Article Text

Abstract
Objective: To determine the interobserver and intraobserver reliability of the interpretation of MRIs for supraspinatus tendinosis.
Methods: In the interobserver trial, the MRIs of 52 athletes’ shoulders were observed by 3 observers on one occasion within a 2-month period. All 52 images were read by the most experienced musculoskeletal radiologist on 3 different occasions on separate days without access to the previous readings for the intraobserver trial. Supraspinatus tendinosis was graded using a modified 4-point scale from grades 0 to grade 3.
Results: The grading of MRI-determined supraspinatus tendinosis was reliable, having an intraclass correlation (ICC) of 0.85 when assessed by the single well-trained observer. Interobserver reliability was only fair to good (ICC = 0.55).
Conclusions: Supraspinatus tendinosis can be accurately identified on MRI with little variation by a single well-trained observer. Interobserver reliability was only fair to good. Our data indicated that the reliability of the assessment was much greater in more experienced radiologists than in those with less experience.
- ICC, intraclass correlation
- PD, proton density
Statistics from Altmetric.com
MRI has proven to be useful in the assessment of rotator cuff injuries. MRI is a non-invasive method of imaging and is unique in that it allows the differentiation of soft tissue structures.1 Improvements in MRI techniques, including fast spin-echo imaging and fat saturation, have facilitated demonstration of tendinous abnormalities of the rotator cuff.
The MRI findings of rotator cuff tendinopathy are characterised by thickened inhomogeneous rotator cuff tendon with increased signal intensity on all pulse sequences.2 Fluid intensity filling an incomplete gap in the tendon on fat-suppressed T2-weighted sequences changes are seen on MRI for partial-thickness tears.3 On MRI, an area of high signal intensity on all pulse sequences outlines complete disruption of the tendon.4
MRI is a non-invasive technique for investigating lesions of the rotator cuff.5,6,7,8,9,10,11 It is widely used in clinical practice to investigate shoulder problems in patients, particularly those relating to the rotator cuff and to glenohumeral joint instability. Advances in technology have greatly improved the quality of MRI.
Many studies have demonstrated acceptable levels of sensitivity, specificity and accuracy in the diagnosis of cuff and capsulo-labral pathology.12–17 The reliability of assessing supraspinatus tendinopathy has not been determined.
MATERIALS AND METHODS
Subjects
Under ethical approval from the SouthEast Health Human Research Ethics Committee (Sydney, Australia), 52 elite swimmers, of club to international levels, participated in the MRI reliability study. The group consisted of 28 (54%) males and 24 (46%) females. They were aged between 13 and 25 years, with a mean (SD) age of 15.5 (2.7) years and a median age of 16 years. The swimmers underwent an MRI of a single shoulder: either the dominant shoulder if asymptomatic or the most affected shoulder if symptomatic. Each swimmer’s evaluation included a shoulder pain and function examination and a swimming training profile before the MRI. Swimmers were excluded if they had any previous surgery, fracture of the shoulder, or inability or unwillingness to participate in the MRI and clinical shoulder examinations. Each participant of the study was given an information sheet outlining the MRI investigation and a consent form to complete.
Study design
One observer made three readings of the same MRIs (intraobserver trial) and three observers independently made readings on the same set of images (interobserver trial).
MRI UNIT
Oblique coronal proton density (PD) and fat-suppressed T2, sagittal T2 and axial PD sequencing were performed on a Signa 1.5 T superconducting magnet, Hi Speed MRI unit (General Electric Medical Systems, Milwaukee, Wisconsin, USA), using system software V.9.1, slew rate 77 T/m/s, 33 mm T gradient amplitude, utilising a high resolution, non-arthrographic technique with a four-channel phased array shoulder coil (Medical Advances, Milwaukee, Wisconsin, USA). Table 1 outlines the MRI protocol used in this study.
MRI protocol for reliability of the MRI-determined supraspinatus tendinosis examination
SUPRASPINATUS TENDINOSIS GRADING
Tendinopathy is characterised by an increased intrasubstance signal on short TE sequences that is not as bright as the fluid on T2-weighted images.18 The involved tendons may be of a normal calibre or thickened. Differentiating tendinosis with a morphologically normal tendon from the magic angle phenomenon is facilitated by signal alteration that persists on long TE images in tendinopathy.16 In this study, supraspinatus tendinosis was graded using a modified 4-point scale from 0 to 3 based on previous studies.4,13,19,20
Diagnosis was based on the appearance of the rotator cuff tendons (grading system) and the presence or absence of signs denoting involvement of the subacromial bursa and subacromial–subdeltoid plane.13,20
In our study, grade 0 (normal) was a tendon with complete homogeneous low intensity on all pulse sequences or minor intratendon signal hyperintensity consistent with magic angle artefact (fig 1 A), grade 1 (mild tendinosis) mild focal increase in tendon signal on PD and fat-suppressed T2 sequencing not equal to that of fluid (fig 1 B), grade 2 (moderate tendinosis) moderate focal increase in tendon signal on PD and fat-suppressed T2 sequencing not equal to that of fluid (fig 1 C), and grade 3 (marked tendinosis) marked a generalised increase in tendon signal without frank fluid signal intensity (fig 1 D).

MRIs of the shoulder illustrating tendinosis grading. (A) Grade 0 (normal). A tendon with complete homogeneous low intensity on all pulse sequences or minor intratendon signal hyperintensity consistent with magic angle artefact. (B) Grade 1 (mild tendinosis). Mild focal increase in tendon signal on PD and fat-suppressed T2 sequencing not equal to that of fluid. (C) Grade 2 (moderate tendinosis). Moderate focal increase in tendon signal on PD and fat suppressed T2 sequencing not equal to that of fluid. (D) Grade 3 (marked tendinosis). Marked generalised increase in tendon signal without frank fluid signal intensity.
Interobserver reliability trial
Three musculoskeletal radiologists received for the interobserver reliability trial. The experience levels of the three musculoskeletal radiologists varied. The first radiologist had 9 years of experience in musculoskeletal MRI. The second radiologist had a 1-year training fellowship and 1 year in the clinical practice of MRI reading. The third musculoskeletal radiologist had much less experience in MRI reading. For each swimmer, the three musculoskeletal radiologists (ie, observers) recorded their supraspinatus tendinosis grade using the standardised criteria (fig 1A–D).
All three observers were blinded to the identity of the swimmers, and each of them read all 52 images on one occasion. Before the reading, each observer was briefed on the study protocol by the most experienced radiologist and given the criteria for grading, together with the MRI forms for the supraspinatus tendinosis reliability test. The readings were performed within 2 months of each other.
Intraobserver reliability trial
The intraobserver reliability trial was based on the same 52 swimmers. The most experienced musculoskeletal radiologist read all 52 images on 3 different occasions without access to the previous readings.
Statistical analysis
Intraobserver reliability and intraobserver reliability trails were analysed for their intraclass correlation coefficients (ICCs) with SPSS, using a 2-way random-effects model with absolute agreement (2, 1). According to Fleiss21,22, an ICC value <0.4 represents poor reliability, values >0.75 represent excellent reliability and values between 0.4 and 0.75 represent fair to good reliability (194–196).
RESULTS
Incidence of tendinosis
Of the 52 shoulders examined, 69% (25 male, 11 female) had MRI-assessed tendinosis, 27 (52%) grade 1, 8 (15%) grade 2 and 1 (2%) grade 3.
Clinical relevance
Some authors have identified abnormal signal intensity of the supraspinatus tendon15,19,23–34 of asymptomatic individuals. Of the elite swimmers in our study, 36/52 (69%) had MRI-determined supraspinatus tendinosis. Each of these swimmers had a positive impingement sign. The positive impingement sign correlated significantly with the MRI assessment of tendinosis (r = 0.49, p<0.001).
Reliability of the supraspinatus tendinosis grading
Interobserver reliability trial
Figure 2 shows the interobserver ICC for the three observers’ readings for the MRI-determined supraspinatus tendinosis grading. Interobserver reliability of the readings for MRI-determined supraspinatus tendinosis grading had an ICC = 0.55, with a 95% CI ranging from 0.27 to 0.72. According to Fleiss,21,22 this level of agreement between the three radiologists is rated as fair to good.
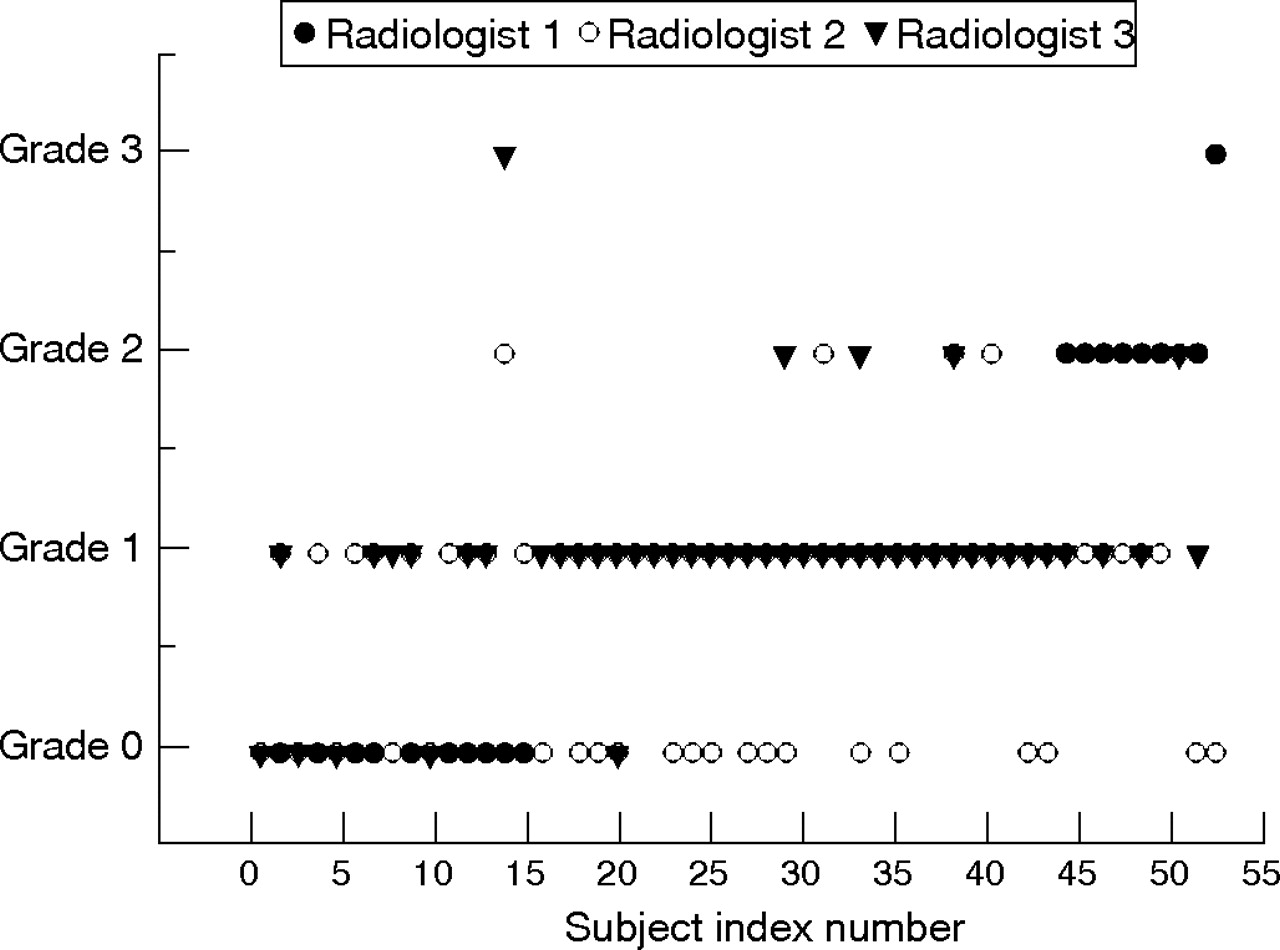
Interobserver reliability of supraspinatus tendinosis grading.
Intraobserver reliability trial
Figure 3 shows the intraobserver ICC for three readings. Intraobserver reliability of readings of the MRI-determined supraspinatus tendinosis grading was ICC = 0.85, with the 95% CI between 0.72 and 0.9. On the basis of the criteria of Fleiss,21,22 this level of agreement between the three readings is rated as excellent.

{kind=link}
{kind=link}
{kind=link}
Intraobserver reliability of supraspinatus tendinosis grading.
DISCUSSION
In elite swimmers, supraspinatus tendinopathy is one of the main causes of shoulder pain. Improvements in MRI, including fast spin-echo imaging and fat saturation, have facilitated demonstration of tendinous abnormalities of the rotator cuff. MRI changes in the rotator cuff and tendinitis have been correlated with findings from conventional double-contrast arthrography,5,8,20,35,23 computed arthrotomography,5,8 arthroscopy11,23 and histological evaluation of the rotator cuff.18
Supraspinatus tendinopathy can be detected using MRI. Kjellin et al18 compared MRIs and histological analysis on cadaver shoulders and showed that increased signal intensity on PD-weighted images (without further increased signal intensity on T2-weighted images) and an indistinct margin at the articular side of the supraspinatus tendon corresponded to eosinophilic, fibrillar, and mucoid degeneration and scarring. Areas of increased signal intensity on T2-weighted images were associated with severe degeneration and disruption of the supraspinatus tendon.18 A study by Gagey et al17 and Williams et al12 also found that gross anatomical and MRI abnormalities of the rotator cuff corresponded to histological changes consistent with tendon degeneration. We observed an excellent correlation between MRI-determined tendinopathy and a positive impingement sign in swimmers.
The sensitivity and specificity of magnetic resonance scanning in the diagnosis of partial-thickness and full-thickness defects of the rotator cuff have been well documented.13,36,37 We found that the grading of MRI-determined supraspinatus tendinosis grading was reliable (ICC = 0.85) when assessed by a single well-trained observer. However, the interobserver reliability was only fair to good (ICC = 0.55). Our data indicated that the reliability of the assessment was much greater in more experienced radiologists and less in the junior radiologist.
What is already known on this topic
-
MRI is a useful, non-invasive technique for the assessment of shoulder problems, particularly those relating to the rotator cuff and glenohumeral joint instability. The reliability of assessing supraspinatus tendinopathy using MRI, however, has not been determined.
What this study adds
-
In elite swimmers, supraspinatus tendinopathy is one of the main causes of shoulder pain.
-
This study found MRI assessment of tendinopathy to be reliable with a single well-trained observer and less so with other observers.
-
There was an excellent correlation between MRI-determined tendinopathy and a positive impingement sign in swimmers.
Acknowledgments
This study was supported by St George Hospital/South East Sydney and Illawarra Area Health Service. We thank the New South Wales Institute of Sport, its coaches, swimmers and their parents for their enthusiastic participation, and the Castlereagh Imaging group for their expertise in MRI interpretation.
REFERENCES
Footnotes
-
Published Online First 5 February 2007
-
Competing interests: None declared.