Article Text

Abstract
Background Anterior cruciate ligament (ACL) injury prevention programmes have shown mixed results, which may be due to differing emphasis on training components. The purpose of this study was to (1) quantify the overall and relative duration of each training component encompassed within these programmes and (2) examine the effect of these durations on ACL injury rates.
Methods A systematic review was completed and meta-analyses performed on eligible studies to produce a pooled OR estimate of the effectiveness of these programmes. Meta-regression was used to detect any relationship that programme duration and the duration of individual training components had on ACL injury rates.
Results 13 studies were included for review. Results of the meta-analyses revealed a significant reduction of injuries after preventative training programmes for all ACL injuries (pooled OR estimate of 0.612, 95% CI 0.44 to 0.85; p=0.004) and for non-contact ACL injuries (OR 0.351, 95% CI 0.23 to 0.54; p<0.001). Results of meta-regression analysis revealed that a greater duration of balance training was associated with a higher injury risk for ACL injury (p=0.04), while greater durations of static stretching was associated with a lower injury risk for non-contact ACL injuries (p=0.04).
Conclusions While ACL prevention programmes are successful in reducing the risk of ACL injury, the ideal combination and emphasis of training components within these programmes remains unclear. Evidence indicates that greater emphases on balance training and static stretching may be associated with an increase and decrease in injury risk, respectively.
- ACL
- Injury Prevention
- Knee injuries
- Sporting injuries
Statistics from Altmetric.com
Introduction
Partaking in recreational or competitive sports places participants at risk for athletic injuries, including ruptures of the anterior cruciate ligament (ACL). Up to 0.05% of the US population sustain ACL injuries each year, with the incidence being higher (3.67%) in those who participate in multidirectional sports such as basketball and soccer.1 Among these injuries, 72% occur in non-contact situations.1 In 1999, the cost associated with the subsequent treatment, diagnosis, surgery and rehabilitation was estimated at close to US$12 000 per individual, and is assuredly higher at the present time.2 These costs did not account for time lost from activity (sport or work), psychological effects or long-term sequelae related to further joint pathology such as osteoarthritis, which has been found in 40–80% of individuals who suffer an ACL injury.3–6 Thus, preventing the initial trauma is considered the most efficient way to reduce the physical, psychological and financial costs associated with this devastating injury.
Multiple ACL prevention programmes have been developed with the goal of addressing modifiable risk factors for ACL injury that include abnormal biomechanical movement patterns7 and neuromuscular alterations.7 ,8 While a majority of these programmes target ACL injuries specifically, others attempt to globally reduce the incidence of lower extremity injuries. Women are the primary focus of these programmes, based on their injury rates being four times higher than their male counterparts.9 ACL injury prevention programmes vary widely in their framework and implementation methods, with a majority reporting successful reductions in injury rates10–19 while others have had less desirable outcomes.20–22 One reason for the range of effectiveness may be due to the fact that the duration and time span over which these programmes are administered vary considerably. Further, emphasis of various training components, including strength, agility, balance and plyometric training, vary widely in their prescribed duration and intensity.
To date, limited research has examined the volume and emphasis of the various training components to determine which components are most effective in reducing injury rates. Yoo et al23 reported that programmes utilising strength and plyometric techniques were the most successful in reducing injuries, while programmes emphasising balance activities were unsuccessful. However, the authors did not state their methods for defining the individual components found in each programme and training volume was not accounted for in the analysis. In a recent meta-analysis, intervention effectiveness was reported to improve if athletes engaged in preventative training greater than 0.75 h/week, but did not delineate the emphasis of training components.24
To understand the volume of training requires knowledge of both the intensity as well as duration of each component.25 Unfortunately, the intensity of exercise is rarely reported in these studies. As such, an initial understanding of the type and duration of training components that yields the greatest reduction in injury risk may lend important insights into the relative emphasis of programme components, and the future development of prevention programmes. Thus, the primary purpose of this systematic review was to quantify the training duration of previously published prevention programmes, identify and quantify the duration of each individual training component, and analyse the efficacy of the various components in reducing ACL injury rates in female athletes. We focused specifically on female athletes, since the majority of programmes to date have targeted this population.
Methods
Study design
A systematic review was performed in accordance with the PRISMA Statement for Reporting Systematic Reviews.26 No protocol exists for this study, which was exempt from review by the University's Institutional Review Board for the protection of the participants. No external funding supported this review.
Search strategy
An electronic search was performed on 31 July 2012 of the PubMed, MEDLINE, CINAHL, SPORTDiscus and the Cochrane Central Register of Controlled Trials databases. The search terms included: knee injur*(tiab), ACL injur*(tiab), and anterior cruciate ligament injur*(tiab) combined with the terms intervent*(tiab) and prevent*(tiab). Filters were utilised to access only those studies that investigated participants and were reported in English. No limitations were imposed on the date of publication.
Eligibility criteria
Studies were included if they met the following criteria: (1) the study design was a randomised controlled, or prospective cohort, trial, (2) the study reported ACL injury incidence, or made it possible to calculate these values for female athletes in both the intervention as well as control groups with the data provided, (3) the study published the specific exercises or components used in the intervention programme and (4) the study reported the duration of each individual training session. Authors of the studies that met some, but not all, of the criteria were contacted for further information and were included if the above details could be obtained.
Study selection
Two authors (JBT and JPW) independently reviewed the studies found during the database search. Articles were screened for eligibility based on review of the title and abstract only. If necessary, any disagreements were resolved by consensus with the third author (SJS). The full-text of included articles were then accessed and again analysed for eligibility. The same process was used to create consensus on articles to be included in the analysis after full-text review. Inter-rater agreement was calculated for both screening procedures using a Fleiss κ with values interpreted as <0 poor agreement, 0.01–0.20 slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement and 0.81–1.0 almost perfect agreement.27 Cited references of relevant articles were scanned and hand-searched for other possible inclusions to this study.
Quality assessment
Included studies were analysed using the Physiotherapy Evidence Database (PEDro) scale, which was developed from the Delphi list and used for quality assessment of the methodology of randomised clinical trials (http://www.pedro.org.au/english/downloads/pedro-scale/). The scale exhibits moderate reliability (intraclass correlation=0.56, 95% CI 0.57 to 0.76) and helps to determine internal validity and identify studies with interpretable results.28 Two reviewers (JBT and JPW) independently assessed each study and where consensus was not reached the third reviewer (SJS) was consulted.
Data collection and analysis
The data extracted from each study included the training season, age of participants, presence or absence of technique-based feedback to athletes, minutes per training session, total number of training sessions, athletic exposures (AEs), player seasons (PSs), the duration and variety of training exercises used in the prevention programmes, and incidence rates of ACL injuries and non-contact ACL injuries. Training session times that were reported by each study were modified to better estimate actual training time by subtracting any reported rest periods, time for upper extremity exercises or simple warm-up jogging that did not focus on technique. If a range of time was given, the midpoint of the range was used for analysis. The total number of training sessions was calculated based on the frequency and duration of the intervention programme. In studies where no exact duration was stated, the length of the training was estimated based on reported calendar dates or the length of a typical season documented in other published studies. Total training time (TTT) was then found by multiplying the total number of training sessions by the number of minutes per training session and was reported in hours.
Each ACL prevention programme was analysed independently and the individual training activities were categorised into one of five components. Strength training was defined as an activity used to improve muscular strength through the use of resistance that included the use of bodyweight, free weights or strength machines. Activities were characterised as explosive if they utilised powerful movements, such as plyometric jumping or bounding. Balance exercises encompassed single-legged or double-legged stance activities that were designed to improve proprioceptive awareness. Agility exercises were defined as activities promoting the ability to move and change direction quickly and effectively, while under control. Finally, the stretching category included all static stretching activities.
After the specific activities were categorised in to one of the five components, training durations were then calculated. In this review, duration was defined as the time spent performing each exercise. The time spent in training in each component was independently estimated by two reviewers (JBT and JPW) based on the reported measures (time, reps, sets and percentage of programme). For example, the programme described by Walden et al18 incorporates six exercises (one-legged knee squat, pelvic lift, two-legged knee squat, bench, lunge and jump/landing) that were measured and reported in time or repetitions. The jump/landing was classified as a balance activity due to its focus on proprioceptive awareness, while the other five were considered to be strengthening exercises. The authors estimated that these six exercises took similar amounts of time to perform. Since each programme session lasted an average of 15 min, 5/6 of the session duration was estimated for strengthening (12.4 min) and 1/6 for balance training (2.6 min). The reviewers then compared their results and a consensus was reached if the estimates were within 10%. If needed, the third reviewer was consulted (SJS), and in cases where no consensus was reached, the authors of references 20 and 29 were contacted.20 ,29 The percentage time of each component in the programme was calculated by dividing the component time per session by the total time per session. TTT for each component was then computed by multiplying the appropriate percentage by the TTT to obtain the estimated total number of hours spent on each component for each intervention programme.
Statistical analysis
Study results were analysed using Comprehensive Meta Analysis, V.2.0 (Biostat, Englewood, New Jersey, USA) and SPSS, V.20 (IBM Corp, Armonk, New York, USA, 2011). In order to standardise injury rates for meta-analysis, and to include all studies, ORs were calculated in two forms: (1) based on AEs and (2) based on athlete PSs. AEs, which might be more correctly termed ‘athlete participation’,30 were reported as AE hours in some studies. AE hours were transformed to AEs based on the calculation of two exposure hours equals 1 AE. AE is the preferred reporting unit and this conversion has been used and calculated in other meta-analyses.30–32 PSs were determined by multiplying the number of athletes by the number of seasons in which injuries were tracked.
ORs were chosen as the metric to compute effect sizes because of its statistical properties that best match with meta-analysis procedures.33 Seven studies dichotomised ACL injuries into contact and non-contact mechanisms,10–12 ,15–18 three reported only non-contact injuries,13 ,14 ,20 and three reported either contact and non-contact together or did not specify the nature of injury.21 ,22 ,29 As such, ORs were computed and reported with 95% CI for (1) all ACL injuries in relation to AEs (either unspecified injuries or contact plus non-contact injuries), (2) all ACL injuries in relation to PSs (either unspecified injuries or contact plus non-contact injuries), (3) all non-contact injuries in relation to AEs and (4) all non-contact injuries in relation to PSs.
Inverse variance meta-analyses, using a random effects model, were performed in order to compute the overall effect estimates of the four groups previously defined by OR calculations. A random effects model is used in cases where the true effect size may vary between studies and incorporates both between as well as within study heterogeneity into summary estimates.33 The 95% CIs for the mean of the population of true ORs were calculated, with p<0.05, indicating that the true OR was different from one. Both a χ2 statistic with corresponding p value, as well as an I2 statistic were calculated and used to describe the total variation across studies due to heterogeneity as opposed to random chance. Values of I2 of 25% are considered low, 50% are considered moderate and 75% are considered high heterogeneity.34 Publication bias was assessed visually with funnel plots and quantified using Rosenthal's Fail-safe N, which determines how many potential missing studies would have to be included in order to make the overall estimate non-significant.35 ,36
Meta-regression was used to analyse the extent to which total and individual programme components predicted the odds of becoming injured. General aspects of the programmes, including TTT and session duration were investigated, as were more specific variables of the training components, including their percentage of emphasis, session duration and total duration. Further, a subgroup analysis was performed to identify the effect of the presence or absence of technique feedback on injury risk. Owing to the low number of studies and power in these analyses, principal components analysis and meta-regression with multiple variables were not performed.
Results
Search results
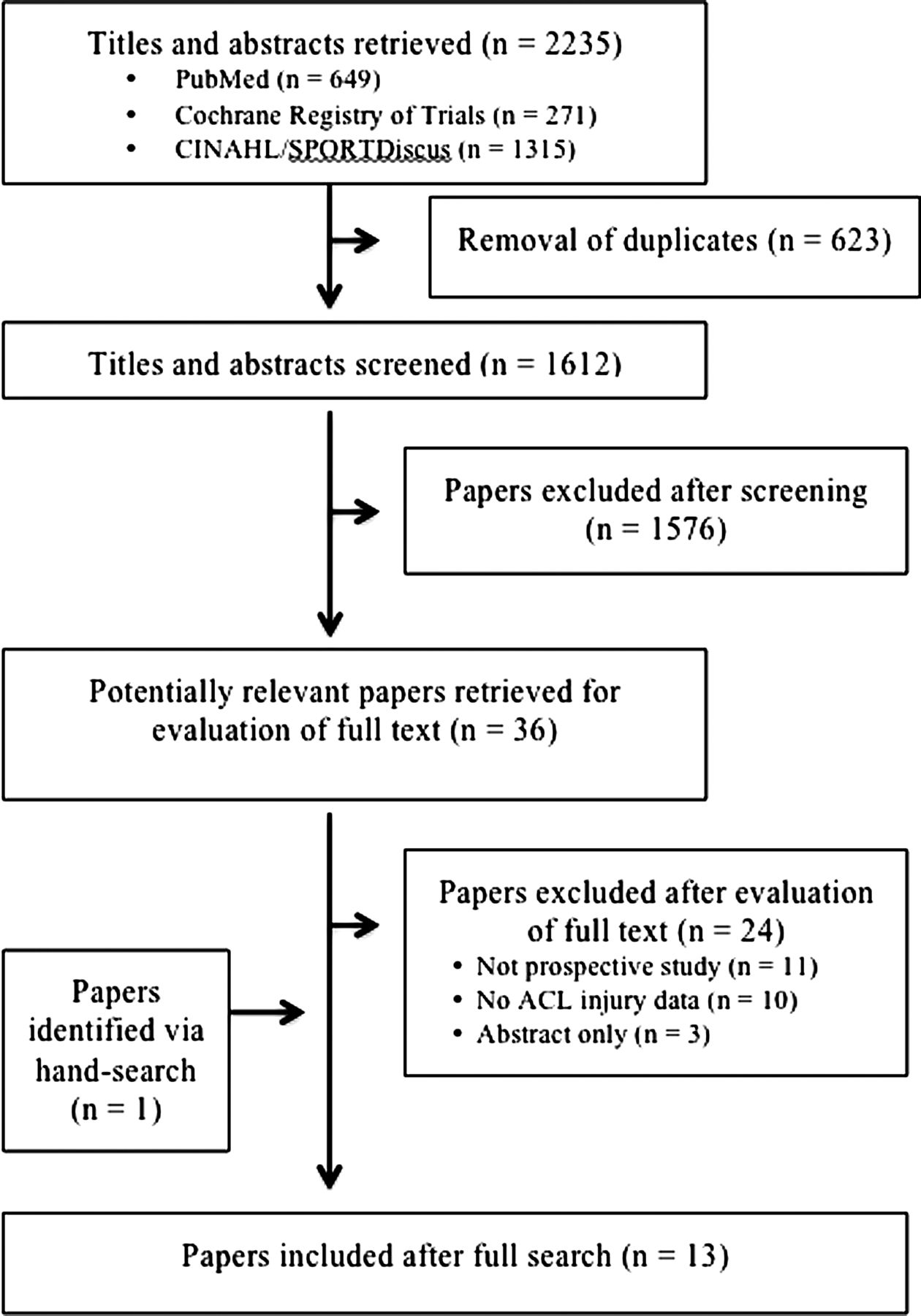
The electronic database search of PubMed, MEDLINE, CINAHL, SPORTDiscus and the Cochrane Register of Controlled Trials yielded 2262 results. A flow diagram of the selection process is in figure 1. After duplicates were removed, 1612 studies remained. Of these, 1576 were excluded based on title and abstract review, leaving 36 for full text review (κ agreement 0.78, 95% CI 0.65 to 0.89). The full text of the remaining studies were retrieved and reviewed for eligibility. Twenty-four of these studies were excluded because they either did not contain specific ACL incidence data, or did not document their intervention programme or were not a prospective study design (κ agreement 0.88, 95% CI 0.71 to 1.0). An additional hand search revealed one study that met the inclusion criteria of this systematic review.22 Thirteen total studies were included in the final analysis.10–18 ,20–22 ,29 Characteristics of these studies are in table 1.
Characteristics of studies included for review

Flow diagram of retrieved, screened and included studies.
Quality assessment
Results of quality assessment using the PEDro scale showed a wide range of scores (3–8) with an average score of 4.5 (table 1). Not all studies that were included in this review were randomised controlled designs and subsequently had lower quality scores. Further, no studies were able to blind the participants or interventionists, which further reduced scores.
Overall intervention effects
Meta-analysis results revealed a statistically significant reduction in all ACL injuries (OR 0.61, 95% CI 0.44 to 0.85) and non-contact ACL injuries (OR 0.35, 95% CI 0.23 to 0.54) when incidence was expressed relative to PSs (figure 2A,B). Similar effect estimates were obtained when incidence was expressed relative to AEs for all ACL injuries (OR 0.64, 95% CI 0.42 to 0.99 and non-contact ACL injuries (OR 0.38, 95% CI 0.22 to 0.64). Because of this, and because more studies were included when injury risk was expressed relative to PSs, only the injury risk data based on PSs were examined in the meta-regression and subgroup analyses.

Meta-analysis forest plot of (A) total anterior cruciate ligament (ACL) injuries and (B) non-contact ACL injuries in relation to player seasons. Favours A indicates reduction in injury risk and favours B indicates heightened injury risk.
Heterogeneity
The χ2 statistic for all meta-analyses was not statistically significant and I2 calculations ranged from 0% to 28%, which is considered to have a low effect from heterogeneity. Since these values were found to be non-significant, further statistical analysis to explain the heterogeneity was not pursued.
Publication bias
Funnel plots depicted asymmetry in the lower right region, indicating that results may have some bias due to the lack of inclusion of small studies with insignificant findings that have been unpublished or not found by our search strategies. However, two separate Classic Fail-safe N tests show that the number of studies needed to be included to change the results of the meta-analyses to non-significant were 55 for the non-contact ACL injury analysis and 12 for the unspecified/total ACL injury analysis.
Total training duration
Total programme training duration can be found in table 1. The frequency of training sessions ranged from once per week to daily; in some cases, training frequency was reduced during the transition of the programme from a training phase to a maintenance phase. The duration of a single training session ranged from 10 to 44.7 min, while the total number of training sessions ranged from 10 to 108. Taken together, this represents a wide variety of TTTs ranging from 9.8 to 22.5 h. Results from the meta-regression analysis revealed no statistically significant effect of TTT or session duration on ACL injury rates (table 2).
Results of meta-regression with significance set at p<0.05 level
Training components
Table 3 reports the results for the duration of each programme component in terms of per cent emphasis, time per training session and total time. Strength, explosive and agility training were each represented in 69% of the programmes, where balance training and static stretching were represented in 54% and 23% of programmes, respectively. The training emphasis (defined as the component with the highest percentage of total duration) varied considerably between programmes, with most programmes having the greatest emphasis on balance and agility training. Meta-regression resulted in two statistically significant findings (table 2). Results show that ACL injury risk increases as the total duration of balance training increases (p=0.04; figure 3), whereas injury risk decreases with a greater emphasis and longer duration of prescribed static stretching (p=0.04).
Programme components of ACL prevention programmes with intended training time

{kind=link}
{kind=link}
{kind=link}
Meta-regression results of total balance training duration. Each circle represents an included study with the size consistent with the weight assigned during meta-analysis. A regression line is seen, indicating a less protective OR as total balance duration increases.
Technique feedback
For non-contact ACL injuries, a subgroup analysis demonstrated that there was no statistical difference between those that received feedback and those that did not (p=0.74). The same subgroup analysis performed in the total ACL injury group also yielded non-statistically significant results (p=0.13).
Discussion
Results of these meta-analyses indicate that injury prevention programmes can be successful in reducing ACL injuries in female athletes. These results are consistent with prior findings23 ,24 ,32 ,37 and suggest that continued research efforts aimed at improving the efficiency and efficacy of these preventative training programmes are warranted. Moreover, results suggest that these programmes may have a stronger effect on the reduction of injury risk for non-contact ACL injuries compared with those resulting from a contact mechanism. Though further meta-regression analyses provided no statistically significant findings on the frequency or durations of these programmes, trends were found with respect to individual training programme components that may help the development of future preventative programmes.
As described in this review, intervention programmes vary widely in their design and implementation. However, meta-regression results did not reveal any clear trend that allows for recommendations of duration parameters for training components of future intervention designs. The lack of significance may be due to a lack of power in the statistical analysis from the small sample size or high variability of included studies. Prospective injury prevention studies are challenging because of the resources that are needed. Only 13 studies on ACL injury prevention programmes that met our inclusion criteria have been previously published. Further, variability in the results may have stemmed from the variety of prevention programme designs or the diversity of sports, ages and athletes targeted in these studies. Thus, future studies of ACL injury prevention programmes will help to improve statistical power and hopefully provide more convincing evidence to help shape future prevention efforts.
While specific duration and emphasis recommendations cannot be made as a result of these analyses, the overarching theme is that some form of prevention training is better than nothing; however, the composition and duration of the optimal prevention programme is still unknown. Larger amounts of balance training were found to be unsuccessful in reducing ACL injury rates and statistical tests showed that increasing the total duration of balance training increased the OR of injury (p=0.04). Yoo et al23 found comparable results in regard to balance training. In their subgroup analysis, the inclusion of balance training yielded an OR that was not statistically significant (OR 0.63, 95% CI 0.37 to 1.09), while programmes without balance training showed a statistically significant OR lowering injury risk (OR 0.27, 95% CI 0.14 to 0.49). Similarly, Sadoghi et al37 found no evidence of effectiveness from the use of a balance board during prevention programmes (p=0.712). However, these findings conflict with previous research that shows positive outcomes on at-risk lower extremity mechanics as a result of balance and proprioceptive training.38 After closer investigation of the balance training protocol used in the study by Myer et al38 appreciably higher durations and intensities were used when compared with balance training components of ACL prevention programmes, suggesting that for balance training to be more efficacious, prevention programmes may need to intensify their balance training prescription.
Further, time spent in balance training may have limited the opportunity for clinicians or teammates to provide valuable feedback in regards to movement patterns and neuromuscular control during more dynamic functional activities. Various types of feedback, including visual and verbal, have been shown to reduce abnormal biomechanics associated with ACL injury risk.39–41 However, results of our subgroup analysis show no significant effect of the presence of technique training or feedback on non-contact (p=0.74) or total (p=0.13) ACL injury risk. The type and amount of feedback varied widely between the programmes included in this review. Some programmes predominantly utilised skilled sports medicine clinicians to provide instruction,10 ,11 ,17 while others used coaches or teammates.12 ,13 ,15 ,16 ,18 ,22 Inconsistent with our findings, other systematic reviews32 ,42 have found that feedback for technique training may be a valuable element of prevention programmes. We encourage authors to detail the amount and type of feedback in future studies so that their potential effects on injury risk reduction can be better elucidated.
Though static stretching has been a controversial topic in regard to injury prevention,43 meta-regression analysis shows that static stretching may have a positive impact on reducing injury rates when performed in an ACL prevention programme. Previous studies have found that static stretching has no overall impact on preventing general musculoskeletal athletic injuries, but may have some relationship with reducing ligamentous injuries.43 ,44 Static stretching may provide a means for ACL injury reduction by improving muscle imbalance or beneficially modifying the structural properties of ligamentous tissues. Cautious interpretation of these meta-regression findings is warranted, as only three of the analysed studies included static stretching in their prevention programmes. Future studies comparing static and dynamic flexibility programmes may be warranted to determine whether the benefits are derived from improved joint range of motion and flexibility or if the technique used to obtain these effects varies based on the implementation method. Any dynamic flexibility components in these programmes were captured as agility exercises based on their ability to promote controlled change of directions.
Other findings, while not statistically significant, are worth noting as they may help guide further research and development of future programmes. Increasing strength training emphasis (p=0.15) and duration (p=0.18) suggest this component may also prove useful in reducing total ACL injury rates. The purpose of including strength training as a component in these programmes is based on the premise that women lack adequate strength to control the alignment of the lower extremity during sport-specific activities. However, after careful review of these prevention programmes, it became apparent that common strength training guidelines, which call for progressive overload, were often lacking in these programmes. As such, the outcomes of these strengthening components may have been limited to more neural adaptations rather than physiological changes in muscle characteristics.25 Given the results of this meta-regression, future research is warranted to examine whether more aggressive or longer term strength training exercises would further impact injury risk reduction.
Increasing the emphasis (p=0.09) and duration (p=0.10) of agility training also showed evidence that this type of training may be beneficial in reducing non-contact ACL injury rates. A 6-week agility training protocol has been shown to improve medial hamstring activation patterns in side-step pivot manoeuvres, which may reduce ACL injury risk.45 Timing of the agility training intervention may be important as lower extremity mechanics in landing and cutting tasks are negatively altered after a fatigue-producing agility training programme.46 More research on the effects of agility training on ACL injury incidence may provide stronger evidence to support these claims.
In addition to strength and agility training, plyometric or explosive training was the most commonly used training component in the ACL prevention programmes included in this review. Though the demands and intended outcomes of these exercises are more likely to resemble sport-specific demands, evidence to support the superiority of these exercises in reducing injury risk was insufficient. This was surprising, considering the positive effects that this type of training can have on altered lower extremity mechanics.47–50 However, the extent to which effectively modifying at-risk biomechanics is able to reduce ACL injuries has not yet been determined. Moreover, the principles that govern programme implementation may also deserve further attention. For example, many of the preventative programmes were administered to young athletes without also including a foundational strength base. This strength foundation is considered to be critical before progressing to more explosive activities25 and may represent an important component to include for maximising effectiveness.
Limitations
This systematic review and meta-analysis was subject to limitations based on the quantity and quality of previously published programmes and the variety of reporting mechanisms of each prevention programme. Calculations and analyses were based on the prescribed prevention programme, as opposed to what the participants actually performed. With compliance rates as low as 26%32 the prescribed versus actual volumes may be very different and could have notably influenced the results. Low compliance leads to lower amounts of training volume, which may influence a programme's effectiveness. Another limitation of this analysis involves the interpretation of training duration. Studies included in this review reported training duration in a variety of units (ie, time and repetitions). Time was the most consistent measurement unit and was therefore used as the definition of training duration in this review. While we fully acknowledge that training volume may be a more practical measure based on the inclusion of intensity in its definition, there was insufficient information reported in these studies to account for intensity in volume calculations. Quantifying the intensity of these programmes may be a critical piece in understanding the relative contributions of each component to injury-risk reduction and what level of stimulus is needed to affect a positive change, and is therefore an important direction of future research and exercise prescription. We strongly encourage future publications to be as explicit as possible in the prescription of their prevention programme relative to intensity, duration and frequency in order to better understand the relative benefit of each component.
Further, we placed each exercise in only one of five categories, though some complex exercises may serve multiple purposes. The optimal prevention strategy may very well be a comprehensive approach, incorporating multiple training components combined into one programme. Because of the small number of studies that were included in this analysis, and therefore low statistical power, training components could not be grouped together to conduct a multivariate statistical analysis. As additional studies are published, interactions between these components may be better delineated and more concrete recommendations for preventative training can be established. On the basis of this review, we recommend that future studies carefully consider and clearly report training methodology (duration, intensity and progression) consistent with current evidence-based strength and conditioning guidelines.
Conclusion
While ACL prevention programmes are effective in reducing the risk of injury in female athletes, the ideal composition of these programmes remains elusive.
Consistent with previous analyses, the effectiveness of ACL prevention programmes may improve as balance training is de-emphasised and static stretching is emphasised. However, given the small number of studies, and the lack of detail regarding the intensity, etc, of various components, considerably more work is needed to determine which combination of programme components, and the duration and intensity at which they are delivered are most effective at reducing injury risk. Further research will help shape future prevention efforts, as more information regarding volume and training emphasis is uncovered.
References
Footnotes
-
Contributors JBT participated in study design, electronic and hand searches, study selection, quality assessment, data extraction, and drafted and revised the manuscript. JPW participated in electronic and hand searches, data collection and drafted and revised the manuscript. SJR helped in study design, statistical analysis, and drafted and revised the manuscript. SJS participated in study design, study selection, data collection, and drafted and revised the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.