasma sodium concentration when body mass, body composition, running speed, weather conditions, and sweat sodium concentration were systematically varied.
Results: Fluid intake at rates that exceed sweating rate is predicted to be the primary cause of hyponatraemia. However, the model predicts that runners secreting relatively salty sweat can finish ultraendurance exercise both dehydrated and hyponatraemic. Electrolyte-containing beverages are predicted to delay the development of hyponatraemia. The predictions suggest that the IMMDA fluid intake recommendations adequately sustain hydration over the 42 km distance if qualifiers—for example, running pace, body size—are followed.
Conclusions: Actions to prevent hyponatraemia should focus on minimising overdrinking relative to sweating rate and attenuating salt depletion in those who excrete salty sweat. This simulation demonstrates the complexity of defining fluid and electrolyte consumption rates during athletic competition.
- water intoxication
- fluid balance
- dehydration
- overhydration
- prolonged exercise
Statistics from Altmetric.com
Symptomatic hyponatraemia associated with athletic competition was first described in 1985,1 and more than 100 cases have been documented.2–4 Although most cases develop during participation in endurance events lasting eight hours or more, this syndrome also develops in slower runners participating in marathon (42 km) races. Most cases are associated with excessive fluid intake and weight gain.2,5 However, there is evidence that some athletes finish ultraendurance competition with plasma sodium concentrations below 130 mEq/l and have body mass losses greater than or equal to the weight loss expected from cellular respiration and respiratory water loss.6,7 The latter suggests that, in certain situations, hyponatraemia can occur without excessive fluid consumption. As sweat sodium concentrations can be high,8,9 it has been proposed that excessive fluid consumption and sweat sodium losses can contribute to symptomatic hyponatraemia.5 Noakes and colleagues have discounted the idea that sweat sodium losses contribute to the development of symptomatic hyponatraemia10,11 and argue that all cases would be prevented if athletes refrained from drinking excessively large volumes during endurance events.10,11
In response to the symptomatic hyponatraemia cases during marathon competitions, the International Marathon Medical Directors Association (IMMDA) of the Association of International Marathons published a position stand recommending that marathon runners drink ad libitum 400–800 ml/h, with the higher rates for the faster, heavier runners competing in warm environmental conditions and the lower rates for the slower runners/walkers completing marathon races in cooler environmental conditions.12 IMMDA has not made any recommendations about sodium intake. The adequacy of the IMMDA recommendation for preventing excessive dehydration or the development of symptomatic hyponatraemia has not been systematically evaluated. Excessive dehydration was not defined and probably refers more to minimising its contributions to heat exhaustion rather than to sustaining race pace. The IMMDA fluid consumption rates were stated as being “applicable to other distance running races”, so perhaps including ultraendurance events, such as Ironman distance triathlons. The effect of using the IMMDA recommendation for races longer than a marathon has also not been systematically evaluated.
This study uses a mathematical model to simulate the effects of different drinking behaviours on hydration status and plasma sodium concentration when body mass, body composition, running speed, weather conditions, and sweat sodium concentration are systematically varied. This mathematical analysis evaluates: (a) the assertion that unreplaced sweat sodium cannot contribute to the development of hyponatraemia during endurance exercise; (b) the applicability of IMMDA fluid replacement recommendations for running events longer than or equal to 42 km; (c) the effectiveness of commercial sports drinks, compared with water, for attenuating plasma sodium reductions. For the analyses, a fluid intake rate was considered effective for sustaining performance if predicted loss of body mass (attributable to dehydration) did not exceed 3% of the initial body mass and/or predicted plasma sodium concentrations did not fall below 130 mEq/l by the end of the estimated race time. A priori, we hypothesised that, under most circumstances, hyponatraemia would be primarily attributable to excessive fluid intake (relative to sweating rate), that high sweat sodium concentration would minimise the amount of overdrinking needed to produce sodium dilution, and the combination of hydration and unreplaced sweat sodium losses could, under specific circumstances, produce both dehydration and hyponatraemia. This simulation demonstrates the complexity of defining fluid and electrolyte consumption needs during athletic competition.
METHODS
Body water and sodium loss (gain) were modelled for subjects of various body masses (50, 70 and 90 kg) and body compositions (total body water equal to 63% and 50% of body mass),13 performing prolonged sustained exercise equivalent to the energy cost of running 8.5, 10, 12.5, and 15 km/h in cool/temperate (∼ 18°C) and warm (∼ 28°C) weather, with various water consumption rates (400, 600 and 800 ml/h) and sweat sodium concentrations (25, 50 and 75 mEq/l).
Changes in body mass (due to water loss/gain) and plasma sodium concentration were calculated from the following equations:
SR = (BM × V)/732 × (1 − ((R + C)/H))
FB = FI − SR × t
%BML = FB/BMi × 100
ΔNa+e = (FI × Na+FI × t) − (SR × Na+sweat × t)
ΔK+e = (FI × K+FI × t) − (SR × K+sweat × t)
[Na+]p2 = ((([Na+]p1 + 23.8) × TBWi + 1.03Δ(Na+e + K+e))/(TBWi + FB)) − 23.8
where SR is sweating rate (litres/h), BM is body mass (kg), V is velocity (km/h), R + C is radiative and convective heat loss (W/m2), H is heat production (W/m2), FB is fluid balance (litres), FI is fluid intake (litres/h), t is time (hours), %BML is percentage body mass loss, BMi is initial body mass (kg), ΔNa+e is the change in exchangeable sodium (mEq), Na+FI is the sodium concentration of the fluids consumed (mEq/l), Na+sweat is the sweat sodium concentration (mEq/l), ΔK+e is the change in exchangeable potassium (mEq), K+FI is the potassium concentration of the fluids consumed (mEq/l), K+sweat is the sweat potassium concentration (mEq/l),[Na+]p2 is the predicted plasma sodium concentration (mEq/l), [Na+]p1 is the initial plasma sodium concentration (mEq/l), and TBWi is initial total body water (litres).
Sweating rate was calculated from energy cost of locomotion and expected heat production14 with adjustment for heat loss from radiation and convection.15 For the latter, it was assumed that the skin to ambient temperature gradient was 10°C and 4°C for cool/temperate and warm weather conditions respectively. The sweating rate equation assumes that sweating and sweat evaporation are 100% efficient. Plasma sodium concentration was calculated using the equation of Kurtz and Nguyen,16 which predicts changes in plasma sodium concentration from changes in the mass balance of sodium, potassium, and water. Details on the derivation of the equation and the significance of the constants are presented elsewhere,16,17 but they account for the unequal distribution of univalent cations between the plasma and interstitial fluid, the osmotic coefficient of sodium salts, the contribution of osmotically inactive exchangeable sodium and potassium, plasma potassium concentration, and osmotically active non-sodium and non-potassium osmoles. For this analysis, initial plasma sodium concentration was assumed to be 140 mEq/l. Potassium losses in sweat were assumed to be 4.5 mEq/l.9,18 For simplicity, BMLs due to respiratory water loss and oxidative metabolism were ignored. This omission should have limited effect on body water status, as the rate of respiratory water loss is typically negated by the water produced during cellular respiration. However, it will produce less BML than what would be expected to occur. Similarly, no attempt was made to adjust water gained from the breakdown of muscle glycogen or protein. However, the model also assumed that there was no change in the quantity of osmotic particles in the intracellular fluid and no water or electrolytes were lost in urine. On the basis of reported urine production rates during Ironman triathlons19 and estimated water released from glycogen oxidation, these omissions probably underestimated fluid balance by 50–300 ml over such a triathlon.
Data were analysed by evaluating the changes in body mass and sodium concentration over time. The rate of fluid intake was considered effective for sustaining performance if dehydration did not produce a BML in excess of 3% initial body mass and/or plasma sodium concentrations did not fall below 130 mEq/l by the end of the estimated race time. These values were chosen because dehydration in excess of 2% body mass is associated with the onset of impaired endurance performance,13,20 and plasma sodium concentrations below 130 mEq/l are associated with the development of symptomatic hyponatraemia.5 For this paper, hyponatraemia is defined as plasma sodium <130 mEq/l.
RESULTS
Table 1 presents the predicted sweating rates for 50–90 kg subjects running at 8.5–15 km/h in cool/temperate and warm weather conditions. Figure 1 presents the predicted BML (attributable to water deficit) and predicted plasma sodium associated with three rates of fluid replacement for a 70 kg person, running at a velocity approximating the average time of mass participant marathons. During cool/temperate weather (upper panels), 400 ml/h water or electrolyte-free fluid is predicted to produce ∼2% BML by the end of a 42 km marathon and ∼6% BML by the end of an Ironman length triathlon. Consumption of 400 ml/h water is not predicted to produce hyponatraemia over the range of sweat sodium concentrations evaluated. Drinking at 600 ml/h would lead to moderate dehydration (2–5% BML) over time. Interestingly, despite modest dehydration, when sweat sodium is 75 mEq/l, drinking at this rate would be sufficient to induce hyponatraemia by the end of an Ironman length competition. Drinking water at a rate of 800 ml/h is predicted to prevent dehydration, but hyponatraemia would occur after five to six and eight to nine hours when sweat sodium concentrations are 75 and 50 mEq/l respectively. In the warm environment, 800 ml/h water consumption is also predicted to produce a modest dehydration (1–2% BML) and hyponatraemia during an Ironman length competition when sweat sodium concentrations are 50 mEq/l and higher.
Predicted sweating rates (litres/h) for running 8.5–15 km/h in cool/temperate (18°C) and warm (28°C) weather
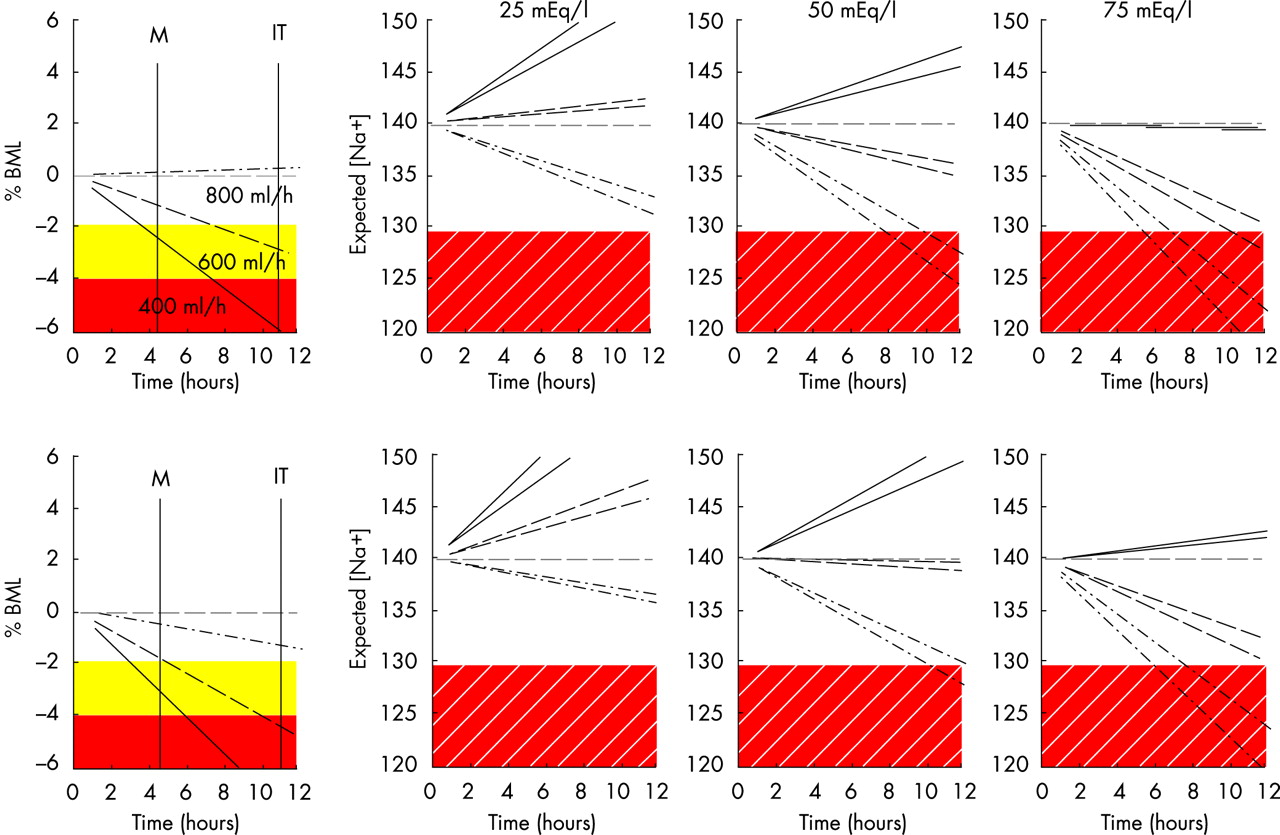
Predicted percentage body mass loss due to water deficit (%BML) and plasma sodium concentration (mEq/l) under three levels of sweat sodium loss for 70 kg subjects of varying body composition drinking 400–800 ml water/hour while running at 10 km/h in cool (18°C; upper panels) and warm (28°C; lower panels) weather. The solid shaded areas demark when water loss would be sufficient to modestly (yellow) and substantially (red) diminish performance. The hatched shaded area demarks the presence of hyponatraemia. The two lines sharing the same line style in the sodium figures are the predicted outcomes for each fluid replacement rate (400 ml/h = solid line, 600 ml/h = dashed line, 800 ml/h = dash-dot line) when total body water accounts for 50% and 63% of body mass. M indicates the finishing time for the marathon run. IT indicates the approximate finishing time for the Ironman distance triathlon based on literature values for participants running a marathon portion at 10 km/h.
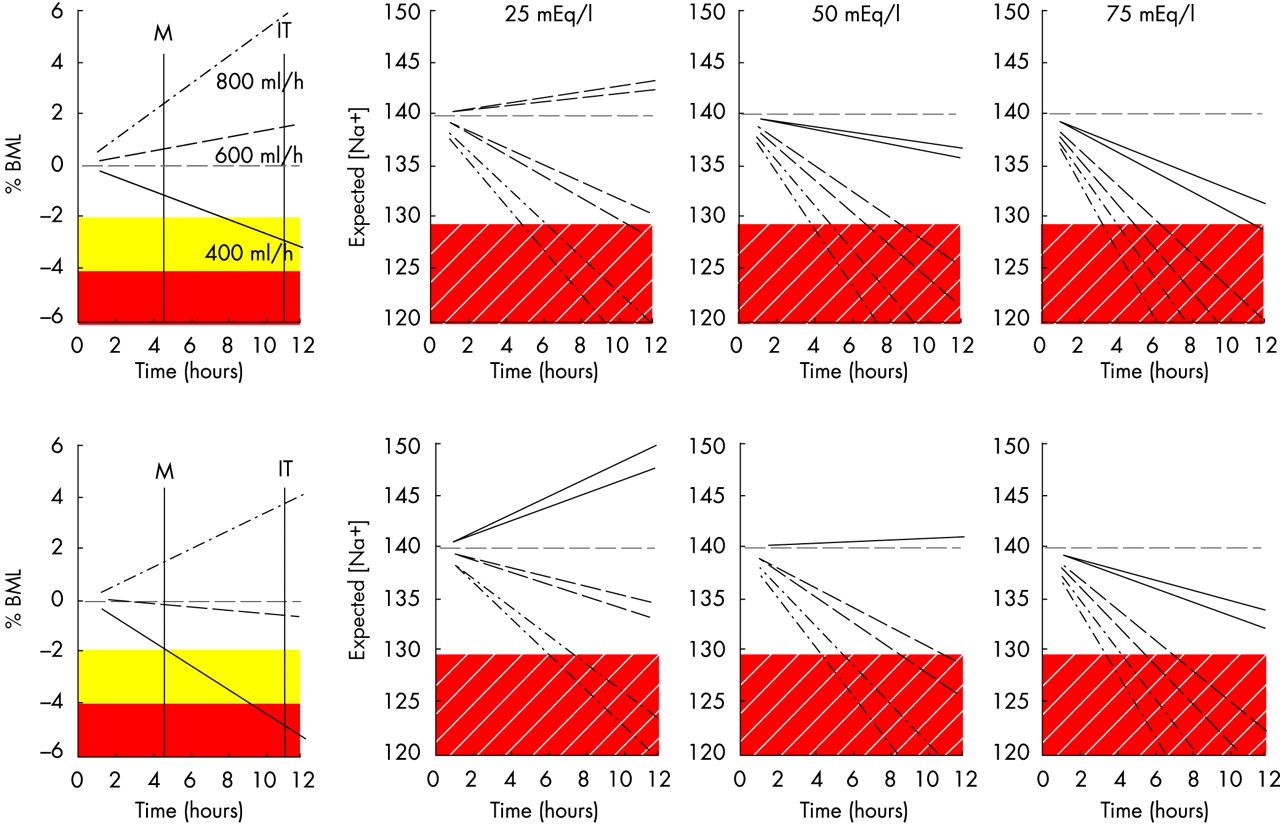
Figure 2 presents the predicted outcomes for the smaller 50 kg person running at 10 km/h. In cool/temperate weather, 400 ml/h consumption of water would sustain adequate hydration and prevent hyponatraemia, whereas 600–800 ml/h water is predicted to be in excess of sweat loss and would dilute plasma sodium over time. Consuming 800 ml/h would produce hyponatraemia before the finish of a 42 km marathon if sweat sodium concentration is 50 mEq/l and higher. In warm weather, 400 ml/h consumption of water is predicted to produce 2% BML and 5% BML by the end of a 42 km marathon and Ironman length triathlon respectively. Consuming 600 ml/h water is predicted to sustain hydration through an Ironman length triathlon, but induce hyponatraemia before the end if sweat sodium concentrations are 50 mEq/l or higher. Drinking 800 ml/h would be in excess of sweating rate and produce hyponatraemia by the end of a marathon if sweat sodium is 75 mEq/l.

Predicted percentage body mass loss due to water deficit (%BML) and plasma sodium concentration (mEq/l) under three levels of sweat sodium loss for 50 kg subjects of varying body composition drinking 400–800 ml water/hour while running at 10 km/h in cool (18°C; upper panels) and warm (28°C; lower panels) weather. The solid shaded areas demark when water loss would be sufficient to modestly (yellow) and substantially (red) diminish performance. The hatched shaded area demarks the presence of hyponatraemia. The two lines sharing the same line style in the sodium figures are the predicted outcomes for each fluid replacement rate (400 ml/h = solid line, 600 ml/h = dashed line, 800 ml/h = dash-dot line) when total body water accounts for 50% and 63% of body mass. M indicates the finishing time for the marathon run. IT indicates the approximate finishing time for the Ironman distance triathlon based on literature values for participants running a marathon portion at 10 km/h.
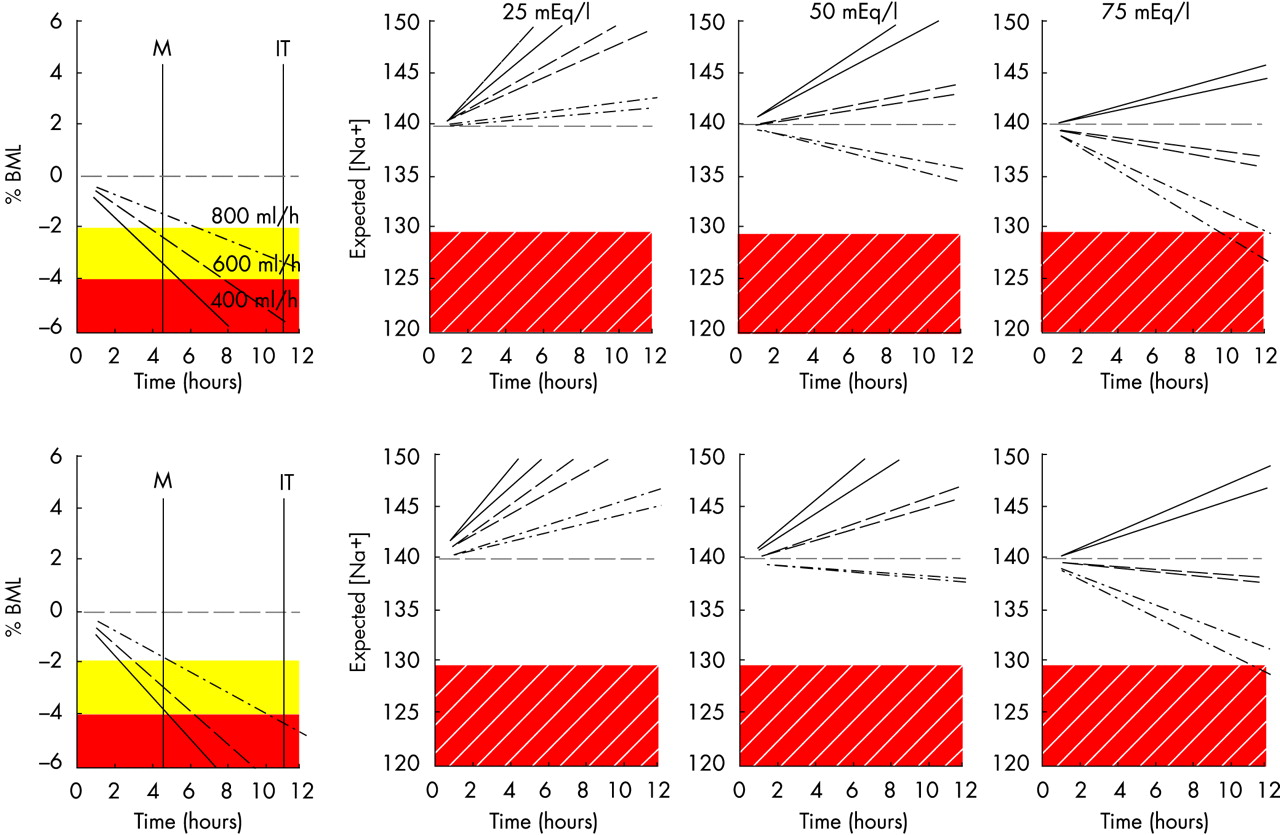
Figure 3 presents the predicted outcomes for a larger 90 kg person running at 10 km/h. Progressive dehydration is predicted over the range of fluid intakes examined. Hyponatraemia was produced only when 800 ml/h was consumed with 75 mEq/l sweat sodium concentration.

Predicted percentage body mass loss due to water deficit (%BML) and plasma sodium concentration (mEq/l) under three levels of sweat sodium loss for 90 kg subjects of varying body composition drinking 400–800 ml water/hour while running at 10 km/h in cool (18°C; upper panels) and warm (28°C; lower panels) weather. The solid shaded areas demark when water loss would be sufficient to modestly (yellow) and substantially (red) diminish performance. The hatched shaded area demarks the presence of hyponatraemia. The two lines sharing the same line style in the sodium figures are the predicted outcomes for each fluid replacement rate (400 ml/h = solid line, 600 ml/h = dashed line, 800 ml/h = dash-dot line) when total body water accounts for 50% and 63% of body mass. M indicates the finishing time for the marathon run. IT indicates the approximate finishing time for the Ironman distance triathlon based on literature values for participants running a marathon portion at 10 km/h.
Slower (8.5 km/h) marathon runners have been reported to be at higher risk of developing exercise associated hyponatraemia.4,21 When this pace was used in the simulation, a 70 kg person consuming 400–600 ml/h water was not predicted to develop hyponatraemia, except if consuming 600 ml/h and sweat sodium was 75 mEq/l. Hyponatraemia would occur after eight to nine hours and 9–11 hours in cool and warm weather respectively. In cool/temperate weather, drinking 800 ml/h would produce overhydration and development of hyponatraemia after six to seven hours and 8.5–10 hours when sweat sodium was 50 and 25 mEq/l respectively. In warm weather, this drinking rate would produce less overhydration, and hyponatraemia would not develop until seven to nine hours at 50 mEq/l sweat sodium. For a 50 kg person, the slower speed would produce a similar pattern of changes, with 800 ml/h inducing dilutional hyponatraemia within a 42 km marathon independent of sweat sodium concentration. Drinking 400 ml/h would sustain adequate hydration and prevent hyponatraemia over an Ironman length triathlon when sweat sodium is 50 mEq/l or less.
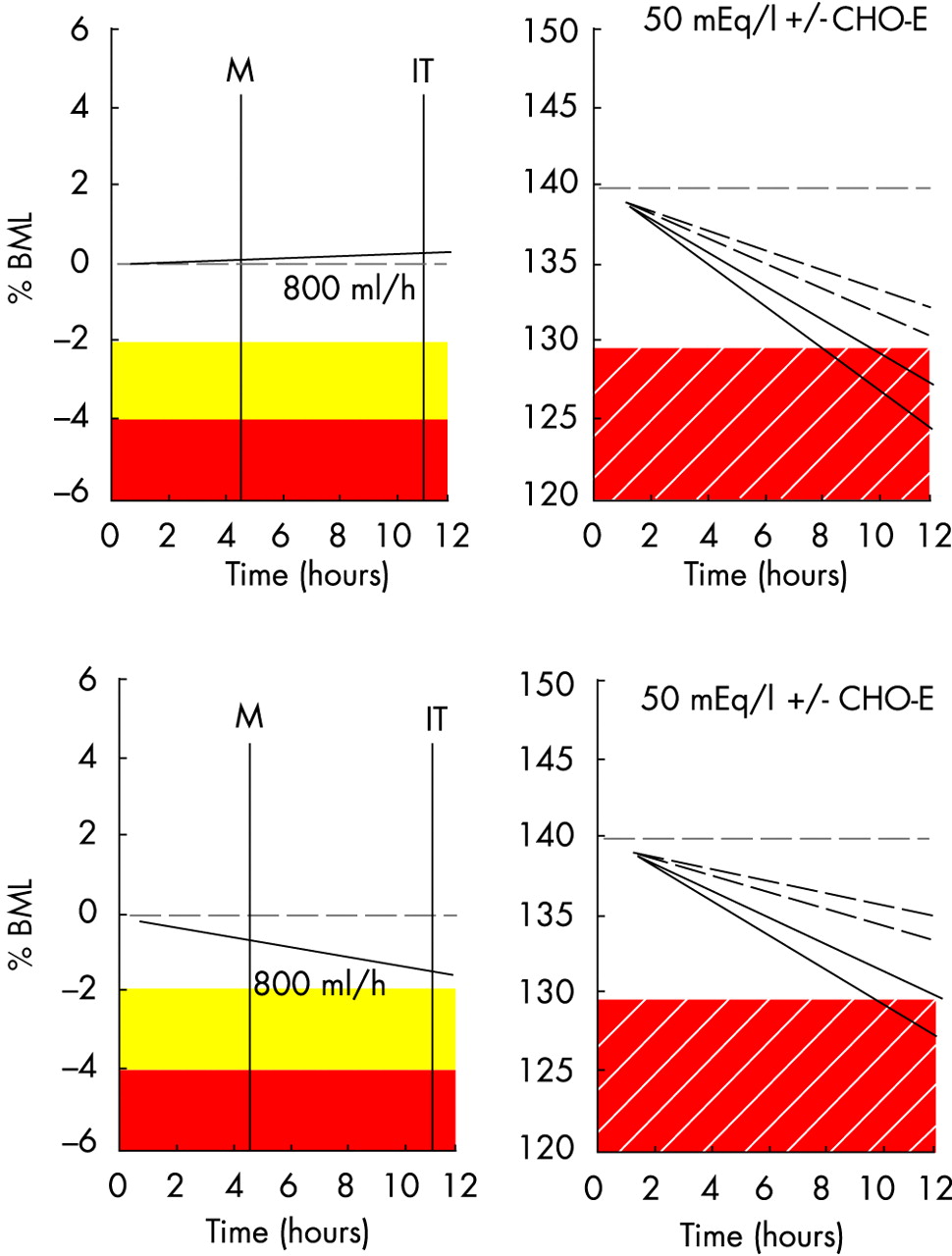
Figure 4 illustrates the influence of consuming a sports drink (containing 20 mEq/l sodium and 3 mEq potassium) in delaying hyponatraemia. In both cool/temperate and warm condition simulations, the sports drink is predicted to slow the rate of plasma sodium reduction (0.44 and 0.55 mEq/l/h when total body water is 63% and 50% of body mass respectively). Therefore, in these situations, sports drink consumption would prevent hyponatraemia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Predicted effectiveness of a carbohydrate-electrolyte sports drink (CHO-E) containing 17 mEq/l sodium and 5 mEq/l potassium for attenuating the decline in plasma sodium concentration (mEq/l) expected for a 70 kg person drinking water at 800 ml/h when running 10 km/h in cool (18°C; upper panel) and warm (28°C; lower panel) weather. The solid shaded areas demark when water loss would be sufficient to modestly (yellow) and (red) substantially diminish performance. The hatched shaded area demarks the presence of hyponatraemia. M indicates the finishing time for the marathon run. IT indicates the approximate finishing time for the Ironman distance triathlon based on literature values for participants running a marathon portion at 10 km/h. For the sodium figures, the solid lines reflect the effect of drinking water only, and hatched lines illustrate the effect of consuming the same volume of a sports drink. The pair of lines of similar type represent the predicted outcomes when total body water accounts for 50% and 63% of body mass. BML, Body mass loss.
The effectiveness of drinking at 400–800 ml/h to sustain hydration over a 42 km run depends on body mass, race speed, and weather. Table 2 provides the predicted BML changes attributable to dehydration in cool/temperate weather. As illustrated in table 2, a 50 kg person consuming 400 ml/h fluid would sustain hydration across the running speeds examined. Consuming 600 ml/h would be predicted to induce overhydration at running speeds below 10 km/h, as would consuming 800 ml/h at 12.5 km/h. Consuming 400–600 ml/h would sustain hydration of a 70 kg runner, except that 400 ml/h at 15 km/h is predicted to produce excessive dehydration. At the other extreme, 800 ml/h is predicted to induce overhydration at running speeds below 10 km/h. For a 90 kg person, consuming 400–800 ml/h would adequately sustain hydration at running speeds of 8.5–10 km/h. At a 12.5 km/h and higher pace, consuming 400 ml/h would be insufficient to prevent excessive dehydration (⩾3% BML), and 800 ml/h would sustain adequate hydration.
Predicted percentage body mass loss due to dehydration at end of 42 km marathon held in cool/temperate (18°C) weather for runners of various body mass drinking 400–800 ml/h while running at 8.5–15 km/h
Table 3 provides the predicted body mass changes attributable to dehydration for a warm weather 42 km marathon. Consuming 400 ml/h would be adequate to sustain hydration for a 50 kg person except at the ∼15 km/h pace, at which dehydration is predicted to reach 3.2% BML. Drinking at a rate of 600 ml/h or higher while running at 8.5 km/h or drinking at a rate of 800 ml/h at 10 km/h would produce overhydration. For a 70 kg runner, a 10 km/h pace and consumption at 400 ml/h would result in dehydration, with 2.9% BML before completion of the race. Drinking 800 ml/h is predicted to induce modest overhydration at 8.5 km/h, otherwise consuming 600–800 ml/h seems appropriate to sustain hydration. For a 90 kg person, 400 ml/h would produce dehydration in excess of 3% BML at all running speeds, and 600 ml/h would be adequate until running pace reached ∼12.5 km/h, and thereafter consumption of 800 ml/h would be needed to sustain hydration.
Predicted percentage body mass loss due to dehydration at the end of a 42 km marathon held in warm (28°C) weather for runners of various body mass drinking 400–800 ml/h while running at 8.5–15 km/h
DISCUSSION
This paper provides a quantitative approach to assessing the contribution of fluid intake and sweat sodium losses to the plasma sodium dilution during prolonged exercise. We were interested in evaluating whether hyponatraemia could occur without overdrinking relative to sweating rate. The sweat sodium concentrations used for the simulation represent the average and range observed in laboratory and field studies.9,18,22 The fluid intake rates were selected to cover the range recently recommended for curtailing overdrinking during marathon running.12
Central to acceptance of the outcomes of these simulations is the validity of the assumptions used in producing the model. Specifically, it was assumed that sweat rates and sweat electrolyte composition would remain constant over time. We further assumed that running velocity would remain constant for the duration of the modelled scenario. It is likely that running pace and sweat rate and composition would vary during a race. The body water estimates represent the average values for men and women, covering a broad range of expected values. The sweating rate estimate used an accepted estimate of energy expenditure. We minimised the likelihood of overpredicting sweating rate by adjusting for the increasing convective heat transfer as running speed increases. Plasma sodium concentrations were predicted using a validated equation. Most importantly, the model produced sweating rate estimates similar to those measured in marathon participants running at 10–15 km/h23–25 and accurately modelled plasma sodium changes measured consequent on prolonged exercise under different rates of fluid replacement and when fluids of various compositions were consumed.26–29 That said, it is known that sweat rates and composition will vary considerably between individuals, so the predictions are only a “reasonable” average response, and actual sweating rates and plasma sodium estimates are probably normally distributed around the predicted values.13
The simulations predict that overdrinking is the cause of exertional hyponatraemia during ∼42 km marathon events. Across the scenarios evaluated for marathon distances, the magnitude of sweat sodium loss was insufficient to produce enough reduction in plasma sodium for symptomatic hyponatraemia without overdrinking relative to sweating rate. This agrees with the observations that hyponatraemic marathon runners have greater self reported fluid intakes than expected sweating rates.3,4,21
For longer duration events, such as Ironman triathlon, overdrinking relative to sweating rate is the major cause of symptomatic hyponatraemia.2 However, the simulation predicts that it is not a prerequisite condition for hyponatraemia. As illustrated in figs 1–3, when sweat sodium concentrations are above average, but within the normal range, a sufficient sweat sodium deficit can accrue for ultraendurance athletes to finish both dehydrated and hyponatraemic. This is supported by the finding that some triathletes with >2% BML during a triathlon competition have plasma sodium concentrations after the race of 130 mEq/l or below.6,7 Whether the magnitude of hyponatraemia is sufficient to produce symptoms, however, is uncertain, as in most cases of symptomatic hyponatraemia plasma sodium concentrations are less than 125 mEq/l.2,5 In our simulations, this level of hyponatraemia was only reached when sweat sodium was well above average.8,13,18
The risk of developing symptomatic hyponatraemia depends on both the magnitude of sodium dilution and the rate at which the water/electrolyte imbalance occurs.30 As figs 1–3 illustrate, salty sweat reduces the amount of overdrinking necessary to produce hyponatraemia and accelerates the reduction in plasma sodium. In the situations where both dehydration and hyponatraemia are present, aggressive rehydration during recovery from the race with water or electrolyte-poor drinks could produce rapid dilution of plasma sodium to concentrations associated with symptomatic hyponatraemia. This scenario may explain why many runners with hyponatraemia present with symptoms several hours after completing a race.3
The use of sports drinks instead of water or electrolyte-free drinks is one strategy for slowing down the development of hyponatraemia. This approach is recommended by the American College of Sports Medicine for ultraendurance races31 and the Institute of Medicine for prolonged physical labour in hot environments.32 As illustrated in fig 4, under conditions in which sweat sodium concentrations are high, fluid replacement with electrolyte sports drink slows down the dilution of plasma sodium, and reduces the likelihood of hyponatraemia development. In the cool/temperate weather conditions, consuming sports drink instead of water delayed the development of hyponatraemia for four to five hours. Thus there is merit in consuming electrolyte-containing drinks or food during ultraendurance competition, and this should be considered as part of a preventive strategy, particularly if there is a suspicion that the athlete secretes relatively salty sweat.
Electrolyte replacement should be considered only as part of the preventive process; most important is the avoidance of excessive fluid intake. Electrolyte replacement will slow but not prevent the development of hyponatraemia if fluid intake is in gross excess of sweating rate. There is no physiological advantage of drinking above sweating rate.33 Furthermore, as dehydration levels to ∼2% of body mass do not adversely affect exercise performance,13,20 there is a range of dehydration that is acceptable during competition. In addition, the magnitude of water deficit before performance deteriorates probably has individual and event/environment variability. For our simulation, we used 3% BML as the threshold of drinking too little during exercise and replacement above sweating rate as too much. We chose 3% BML because enough time would have accrued since attainment of 2% BML for performance time to be significantly compromised. We then evaluated the efficacy of the IMMDA position stand for sustaining hydration during marathon and longer ultradistance events.
As illustrated in tables 2 and 3, within the boundaries of consuming 400–800 ml/h fluid, there was a rehydration rate that was appropriate for sustaining hydration. Within that fluid intake range, the optimal rate depended on body mass, race pace, and weather. Whereas drinking 600 ml/h was appropriate for a 70–90 kg person in the cool/temperate weather simulation, the same rate of fluid replacement would produce overhydration in a 50 kg person running at pace of 10 km/h or slower. Furthermore, this rate of fluid intake, for a 50 kg person running at a 10 km/h pace with sweat sodium of 50 mEq/l, is predicted to lower plasma sodium concentrations to 123–126 mEq/l by the end of the race. In contrast, a 90 kg person would have developed excessive dehydration. Thus, if athletes implement the range of fluid intakes and qualifiers provided in the IMMDA guidelines, the simulation predicts that excessive dehydration and hyponatraemia would be prevented in a 42 km marathon. However, like the fluid replacement recommendations of other professional organisations,31,34 the IMMDA recommendations need to be sensibly implemented, as arbitrary use of the fluid intake range provided without consideration of the parameters that influence sweating rate will lead to excessive dehydration in some athletes and overhydration in others. Athletes should be encouraged to evaluate their individual fluid losses during practice sessions and develop personal rehydration programmes.
It is important to recognise that the body mass changes predicted by the model reflect only those attributable to changes in total body water. Oxidation of carbohydrate, fat, and protein leads to a loss of mass independent of total body water. Similarly, ventilation leads to respiratory water loss and BML. However, the respiratory water loss typically does not affect total body water, as approximately the same amount of water is produced during cell respiration. These weight losses can be estimated: 0.12 g/kcal and 0.11 g/kcal respectively.24 For a 70 kg participant in a 42 km marathon, they could produce 1% BML without affecting fluid balance.
In summary, fluid intake in excess of sweating rate is the primary cause of hyponatraemia associated with prolonged exercise. Thus preventive strategies to limit overhydration are warranted. The contribution of sweat sodium losses, however, should not be ignored. People who secrete relatively salty sweat can tolerate less overdrinking before developing hyponatraemia. Furthermore, if they rely solely on water or weak electrolyte solutions for fluid replacement and consume only electrolyte-poor foods, it is possible for them to become both dehydrated and hyponatraemic. Sports beverages can help to delay the development of hyponatraemia in these situations. Fluid replacement strategies designed to prevent symptomatic hyponatraemia should target both fluid and electrolyte intake. Finally, athletes should be encouraged to develop customised fluid replacement programmes, through trial and error, that ensure that enough fluid is consumed to prevent excessive dehydration without risking hyperhydration.
What this study adds
-
A mathematical model is used to illustrate the complex interactions between exercise intensity, climatic conditions, sweat composition, total body water, drinking rate, and drink composition for sustaining fluid balance and normal natraemia
-
Strategies to prevent exercise associated hyponatraemia should target fluid intake but also consider solute losses
What is already known on this topic
-
Exercise associated hyponatraemia, although rare, can compromise performance and health
-
It most often afflicts athletes performing prolonged exercise lasting four hours or longer and who drink over-aggressively; female and slower participants are also at higher risk of developing the condition
Acknowledgments
The opinions an assertions contained herein are the private views of the author(s) and are not to be construed as official or as reflecting the views of the Army or Department of Defense. Approved for public release; distribution unlimited.
REFERENCES
Commentary 1
This modelling study again shows that it is the overconsumption of fluid that is the primary factor causing the symptomatic hyponatraemia that develops in 42 km marathon runners and that sodium losses may play a contributory role, in addition to excessive fluid consumption, in competitors in longer events such as the Ironman triathlon. Although the first conclusion has been proved in prospective studies, the latter has yet to be confirmed in appropriate clinical trials. The distinction is important because, if the authors are correct, the ingestion of electrolyte-containing sports drinks may assist in the prevention of this condition in very prolonged exercise such as the Ironman triathlon, whereas the study of Almond et al1 has clearly shown that this is not the case in the standard 42 km marathon. Yet it was the zealous overmarketing of sports drinks to slow running marathon runners and Ironman triathletes that produced the epidemic of this condition, especially in the United States, beginning in the 1990s. We must be careful that we do not hand the commercially driven marketeers of these products more ammunition to continue their zealous oversell. Two factors may yet disprove the present authors’ second prediction. Firstly, everyone with exercise associated hyponatraemia must be suffering from the syndrome of inappropriate secretion of anti-diuretic hormone.2 An under-recognised feature is that athletes with the syndrome will excrete any sodium present in an electrolyte-containing drink while avidly retaining the excess fluid, thereby aggravating the hyponatraemia.2 Secondly, there is an unrecognised internal body store—the osmotically inactive but exchangeable sodium store—that potentially dwarfs the amount of any sodium that can be ingested during exercise. It may be that, what appears to be the contribution of sodium losses in sweat to the production of symptomatic hyponatraemia, may really be the failure to mobilise ionised sodium from these osmotically inactive internal body stores.2 The function of these stores appears to be to buffer large changes in serum sodium concentrations when either large sodium or water losses or gains are incurred, especially during prolonged exercise.2 The authors’ other important conclusion is that the modest drinking guidelines promoted by the International Marathon Medical Directors Association (IMMDA) appear to be safe and appropriate for most exercise conditions.
Commentary 2
The authors’ use of a mathematical model (the Nguyen-Kurtz equation1) to predict how plasma sodium concentration changes with time has important implications. Firstly, consistent with observational reports,2,3 it points to fluid overload as the prime pathogenetic factor in exercise associated hyponatraemia. Secondly, their model predicts that sodium plus potassium loss can also have a significant impact on plasma sodium concentration. To further evaluate this second parameter, the Nguyen-Kurtz equation1 can be used to calculate how plasma sodium concentration changes when total body water (TBW) does not change. Zero change in TBW means that the athlete has exactly replaced fluid lost.
For ΔTBW = 0, the Nguyen-Kurtz equation simplifies to:
[Na+]2p = [Na+]1p + 1.03ΔE/TBWi
where [Na+]2p is the new plasma sodium concentration (mEq/l), [Na+]1p is the initial plasma sodium concentration (mEq/l), ΔE is the change in the sum of sodium and potassium (mEq), and TBWi is the initial total body water.
As [Na+]2p − [Na+]1p = Δ[Na+]p,
Δ[Na+]p = 1.03ΔE/TBWi
As ΔE = (DR × [E]drink − SR × [E]sweat) × t
and DR = SR,
ΔE = SR([E]drink − [E]sweat) × t
where DR is drinking rate, SR is sweat rate (litres/h), [E]drink is the sum of the concentrations of sodium and potassium in ingested fluid (mEq/l), [E]sweat is the sum of the concentrations of sodium and potassium in sweat (mEq/l), and t is the time (hours).
Therefore
Δ[Na+]p = ((1.03 × SR([E]drink − [E]sweat))/TBWi) × t
An hourly rate of change in plasma sodium concentration can be readily obtained by equating time to one hour:
Δ[Na+]p,1h = (1.03 × SR([E]drink − [E]sweat))/TBWi
For example, consider an athlete with TBWi = 40 litres, sweat rate = 1 litre/h, [E]sweat = 50 mEq/l and ingesting a sports drink with [E]drink = 22 mEq/l. This athlete is predicted to lower [Na+]p by 1.03(22 – 50)/40 = −0.72 mEq/l per hour. Notice that if [E]sweat = [E]drink, and ΔTBW = 0, then there would be no change in [Na+]p.
Clearly, sports drinks have some benefit. However, this benefit does not extend to cases in which there is fluid overload, in other words, a positive change in TBW. An athlete with 40 litres TBW will, by retaining 2 litres of sports drink, lower [Na+]p from 140 to 133.3 mEq/l compared with 132.2 mEq/l with plain water. The concentration of the sports drink of 22 mEq electrolyte/litre is, after all, quite small against a sodium plasma concentration of 140 mEq/l.
Observational tests of the authors’ model for long exercise times are sparse. The laboratory studies of Barr et al4 and Sanders et al5 over six and four hours respectively are, however, consistent both in sweat rates and electrolyte loss with the authors’ predictions. During events, sweat rates and electrolyte loss rates can only be indirectly estimated. Glace et al6 tracked electrolyte and fluid ingestion and pre-race and mid-race plasma sodium concentrations in a 160 km run held in hot weather (21–38°C). Of note are the prodigious amounts of water (mean (SD) 19.4 (5.6) litres) and electrolyte (16.4 (6.8) g Na+ and 7.2 (3.1) g K+) consumed by race finishers under these harsh conditions. Plasma sodium concentrations after the race reported by Glace et al are consistent with the authors’ predictions.
Commentary 3
This paper makes a significant contribution to our understanding of the aetiology of exercise related hyponatraemia and identifying possible practical approaches that can decrease the risk. The authors used a unique and scientifically sound approach in developing a theoretical model to predict the development of hyponatraemia under a variety of circumstances. Although this scientific model must now be tested in laboratory and field settings to confirm, refute, or refine its predictions, its basic tenets agree with existing findings and further underscore the dangers associated with drinking too much sodium-free fluid during prolonged exercise.
Commentary 4
Before the insightful data of Speedy et al1 were published, authorities viewed exertional hyponatraemia solely as a problem of fluid overload—that is, weight gain. The observations of Speedy et al, recorded at the New Zealand Ironman triathlon, provided evidence for a new paradigm: athletes became hyponatraemic but lost body weight during prolonged endurance exercise. Their graph of the plasma sodium concentrations of 330 ultradistance triathletes (fig 1)1 tantalisingly suggested that there are multiple causes of exertional hyponatraemia, forcing physiologists and doctors to re-examine their views and clarify mechanisms.
The present paper advances this process considerably. The authors’ use of a simple mathematical model to predict the effects of different drinking behaviours on hydration status and plasma sodium concentration shows the theoretical means by which different varieties of this illness—for example, hypovolaemic hyponatraemia, hypervolaemic hyponatraemia—develop. To the benefit of ultraendurance athletes, this model incorporates physiologically realistic sweat sodium concentrations, sweat rates, body sizes, running speeds, and environmental conditions.
Previous studies provided clues such as: runners with smaller total body water—for example, women—are at greater risk of overhydration; runners who are on the course longer drink more because they tend to linger at aide stations. The present mathematical model allows the reader to conceptualise exertional hyponatraemia as a multifaceted illness. It shows that the answer to the question, “How does exertional hyponatraemia develop?” is more complex than our previous answer, “By consuming too much water.”
The reader receives at least two insightful messages from figs 1–4. Firstly, any runner can develop exertional hyponatraemia when certain conditions exist—that is, an intense desire to consume as much water as possible—but the volume of fluid consumed in excess of sweat loss may not be huge. As shown in this paper, a 50 kg ectomorphic runner needs to consume only 600 ml/h to experience a plasma sodium concentration of 123–126 mEq/l. Secondly, and most importantly in my opinion, a high sweat sodium concentration is a critical aetiological factor in hypovolaemic hyponatraemia. This fact was not widely accepted two years ago, but today has important implications for athletes. It suggests that heredity and training/acclimatisation state—that is, inherently possessing concentrated sweat, high sweat rate, or small total body water—interact as exertional hyponatraemia develops.
I appreciate the opportunity to comment on this manuscript because it will move our understanding of a life threatening illness from a state of perplexed, often heated, debate to thoughtful science—a rare experience in the life of a scientist or peer reviewer. I believe that this model will serve as a guide for future laboratory investigations and field studies by virtue of its numerous testable hypotheses. It will also provide coaches and athletes with a comprehensive list of factors to consider as they plan training and competitive efforts.
REFERENCES
Footnotes
-
Competing interests: none declared