Article Text

Abstract
Objectives: Inter-individual variations in sea level performance after altitude training have been attributed, at least in part, to an inter-individual variability in hypoxia induced erythropoiesis. The aim of the present study was to examine whether the variability in the increase in total haemoglobin mass after training at moderate altitude could be predicted by the erythropoietin response after 4 h exposure to normobaric hypoxia at an ambient Po2 corresponding to the training altitude.
Methods: Erythropoietin levels were measured in 16 elite junior swimmers before and after 4 h exposure to normobaric hypoxia (Fio2 0.15, ∼2500 m) as well as repeatedly during 3 week altitude training (2100–2300 m). Before and after the altitude training, total haemoglobin mass (CO rebreathing) and performance in a stepwise increasing swimming test were determined.
Results: The erythropoietin increase (10–185%) after 4 h exposure to normobaric hypoxia showed considerable inter-individual variation and was significantly (p<0.001) correlated with the acute erythropoietin increase during altitude training but not with the change in total haemoglobin mass (significant increase of ∼6% on average). The change in sea level performance after altitude training was not related to the change in total haemoglobin mass.
Conclusions: The results of the present prospective study confirmed the wide inter-individual variability in erythropoietic response to altitude training in elite athletes. However, their erythropoietin response to acute altitude exposure might not identify those athletes who respond to altitude training with an increase in total haemoglobin mass.
- EPO, erythropoietin
- Hb, haemoglobin concentration
- Hct, haematocrit
- MCV, mean corpuscular erythrocyte volume
- RBV, red blood cell volume
- THM, total haemoglobin mass
- athletes
- erythropoietin
- hypoxia
- total haemoglobin mass
Statistics from Altmetric.com
- EPO, erythropoietin
- Hb, haemoglobin concentration
- Hct, haematocrit
- MCV, mean corpuscular erythrocyte volume
- RBV, red blood cell volume
- THM, total haemoglobin mass
There is remarkable inter-individual variability in improvement in sea level performance after training at moderate altitudes of 2000–2500 m. Chapman et al1 presumed that this variability might largely be explained by individual variation in the erythropoietic response to altitude. In a retrospective analysis of a controlled study, they showed that college runners who had responded to altitude training with significant improvement in a 5000 m run at sea level, experienced a distinctly increased erythropoiesis during 4 weeks of altitude raining. Compared to other college runners who had not improved after altitude training, these athletes displayed a larger acute increase in erythropoietin (EPO), still had significantly elevated EPO levels after 14 days of altitude training, and experienced significant augmentation of total red cell volume after return to sea level. It was concluded that a large acute increase in EPO, sufficient to cause an increase total red cell volume, is an important determinant for improvement in sea level performance after altitude training.
Great inter-individual variability has been found in the erythropoietic response to high and moderate altitudes.2,3 During a 3 week sojourn at high altitude (6542 m) the increase in EPO and the subsequent haemoglobin response to EPO were both found to vary considerably.2 More recently, Ge et al3 reported a marked individual variability in EPO increase after 6 and 24 h exposure to hypobaric hypoxia equivalent to altitudes of 1780–2800 m. Furthermore, they concluded that altitudes ⩾2100–2500 m might be a threshold for the induction of increased erythropoiesis in most athletes.
In the present prospective study, we investigated whether the EPO response to acute exposure to normobaric hypoxia allows the identification of athletes who will respond to altitude training with a distinct increase in EPO concentration and a subsequent augmentation of haemoglobin mass. We hypothesised that the EPO response after 4 h exposure to normobaric hypoxia at an ambient Po2 similar to the training altitude is indicative for the extent of acute EPO increase during a training camp at moderate altitude and that a large EPO increase after acute hypoxic exposure is associated with a large increase in total haemoglobin mass after training at moderate altitude and vice versa.
To test our hypotheses, EPO was measured in 16 elite junior swimmers (nine males and seven females) prior to and after 4 h exposure to normobaric hypoxia (Fio2 0.15) as well as repeatedly during living and training at an altitude of 2100–2300 m. Furthermore, total haemoglobin mass was determined with CO rebreathing before and after altitude training as was performance in an incremental swimming test.
METHODS
Subjects
A total of 20 elite junior swimmers (11 females and nine males) volunteered for the study. Four swimmers (two females and two males) suffered from infectious diseases during altitude training or the testing period and had to reduce or even stop their training for several days. Their data were not included. The descriptive data of the remaining 16 swimmers were: 16.4 (standard deviation (SD) 1.4) years, 180.3 (8.5) cm, 70.4 (9.5) kg; females (n = 9): 15.4 (0.9) years, 174.0 (4.7) cm, 63.7 (4.3) kg; males (n = 7): 17.7 (0.8) years, 188.3 (4.2) cm, 79.0 (6.7) kg. All swimmers had been intensively training for at least 5 years and most of them had successfully participated in European or World Championships or in European Junior Championships. Written informed consent was obtained in each case and also from their parents for those athletes younger than 18 years. The study was approved by the Ethics Committee of the Medical Faculty of the University of Heidelberg, Germany. Six of the female and three of the male swimmers had already participated in between one and four training camps at moderate altitudes of 1800–2300 m; none had been to altitude for at least 6 months prior to the study.
None of the swimmers was anaemic (females: haemoglobin concentration (Hb) >11.7 g dl−1, males Hb >13.5 g dl−1, normal values for haematocrit (Hct) and mean corpuscular erythrocyte volume (MCV)). Ferritin values (females: 33.2 (SD 13.6) µg l−1, males: 50.7 (27.4) µg l−1) were within normal range except for two females whose ferritin values were <25 µg l−1. They were treated with 567.7 mg ferrous-glycin-sulfate (gelatin coated capsules) equivalent to 100 mg elemental iron daily throughout the study.
Experimental protocol
Tests before altitude training
A total of 10 athletes (five females, five males) were tested 2 weeks, and six athletes (four females, two males) 1 week before travelling to the altitude training camp as follows:
-
Day 1: Health checks including blood draws (to determine Hb, Hct, and ferritin) and incremental cycle spiroergometry in normoxia.
-
Day 2: Incremental swimming test.
-
Day 3: Venous blood draws in the morning to determine baseline EPO; 4 h in normobaric hypoxia (Fio2 0.15); blood draws to determine EPO response to acute altitude exposure; and measurement of total haemoglobin mass with CO rebreathing.
Tests after altitude training
All swimmers performed the incremental swimming test and their total haemoglobin mass, Hb, and Hct were measured 10 days after return to sea level, the time when athletes and coaches consider that maximal sea level performance is achieved after altitude training.
EPO measurements during altitude training
Blood draws were conducted in the mornings of days 1, 2, 8, and 20 of altitude training. As the swimmers did not travel together and had arrived at the altitude training camp in three groups at different times of the day, the acute EPO response during altitude training was determined as the maximal individual value of measurements taken on days 1 and 2 at altitude. On average, maximal EPO increases were determined after 22.3 (SD 11.9) h at moderate altitude.
Blood analyses
Blood samples (5 ml) were drawn into an EDTA tube from an antecubital vein in the sitting position. Hb, erythrocyte count, and MCV were measured with a Coulter T 840 Counter (Coulter Electronics, Krefeld, Germany). Hct was determined with microcentrifugation. For determination of serum EPO, 7 ml of venous blood were drawn from an antecubital vein, centrifuged (3000 rpm, 10 min, 4°C) within 30 min, and stored at −20°C until measurement (Erythropoietin ELISA, IBL, Hamburg, Germany). Ferritin was measured photometrically (EIAgen Ferritin Kit, Adaltis, Freiburg, Germany) before altitude training. Each measurement was carried out in duplicate.
Measurement of total haemoglobin mass
Total haemoglobin mass was measured with carbon monoxide (CO) using a rebreathing method as described previously.4 The athlete ventilated a mixture of CO (0.85 ml CO per kg body weight) in 5 l of O2 in a closed system. If necessary, O2 was refilled. Immediately before starting the measurement, 5 ml of venous blood were drawn from an antecubital vein for determination of Hb, Hct, erythrocyte count, and MCV. The COHb fraction was measured in venous blood from an antecubital vein with an automated system (270 CO-Oxymeter, CIBA-Corning, Fernwald, Germany) before and every 2 min while ventilating this mixture until a plateau was reached, usually near 5% COHb after 10–15 min. Total haemoglobin mass (THM) was calculated as:
THM = K MCO (100/DCOHB 1.34).
Red blood cell volume (RBV) was calculated as
RBV = THM/MCHC
according to Burge et al5, where K is barometric pressure/[760 (1+(0.003669 temperature))], MCO is volume of added CO in ml, and DCOHB is the difference between basal COHb and maximal COHb multiplied by 1.34 as 1.34 ml CO bind to 1 g Hb.
Exercise testing
The incremental swimming tests consist of five steps starting at an intensity of about 80% of the personal best performance at the time of testing. Intensity is increased by 5% per step until maximal performance is reached in the last step. Step duration (100–400 m) and swim style depend on the swimmer’s specialisation. These tests were conducted in a 50 m pool and are regularly performed by elite German swimmers to monitor performance and derive training recommendations. For lactate measurement, 20 µl of capillary blood were drawn from the earlobe at the end of each step and repeatedly after the maximal step and measured using an automated system (EBIO plus, Eppendorf, Hamburg, Germany).
Normobaric hypoxia
The swimmers were exposed to normobaric hypoxia by diluting ambient air with nitrogen in a special room. The N2 enriched air supply is controlled by an O2 sensor driven inlet valve; N2 enrichment is achieved by an O2 separation system using compression (AGA, Hamburg, Germany). In the present study the ambient inspiratory oxygen fraction (Fio2) was 0.15 simulating a degree of hypoxia corresponding to an altitude of about 2500 m. Ambient O2 and CO2 were continuously monitored.
All tests in normoxia were conducted at a natural altitude of about 120 m.
Altitude training
The altitude training camp took place in Monachil (Sierra Nevada), Spain, where the swimmers lived and trained at an altitude of 2100–2300 m. The athletes performed 60–70 km of swim training per week, mainly endurance training with intensities below a lactate level of 4 mmol l−1 (55%) but with some lactate levels between 4 and 6 mmol l−1 (9%). About 30% of the training concentrated on improving swimming style. Training was supervised by experienced coaches. Lactate was measured in capillary blood during several training sessions and training intensity adjusted if necessary.
Statistics
Statistical analysis was performed with the software programs Sigmastat 2.0 and Sigmaplot 7.0 for Windows from Jandel Scientific (San Rafael, CA). Data are presented as mean (SD) values. Differences between values obtained before and after training and between measurements in normoxia and normobaric hypoxia were analysed using Student’s paired t test checking for normal distributions. For comparison of the EPO measurements over time, repeated measures ANOVA on Ranks was used followed by Dunnett’s test for multiple comparison procedure to determine the source of difference. Correlations between selected parameters were analysed by linear regression. The level of significance was set at p<0.05.
RESULTS
Erythropoietin response
EPO was significantly increased after 4 h exposure to normobaric hypoxia by 58.3% (SD 41.4%) and on days 1 and 2 of altitude training by 51.8% (45.6%) (15.2 (5.0) and 14.7 (6.0) v 10.2 (4.0) mU ml−1, respectively). On days 8 and 20 of altitude training, EPO was not significantly different from the values measured in normoxia (sea level baseline). There was a large individual variation in the EPO response after 4 h in normobaric hypoxia as well as during altitude training as shown in fig 1A. The EPO increase after 4 h exposure to normobaric hypoxia was significantly correlated with the acute EPO increase during altitude training (fig 1B).

(A) Changes in EPO after 4 h exposure to normobaric hypoxia (Fio2 0.15) and during altitude training. The data are presented as per cent differences to sea level baseline values. Individual values and mean and standard deviation values are shown. *Indicates significantly different from sea level baseline. (B) Correlation between the EPO response to 4 h exposure to normobaric hypoxia (Fio2 0.15) and the acute EPO response during training at an altitude of 2100–2300 m. The data are presented as per cent sea level baseline values.
Total haemoglobin mass and haemoglobin
The changes in total haemoglobin mass showed a wide inter-individual variability as can be seen in fig 2A. After 3 weeks of altitude training, total haemoglobin mass was significantly increased by 6% on average, from 855 (SD 185) to 909 (196) g (12.1 (1.6) to 12.9 (1.8) g kg−1 body weight; RBV: 35.1 (4.2) to 36.9 (5.1) ml kg−1 body weight). However, there were no significant correlations between the acute EPO increase at altitude and the change in total haemoglobin mass (fig 2B) or between EPO on days 8 (r = −0.08, p = 0.78) and 20 (r = 0.04, p = 0.89) of altitude training and changes in total haemoglobin mass (both parameters expressed as per cent sea level baseline).

(A) Changes in THM after altitude training. The data are presented as per cent sea level baseline values. Individual values and mean and standard deviation values are shown. *Indicates significantly different from sea level baseline (p<0.001). (B) Correlation between the acute EPO response during altitude training and the change in THM after altitude training. The data are presented as per cent differences from sea level baseline values.
Neither Hb nor Hct had changed significantly after altitude training (females: Hb 13.3 (SD 0.6) g dl−1 after training v 13.0 (0.8) g dl−1 before training, Hct 39.9% (2.2%) v 39.5% (2.5%); males: Hb 14.8 (0.3) g dl−1v 15.1 (0.4) g dl−1, Hct 44.1% (1.2%) v 45.4% (1.4%).
Performance in the incremental swimming test
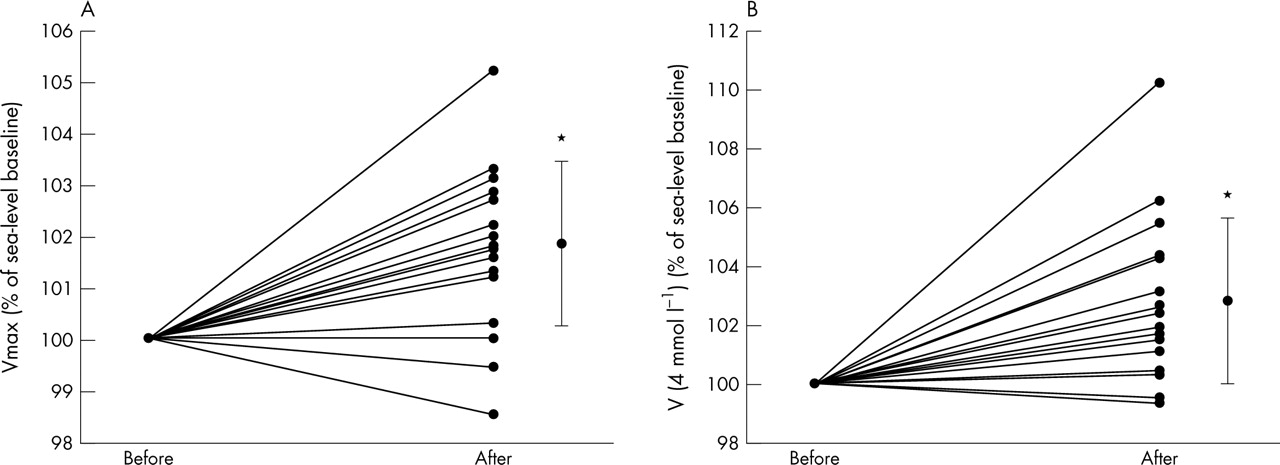
Considerable individual variation was found in the improvement in maximal and submaximal performance as demonstrated in fig 3A and B. Maximal performance and performance at 4 mmol l−1 lactate concentration were significantly increased by about 2–3% after altitude training. Maximal lactate concentration remained unchanged (10.3 (SD 3.0) mmol l−1 after v 9.6 (3.0) mmol l−1 before altitude training). There were no significant correlations between the change in total haemoglobin mass and the change in maximal performance nor between the change in total haemoglobin mass and the change in performance at a 4 mmol l−1 lactate concentration.

{kind=link}
{kind=link}
{kind=link}
Changes in maximal performance and in performance at a 4 mmol l−1 lactate concentration in an incremental swimming test. The data are presented as per cent sea level baseline values. Individual values and mean values and standard deviation are shown. *Indicates significantly different from sea level baseline (p<0.001). V, velocity.
DISCUSSION
The main new observation of the present study was a significant correlation between the EPO increase that occurred during the first days of living and training at moderate altitude and the EPO response after 4 h exposure to normobaric hypoxia at an ambient Po2 similar to the training altitude. However, the increase in total haemoglobin mass after altitude training was correlated neither with the acute EPO increase nor with the EPO values measured in the middle and at the end of 3 week altitude training. These results indicate that athletes who respond to training at moderate altitude with a large acute EPO increase might be identified with the help of short exposure to equivalent normobaric hypoxia; however, apparently, high acute EPO increases upon altitude exposure did not always yield large increases in total haemoglobin mass after living and training at moderate altitude.
Elite athletes from various sports train at moderate altitude (1700–3000 m) in an attempt to improve their aerobic capacity because of a hypoxia induced increase in total haemoglobin mass.6,7 Results of studies on the effects either of living and training at moderate altitude or of living at moderate altitude and training at low altitude on total haemoglobin mass (red cell volume) and sea level performance are controversial.8,9–16 In most of the studies with elite athletes, total haemoglobin mass was not significantly increased after living and training at moderate altitude.10–12,15,16
Several explanations for the unexpected lack of increase in total haemoglobin mass after altitude training have been suggested: insufficient iron stores could have prevented efficient erythropoiesis17; altitudes <2100–2500 m seem to be below the threshold for efficient hypoxia induced EPO release18; polycythaemic hypervolaemia caused by years of endurance training in elite athletes might have reached a maximum with no potential for a further increase12 and substantial individual variation in the erythropoietic response to altitude might have been responsible for the lack of significant changes and might also explain the considerable inter-individual variation in sea level performance after altitude training.1 The present study focused on the question of whether the EPO response to acute normobaric hypoxia might indicate which athletes would improve their sea level performance after training at moderate altitude because of a hypoxia induced increase in total haemoglobin mass. We did not include a control group of elite junior swimmers performing equivalent training at sea level as it was not the aim of this study to examine whether or not the mean increase in sea level performance is greater after altitude training compared to equivalent sea level training.
There is some debate about the physiological limit of total haemoglobin mass in endurance athletes. While Gore et al12 suggested that world class endurance athletes might have “maximised” their total haemoglobin mass after many years of sea level training, Schmidt et al19 recently reported significantly higher total haemoglobin mass in professional cyclists living at an altitude of 2600 m compared to professional cyclists living at sea level with similar Vo2max, indicating that there is still potential for a further increase in total haemoglobin mass in sea level endurance athletes if they perform altitude training. The subjects in the present study were elite junior swimmers who undoubtedly still had the potential to increase total haemoglobin mass, whose erythropoiesis was not impaired by insufficient iron availability, and who lived and trained at an altitude high enough for a sufficient hypoxia induced increase in erythropoiesis. The significant mean increase in total haemoglobin mass (red cell volume) of 0.8 g kg–1 (1.8 ml kg–1) found in these elite junior swimmers after 3 weeks of living and training at moderate altitude is comparable to the results of Levine et al13 who reported a mean increase in red cell volume of 3.0 ml kg–1 in college runners after 4 weeks of living and training at an altitude of 2500 m. The individual variation in the changes of total haemoglobin mass in the present study was remarkable and varied between a 3.7% decrease and a 24% increase in the sea level baseline value (fig 2). There is also some debate about the extent to which total haemoglobin mass can be increased during altitude acclimatisation. Because of the results of a dose-response study in which the changes in Hb during a 6 week treatment with recombinant human EPO were measured20 in healthy young males, the results of a number of altitude acclimation studies with large increases in red cell volume were questioned.21 According to the calculations of Sawka et al21 and of Berglund and Ekblom,20 the 24% increase in total haemoglobin mass in one female swimmer in the present study seems to be incredibly high. However, to our knowledge, there exist no studies in which the changes in total haemoglobin mass following treatment with recombinant human EPO were measured and it is not known to what extent total haemoglobin mass can be increased in trained subjects when circulating EPO levels are elevated.
What is already known on this topic
Wide inter-individual variations have been observed in the increase in erythropoietin levels during altitude exposure as well as in the increase in total haemoglobin mass and in the improvement in sea-level performance after altitude training.
There was no significant correlation between the EPO response to altitude and the change in total haemoglobin mass. This finding is in accordance with results reported by Rusko et al14 who did not find a correlation between EPO values on days 2 and 25 of hypoxia exposure and the significant increase in total red cell volume in cross country skiers who lived 12–16 h daily for 25 days in normobaric hypoxia (Fio2 0.15) and who trained in normoxia. Thus, the assumption made by Chapman et al1 that a large acute EPO increase during altitude exposure would cause a respective increase in total haemoglobin mass could not be confirmed.
Apparently, there is no simple linear relationship between punctual EPO measurements during altitude training and the increase in total haemoglobin mass. One reason might be an inter-individual variation in the response to the hypoxia induced EPO increase. Richalet et al2 not only found a great inter-individual variability in the EPO response to high altitude at 6542 m, but also reported high and low responders to the hypoxia induced EPO increase, with, for example, relatively low EPO levels in subjects with sharp Hb increases. Furthermore, the inter-individual variability in the EPO response to hypoxia is not clearly understood. It can partially be explained by variations in O2 supply to the EPO producing renal tissue, but renal blood flow and O2 consumption in the tubular cells seem to be even more important determinants.2,3 Renal tissue oxygenation, which is improved with acclimatisation, to a great extent explains the decrease in EPO during prolonged altitude exposure.2,3,14,22 As could be seen in the present study, the EPO decrease had occurred after about 1 week of exposure to moderate altitude when secondary polycythaemia has not yet completely developed.6
Another reason for the lack of significant correlation between the EPO response to altitude and the change in total haemoglobin mass could be a mild neocytolysis that might have occurred in some of the swimmers during the 10 days between return to sea level and measurement of total haemoglobin mass. Rice et al23 observed a 7–10% decrease in red cell mass in polycythaemic high altitude (4380 m) residents with Hb values of 21–26 g dl−1 on descent to sea level due to neocytolysis caused by suppressed EPO levels. Gore et al12 and Dill et al10 did not report a significant decrease in total haemoglobin mass in elite athletes during repeated measurements up to 20 days after training at moderate altitude (2300–2700 m). We cannot completely exclude that total haemoglobin mass slightly decreased in some of the swimmers during the first days after descent to sea level. However, we had decided to measure total haemoglobin mass and performance 10 days after return to sea level because, according to the experienced German coaches, this time interval is required for swimmers to achieve maximal sea level performance after altitude training.
What this study adds
The erythropoietin response after 4 h hypoxic exposure at an ambient Po2 corresponding to the training altitude is closely related to the acute erythropoietin increase during altitude training but does not allow prediction of the variation in the increase in total haemoglobin mass or in sea-level performance after descent.
The importance of increased total haemoglobin mass for aerobic capacity has been shown repeatedly24,25 and is supported by studies on blood doping.26 Therefore, a wide inter-individual variability in sea level performance after altitude training might very likely be explained by the observed inter-individual variation in the change in total haemoglobin mass. In the present study, the changes in total haemoglobin mass did not correlate with the changes in maximal performance or with performance at a lactate concentration of 4 mmol l−1.
It is a weakness of the present study that we could not measure Vo2max before and after altitude training in a specific test, for example during an incremental swim test in a flume. Instead, subjects performed an incremental swim test in a 50 m pool, the test performance at a 4 mmol l−1 lactate concentration being the most important measure. After altitude training, performance at a 4 mmol l−1 lactate concentration as well as maximal performance were significantly increased by 2–3%. These increases showed considerable inter-individual variation which cannot be explained by differences in the individual training programs at altitude as the training of all swimmers was supervised by experienced coaches. Performance changes were not correlated with the change in total haemoglobin mass, perhaps because both aerobic and anaerobic capacity are very likely determining factors for maximal performance and for performance at a lactate concentration of 4 mmol l−1. It has been shown in other studies that anaerobic capacity can also be influenced by altitude training.27,28
In conclusion, this investigation confirmed the wide inter-individual variation in the erythropoietic response to altitude training in elite athletes and demonstrated that the EPO increase which occurred during the first days of living and training at moderate altitude correlated well with the EPO response after 4 h exposure to equivalent normobaric hypoxia. However, the variability in the increase in total haemoglobin mass and in sea level performance after training at moderate altitude could not be predicted by the EPO response to acute hypoxic exposure.
Acknowledgments
The authors wish to thank all the swimmers and coaches, especially head coach Achim Jedamsky, for their co-operation. We further gratefully acknowledge the technical assistance of Judith Schönith and Martina Haselmayr throughout the study and the help of Stefan Borisch with the measurements of total haemoglobin mass.
REFERENCES
Footnotes
-
Competing interests: none declared
-
The study was supported by Deutscher Sportbund