Article Text

Abstract
Background Exercise-associated hyponatraemia (EAH) is a potentially fatal cause of collapse in endurance exercise. It is understood to be a dilutional hyponatraemia caused by an increase of total body water relative to the amount of exchangeable sodium stores. Fourteen runners presented to one London hospital with symptomatic EAH several hours after finishing the 2003 London Marathon, and more recently, a young male runner died from the complications of severe EAH after crossing the finish line of the London Marathon.
Objectives To determine the incidence of EAH in runners in the London Marathon.
Methods Volunteers were recruited at race registration where they were weighed, had blood tests and completed a demographic and experience questionnaire. Weights, blood tests and a fluid intake questionnaire were repeated after the finish. Blood was analysed on-site using hand-held i-STAT blood analysers.
Results Of the 88 volunteers, 11 (12.5%) developed asymptomatic hyponatraemia (serum sodium 128–134 mmol/l). They consumed more fluid (p<0.001) and gained more weight (p<0.001) than did those without hyponatraemia.
Conclusions A significant proportion (12.5%) of healthy volunteers developed asymptomatic hyponatraemia running a marathon in cool conditions. On average, these runners consumed more fluid and gained more weight than did non-hyponatraemic runners, although fluid intake was not related to weight gain in this study. Four of the 11 hyponatraemic runners lost weight over the course of the marathon, strengthening the case for an additional factor, such as inappropriate antidiuretic hormone release during exercise, in the development of EAH.
Statistics from Altmetric.com
Introduction
Over 710 000 runners have successfully completed the London Marathon in its 28-year history. While it is generally considered to be a safe event, medical staff at the marathon assess and treat up to 2% of runners annually for problems ranging from muscle cramps and exercise-associated collapse to hyperthermia and cardiac arrest. Marathon runners are at risk of collapse from causes related to exercise1 not commonly seen in the general population. A life-threatening cause of collapse during endurance exercise is exercise-associated hyponatraemia (EAH), which has been responsible for the deaths of at least five runners in the USA and UK in the last few years.2,–,5
EAH is defined as serum sodium concentration ([Na+]) less than 135 mmol/l during or up to 24 h after prolonged physical activity.4 The disorder is broadly classified into symptomatic or asymptomatic hyponatraemia by the presence or absence of signs or symptoms rather than by the absolute value of [Na+] as this is not a reliable predictor of clinical severity.4 Early signs and symptoms of hyponatraemia are non-specific such as bloating, nausea, vomiting and headache. The more severe manifestations of hyponatraemia, hyponatraemic encephalopathy caused by cerebral oedema, can lead to confusion, seizures, coma and death.4
EAH is widely understood to be a dilutional hyponatraemia caused by an increase of total body water relative to the amount of exchangeable sodium stores.4 Aetiological factors include excessive fluid consumption in excess of total body fluid losses,4 6 altered renal function,3 7 longer race duration,8 female gender9 and smaller size.6 Excessive sodium loss may also have an impact on the development of EAH, although it has not been shown to be a primary causative factor.4
In an attempt to reduce the morbidity and mortality associated with EAH, the International EAH Consensus Development Conference has met twice in recent years, publishing Consensus Statements with recommendations for fluid replacement during endurance exercise.4 10 Guidance has also been produced by the American College of Sports Medicine11 and the International Marathon Medical Directors Association.12 Yet in studies on volunteers running marathons in Europe and the USA, the incidence of hyponatraemia is between 3% and 22%.13 14 After running the London Marathon in 2003, 14 runners presented to one London hospital with symptomatic EAH.15 More recently, a young male runner died of pulmonary and cerebral oedema consequent to EAH after crossing the finish line of the London Marathon.5 This study aimed to examine the incidence of hyponatraemia in finishers in the London Marathon.
Method
Study setting
The London Marathon is a full 42.2 km marathon held over a flat city course in the spring. Bottles of water (330 ml) are available from water stations situated every mile (1.6 km) from the third mile onwards. Additionally, 330 ml sachets of a sports drink containing 22 mmol/l [Na+]16 are available at 4.6, 8.8, 15.3 and 23.7 miles. Runners are advised in the prerace literature not to drink at every station and not to drink excessively.
Study population
Healthy volunteers were recruited at race registration from runners participating in the 2006 London Marathon. Written consent was obtained from each volunteer. Each was weighed in light clothing and completed a questionnaire detailing demographics and marathon experience. A 2 ml sample of venous blood was drawn from the antecubital fossa and analysed immediately for sodium on self-calibrating, handheld i-STAT blood analysers (Abbott Point of Care, East Windsor, New Jersey, USA). (The i-STAT analyser has been shown to have excellent reliability for measuring [Na+] when compared to simultaneous laboratory analyser measurements.17 18 It has been used with success in the marathon setting14 19 and has been in use in the medical tents of the London Marathon since 2005.) As soon as possible after finishing the marathon, volunteers were asked to report to the medical tent on-site where they were weighed on the same scales, had a postrace blood test analysed in the same fashion as before and completed a fluid intake questionnaire. Estimated fluid intake was calculated by multiplying the number of drinks consumed by 330 ml (the volume of a water bottle or sports drink sachet.)
Statistical analysis
Statistics were calculated using GraphPad Prism (GraphPad Software, San Diego, California, USA). Descriptive statistics were used to illustrate demographics and to estimate the incidence of hyponatraemia. Differences between groups were analysed with independent t tests for continuous variables, χ2 for categorical variables and Mann–Whitney U tests for non-parametric data. Where appropriate, skewed data were transformed to a logarithmic scale to follow a normal distribution. Relationships between continuous variables were analysed using Pearson's Product Moment correlation and linear regression. Data are presented as “mean (SD)” unless otherwise stated. Significance was defined as p<0.05.
Results
The event was held in wet, rainy conditions with air temperature 9–12°C, humidity 73% and wind speed 3–9 km/h. Wet bulb globe temperature (WBGT) was 9°C at the start. The race started with 33 578 runners; 33 222 finished. At the finish, 603 runners were seen in the medical tents. No cases of symptomatic EAH were found among these runners.
Volunteers
Demographics
One hundred and sixteen volunteers were recruited. Prerace data sets on five runners were incomplete, and they were not included in further analysis. The remaining 111 comprised 42 female and 69 male runners with an average age of 38.8 years. Eighty-eight of these 111 (79.3%) returned for postrace tests after the marathon. The returning runners had a lower baseline [Na+] (138 (3) mmol/l, p=0.044) and ran the marathon 33 min faster (p=0.005) than did those who did not return for blood tests (baseline [Na+] 140 (2) mmol/l) (figure 1). Otherwise, the two groups were not significantly different in terms of age, sex, body mass index (BMI) or previous experience.
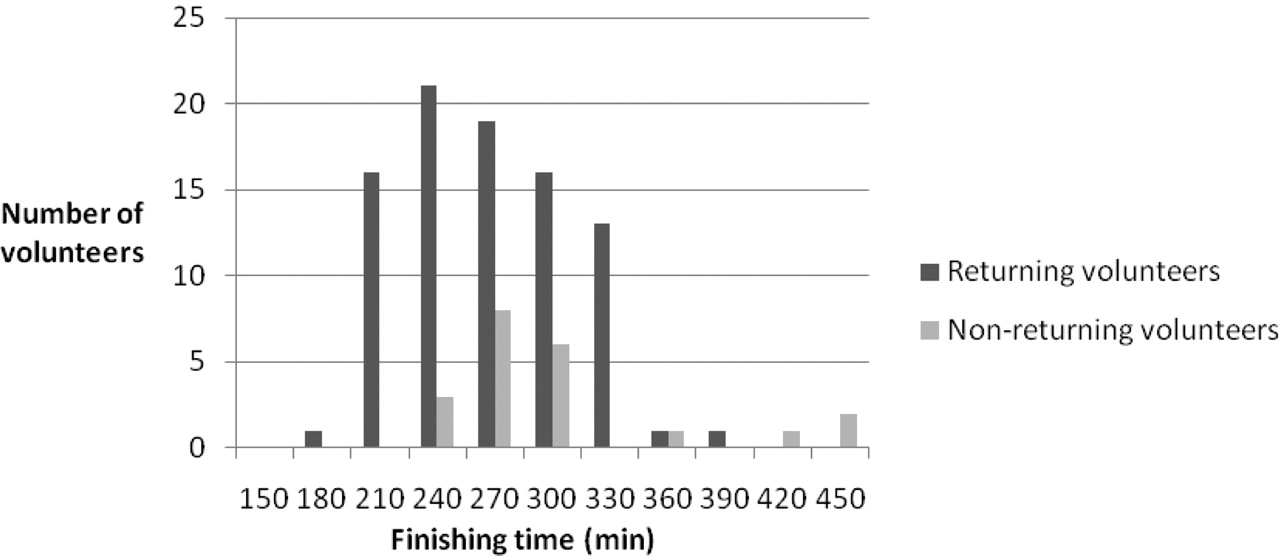
Finishing times of all study volunteers.
All except two non-returners finished the marathon. One did not start the race, and another withdrew after tripping and injuring her leg. A third runner collapsed after finishing and was reviewed by the medical team. His [Na+] was found to be 138 mmol/l, excluding the diagnosis of EAH.
Postrace results
Asymptomatic hyponatraemia was identified in 11 (12.5%) of the 88 volunteers. Their [Na+] ranged from 128 to 134 mmol/l. This group was not significantly different from the volunteers that did not develop hyponatraemia in terms of age (p=0.412), sex (p=0.084, χ2=2.989), prerace weight (p=0.429), BMI (p=0.231) or previous marathon experience (median number of previous marathons: p=0.545; proportion with experience: p=0.865, χ2=0.029) (table 1). There was no significant difference in finishing times between hyponatraemic and non-hyponatraemic runners (table 2). There were no cases of symptomatic hyponatraemia.
Demographics of returning volunteers*
Hyponatraemic and non-hyponatraemic volunteers' finishing times, weight change and fluid intake*
Fluid intake
Average fluid intake over the course of the marathon was 2144 ml; however, runners who developed hyponatraemia reported a significantly larger fluid intake (3683 ml vs 1924 ml, p=0.001) and consumed fluid at a higher rate than those without hyponatraemia (843 ml/h vs 451 ml/h, p=0.002) (table 2). There was no difference in frequency of drinking (p=0.138) or frequency of urination (p=0.099) during the race. Runners who developed hyponatraemia reported drinking more fluid in the time between finishing and their postrace review than did those who did not develop hyponatraemia, but this difference was not statistically significant (271 vs 186 ml, p=0.200).
Weight change
Runners with hyponatraemia completed the marathon 0.46 (1.65) kg heavier than their baseline weight, while those without hyponatraemia lost 1.46 (1.70) kg (p<0.001) over the same period. Relative weight change was also significantly different between the two groups (0.76 (2.8)% vs −1.9 (−2.2)%, p<0.001) (table 2).
Sodium changes
Runners who developed hyponatraemia had a lower baseline [Na+] (albeit within the normal reference range) than those who did not develop hyponatraemia. They also exhibited a greater fall in [Na+] than those without hyponatraemia (table 3).
Volunteers' pre- and postmarathon [Na+] and change in [Na+]
Among all volunteers, postmarathon [Na+] had a strong linear relationship with change in [Na+] (r2=0.772, p<0.001) (figure 2).

Postmarathon [Na+] plotted against change in [Na+].
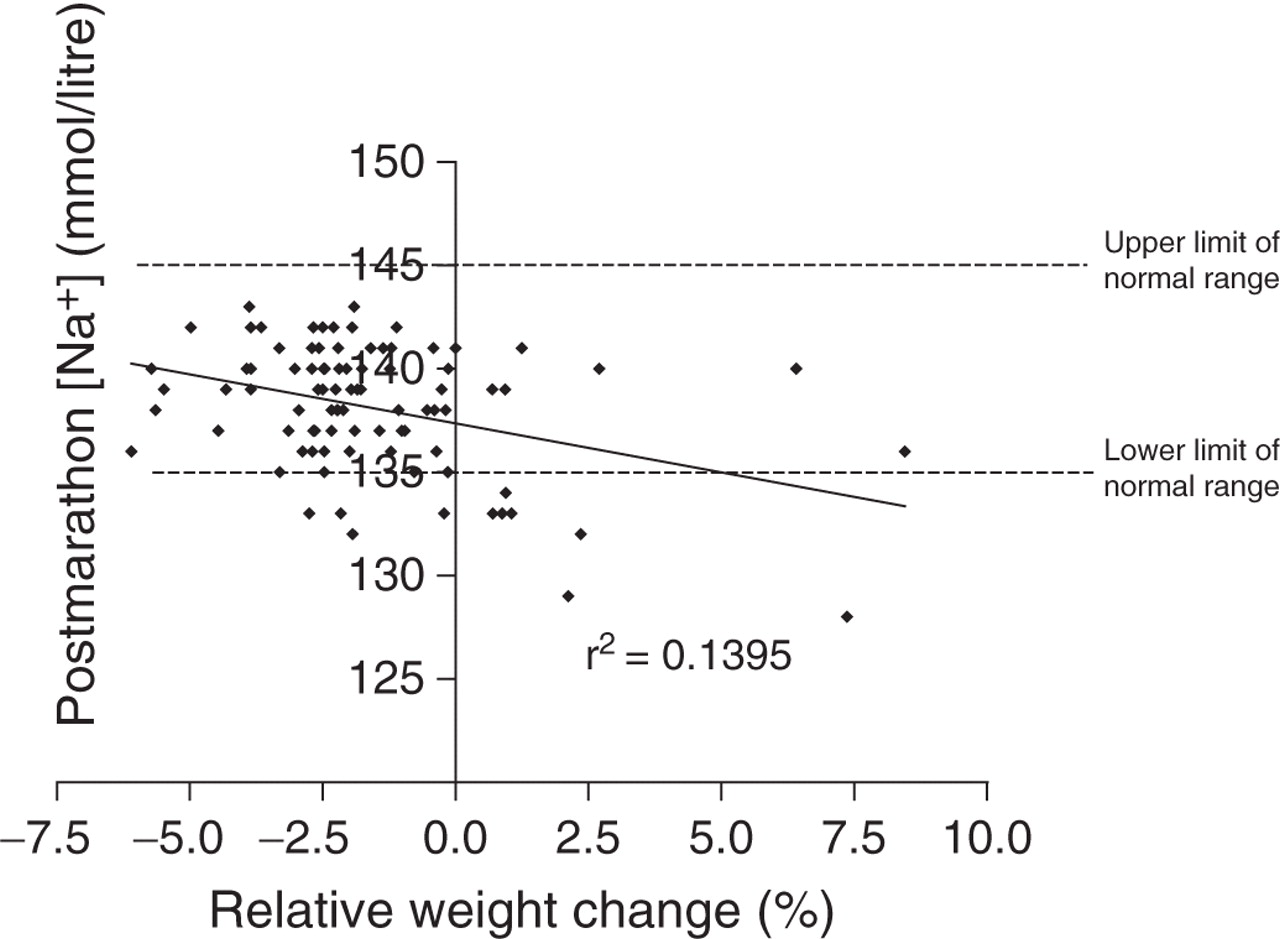
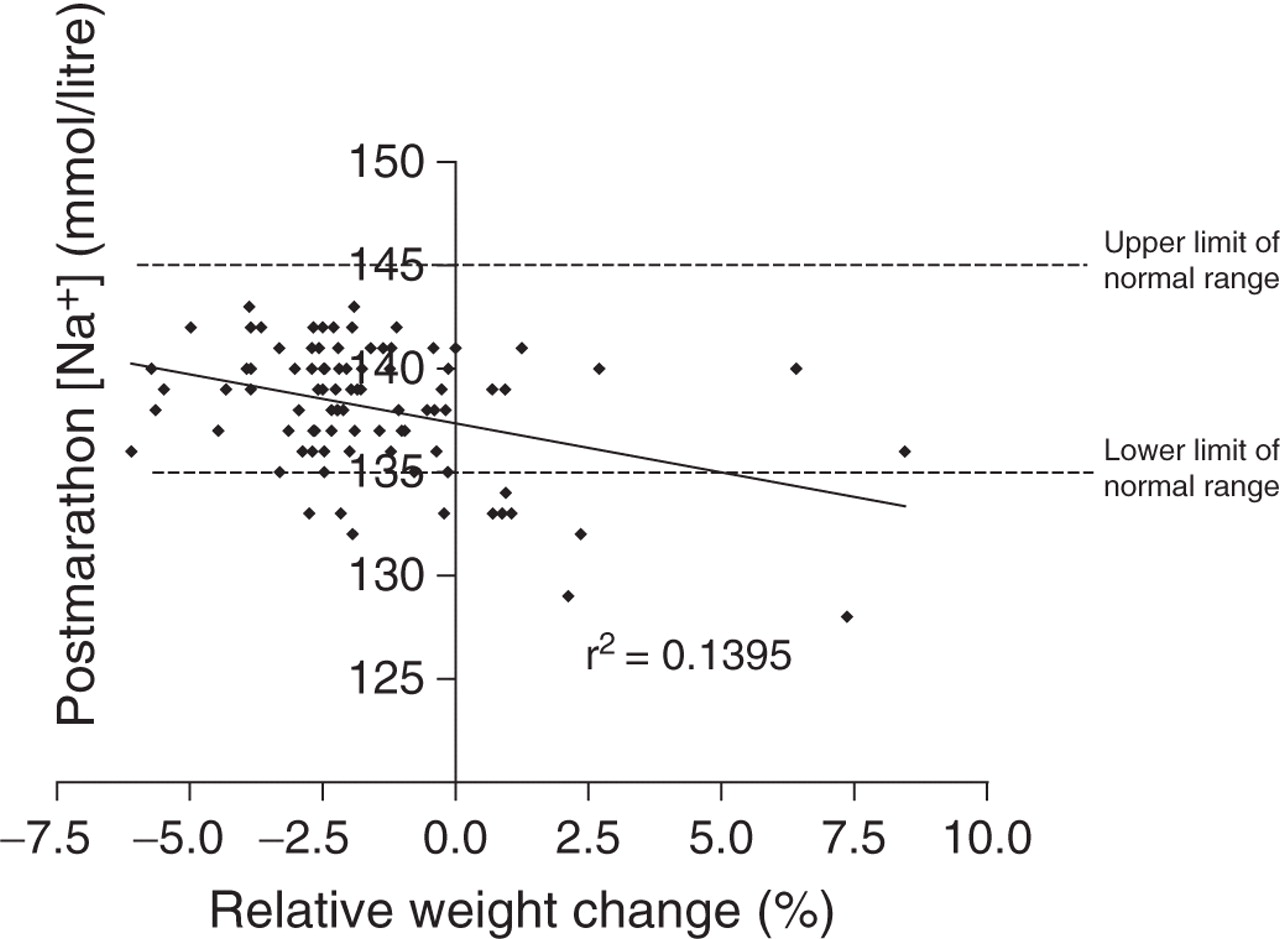
Postrace [Na+] was inversely related to fluid intake (r2=0.160, p<0.001) (figure 3) as well as to absolute weight change (r2=0.133, p<0.001) and relative weight change (r2=0.140, p<0.001) (figure 4). These relationships were similar when the change in [Na+] was modelled against fluid intake (r2=0.169, p<0.001) and absolute (r2=0.096, p=0.003) and relative weight change (r2=0.097, p=0.003). Although there was a positive trend between fluid intake and weight change, this relationship was not significant (p=0.217).

Postmarathon [Na+] against fluid intake.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Postmarathon [Na+] versus relative weight change.
Discussion
Principal findings
Eleven of a control group of 88 healthy volunteers (12.5%) running the London Marathon had asymptomatic hyponatraemia at the finish. On average, these runners consumed more fluid and gained more weight than did non-hyponatraemic runners, although fluid intake was not related to weight gain in this study, and four of the 11 hyponatraemic runners lost weight over the course of the marathon. Female gender and slow race pace were not associated with the development of EAH in this study. Five of the 11 runners who developed hyponatraemia finished the race within 4 h.
Discussion
The primary aetiological factor in the development of EAH is fluid consumption in excess of total body fluid losses.4 6 8 Athletes drink more during exercise in hot conditions than in cool conditions,20 and unusually hot environmental conditions are a recognised risk factor for EAH.4 A cluster of 14 cases of EAH after a previous London Marathon was partly attributed to the hot conditions on the day (WBGT 15.2°C, 0.43 cases of symptomatic EAH per 1000 finishers); cooler conditions on each of the following 2 years were associated with only single cases (2004: WBGT 10.8°C, 0.03/1000; 2005: WBGT 12°C, 0.03/1000).15 In the cool, wet conditions encountered during this current event, none of the collapsed runners seen by medical staff in the medical tents had hyponatraemia (unpublished data). However, despite these conditions, 12.5% of a group of healthy volunteers running the London Marathon drank sufficient quantities of fluid to lower their [Na+] by an average of 6 mmol/l, thereby developing hyponatraemia.
Weight change is a useful objective measure of fluid intake6 and retention.3 Consistent with data from the Boston Marathon,6 hyponatraemic runners in this study reported a significantly larger fluid intake and exhibited considerable weight gain compared with non-hyponatraemic runners. Significant inverse relationships between [Na+] and weight change and [Na+] and fluid intake in this study lend support to the findings of Almond et al,6 providing further evidence for the role of excessive fluid intake in the aetiology of EAH. However, in this study, estimated fluid intake was not related to weight gain. Several reasons may account for this. First, fluid intake was self-reported and subject to recall bias. Second, runners should expect to lose some weight over the course of a marathon due to substrate oxidation;21 neutral weight balance therefore suggests over-hydration. A recent study calculated that weight loss of 0.75 kg was the minimum necessary over the course of a marathon to reduce the risk of developing hyponatraemia.14 Finally, weight gain and subsequent EAH may be related to factors other than fluid intake. The volumes consumed by participants in this study were on the whole not exceptional quantities, although the differences between the two groups are significant. The larger group of 77 unaffected runners drank less than 2 litres each over the course of the race, while runners who developed hyponatraemia drank an average of over 3.5 litres per person. Unaffected runners drank at an average rate of 450 ml/h; hyponatraemic runners drank 842 ml of fluid/h on average, almost twice the rate. However, four of the hyponatraemic runners in this study consumed fluid at rates (less than 450 ml/h) unlikely to cause fluid overload purely by overwhelming the renal excretory capacity. Additionally, four hyponatraemic runners actually lost weight over the course of the run (two of these four consumed fluid at less than 450 ml/h). Inappropriate antidiuretic hormone (ADH) release during exercise causing altered renal function and secondary fluid retention is one such mechanism by which EAH can develop in the absence of excessive fluid intake.3 4 22 Inappropriate ADH release increases the risk of developing EAH even when relatively “normal” volumes of fluid are consumed.4 Non-osmotic stimulation of ADH causing EAH has been linked to the release of interleukin-6 in exertional rhabdomyolysis in marathon runners.3 23 Evidence of inappropriately concentrated urine would be a useful surrogate marker of the syndrome of inappropriate secretion of antidiuretic hormone (SIADH) for future studies.
Recent experience from the London Marathon indicates that runners with hyponatraemia have tended to present to hospital several hours after finishing the event apparently well, suggesting that fluid consumed after exercise may add to the risk of developing hyponatraemia.3 8 One theory19 24 suggests that as blood flow returns to the gut with the cessation of exercise and before the renal system has returned to normal, increased absorption of water from the gut contributes to fluid overload and the subsequent risk of EAH. Runners in this study who developed hyponatraemia tended to drink more after the race than those who did not develop hyponatraemia, but this difference did not reach statistical significance. Persistent SIADH may explain postrace onset of EAH as runners continue to consume fluids under the mistaken impression that delayed urination signifies dehydration.3 For practical reasons, volunteers in this study were asked to report for follow-up blood tests as soon as possible after finishing the marathon. The incidence of hyponatraemia may well have been higher if blood samples had been taken later. Development of EAH in the hours after the marathon is worthy of further investigation.
EAH is more common after exercise of more than 4 h duration: slower runners have more opportunity to consume excessive volumes of fluid.6 8 9 25 In this study, however, five of the 11 runners (45.5%) who developed hyponatraemia finished the race within 4 h, and, contrary to other studies,8 the current study did not find a correlation between finishing times and [Na+]. Closer analysis reveals that three of these five consumed at least 600 ml in the time between finishing and their review, thereby increasing their total fluid intake by 25–30% after stopping exercise. These two observations enhance the case for the presence of an additional factor, such as altered renal function persisting after the precipitating activity, in the development of EAH.
A limitation noted by other studies was a lack of baseline or premarathon [Na+].6 Without a baseline, it could be argued that development of hyponatraemia is related to low premarathon [Na+]. Although those who developed hyponatraemia did start with a lower premarathon [Na+], they were all within the normal range. Notably, however, these runners demonstrated a significantly greater fall in [Na+] than those who did not develop hyponatraemia.
The incidence of asymptomatic hyponatraemia in this study group is consistent with the experience at the Boston Marathon supporting the contention that EAH is under-recognised.6 The tipping point at which asymptomatic hyponatraemia becomes symptomatic is highly variable and therefore unpredictable. Following Almond et al, if this incidence of EAH is representative of all finishers in the London Marathon, 4152 runners are likely to have finished with asymptomatic hyponatraemia, despite the cool wet weather conditions discouraging excessive drinking. This life-threatening condition, which recently claimed the life of a healthy runner in the London Marathon,5 appears to remain a real threat despite recent EAH Consensus Statements4 10 and an Advisory Statement from the International Marathon Medical Directors Association12 on safe drinking habits during exercise. This significant incidence of asymptomatic hyponatraemia which developed in cool running conditions in a healthy running population should alert marathon medical staff and organisers to the potential for an increase in more severe hyponatraemia in warmer weather conditions which encourage excessive drinking. Runners should continue to be educated about fluid intake during exercise and the symptoms of early hyponatraemia such as weight gain.
Limitations
Logistical considerations determined that prerace weight and [Na+] were measured at registration rather than at the start; thus, we cannot ascertain the true prerace hydration status of the volunteers immediately before the race. Fluid intake in this study was self-reported. Runners often take great care over their training and race schedules; however, fluid intake was reported retrospectively and therefore must be treated as an estimate. Fortunately, weight change, a more reliable and objective measure of fluid balance,3 produced similar results.
Twenty-three volunteers (20.1%) did not return for a blood test after the marathon. There could be many reasons for this, but we do know this group finished the marathon later than those who did return. If prolonged duration of exercise is a recognised risk factor and had this group returned for blood tests, might the incidence of EAH have been even higher?
Conclusion
A significant proportion (12.5%) of healthy volunteers developed asymptomatic hyponatraemia running a marathon in cool conditions. On average, these runners consumed more fluid and gained more weight than did non-hyponatraemic runners, although fluid intake was not related to weight gain in this study, and four of the 11 hyponatraemic runners lost weight over the course of the marathon. Female gender and slow race pace were not associated with the development of EAH in this study. Five of the 11 runners who developed hyponatraemia finished the race within 4 h. Three of these five consumed up to 30% of their total fluid intake after they had finished the marathon. These observations enhance the case for the presence of an additional factor in the development of EAH, such as inappropriate ADH release during exercise causing altered renal function and which may persist after cessation of the precipitating activity.
What is already known on this topic
Exercise-associated hyponatraemia (EAH) is a potentially fatal cause of collapse in endurance exercise. Risk factors include excessive fluid consumption in excess of total body fluid losses, altered renal function, longer race duration, female gender and smaller size. Five marathon runners are known to have died from EAH in recent years.
What this study adds
A significant proportion (12.5%) of healthy volunteers developed asymptomatic hyponatraemia running a marathon in cool conditions. Although they consumed more fluid and gained more weight than non-hyponatraemic runners, fluid intake was not related to weight gain; several hyponatraemic runners lost weight. SIADH during exercise may potentially account for this phenomenon.
Acknowledgments
The authors would like to thank all the runners who kindly volunteered to help us in this study. Thanks must also go to Abbott Point of Care, who kindly supplied the i-STAT blood analysers and cartridges for this study and continue to support the London Marathon medical team.
References
Footnotes
-
Funding Abbott Point of Care supplied the i-STAT blood analysers and cartridges for this study.
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the East London and the City Research Ethics Committee 3.
-
Patient consent Obtained.