Article Text

Abstract
Background: The nature of tendon neovascularisation associated with pain over time has not been studied.
Objective: To prospectively study the patellar tendons in elite junior volleyball players.
Methods: The patellar tendons in all students at the Swedish National Centre for high school volleyball were evaluated clinically and by ultrasonography (US) and Power Doppler (PD) sonography.
Results: Altogether 120 patellar tendons were followed for 7 months. At inclusion, jumper’s knee was diagnosed clinically in 17 patellar tendons. There were structural changes on US in 14 tendons, in 13 of which PD sonography showed neovascularisation. There were 70 clinically normal tendons with normal US and PD sonography, 24 clinically normal tendons with abnormal US but normal PD sonography, and nine clinically normal tendons with abnormal US and neovascularisation on PD sonography. At 7 month follow up, jumper’s knee was diagnosed clinically and by US in 19 patellar tendons, in 17 of which there was neovascularisation. Three of nine clinically normal tendons with structural changes and neovascularisation at inclusion developed jumper’s knee. Two of 24 tendons clinically normal at inclusion, with abnormal US but normal PD sonography, developed jumper’s knee with abnormal US and neovascularisation on PD sonography. A total of 20 clinically normal tendons with normal US and PD sonography at inclusion developed structural tendon changes and 12 of these also developed neovascularisation.
Conclusions: The clinical diagnosis of jumper’s knee is most often associated with neovascularisation in the area with structural tendon changes. The finding of neovessels might indicate a deterioration of the condition.
- PD, power Doppler
- US, ultrasonography
- jumper’s knee
- neovascularisation
- pain
Statistics from Altmetric.com
Jumper’s knee (chronic patellar tendinosis) is a troublesome condition with unknown aetiology and pathogenesis. The condition is mainly seen in athletes engaged in explosive jumping sports,1–3 and is likely associated with overloading of the knee extensor mechanism.3–8 Jumper’s knee is the most common overuse injury in volleyball (28%), and 40% of professional players have experienced symptoms of jumper’s knee during their careers.9
Clinically, jumper’s knee is characterised by activity related pain and/or soreness at the patellar tendon attachment to the patella.1,3,5,10 The condition is difficult to treat and there is no treatment of choice, conservative or surgical.11–14 Several studies report unpredictable results with surgical treatment.3,15–19 Interestingly, it is not yet known where the pain comes from in this condition.20,21
Ultrasonography (US) is a good method to study the tendon structure.22,23 In both adolescent and adult patients with a long history of pain from the patellar tendon, examination usually shows a local widening, irregular collagen fibre structure, and hypoechogenic areas in the patellar tendon insertion into the patella.2,24 However, these changes can also be seen in asymptomatic athletes.25–27 Power Doppler (PD) and colour Doppler techniques can be used to study blood flow in the tendon.28–30 However, only high flow rates can be registered with these techniques as normal blood flow in the tendon does not register due to its relatively low flow rate. Recent studies on chronic painful Achilles tendon have indicated an association between pain during tendon loading activity and the occurrence of neovascularisation in the area with tendon changes.30,31
The aim of this prospective study was to clinically, and by grey scale US and PD sonography, follow the patellar tendons in elite junior volleyball players (15–19 years) at the Swedish National Centre for volleyball during one season (30 weeks) of high intensity training and playing. We were particularly interested in the occurrence of neovascularisation and pain.
METHODS
Subjects
The most talented junior volleyball players in Sweden are recruited to the Swedish National Centre for high school volleyball. General physical tests and sport specific tests are undertaken regularly. During their 3 years at the Swedish National Centre for high school volleyball, the players consistently train and play 15 h/week throughout the season. Most of the volleyball players are members of the Swedish Junior National Team and participate in international tournaments. Four teams represent the high school in the Swedish Volleyball Federation leagues, from the women’s top elite division to the first and second divisions for men and women.
After permission from the Educational Board of the Swedish National Centre for volleyball, all 60 players (29 male and 31 female) in first, second, and third grades (15–19 years old) were invited to participate in the study.
The study was approved by the Ethical Committee of the Medical Faculty at the University of Gothenburg, Sweden. All volleyball players provided written informed consent.
The study started at the beginning of the semester in September 2002 with a lecture on jumper’s knee (patellar tendinosis) for all students. Thereafter, all students filled out a questionnaire (see below) with investigator (KG) assistance.
Questionnaire and clinical examination
Questions to the athletes included: date of birth, amount and type of training, present and former symptoms involving the patellar tendon, treatments, other knee injuries, and results of treatments. The volleyball players who reported pain at the patellar tendon marked the area of pain on a special knee chart.
All participants underwent a clinical knee examination by a registered sports physiotherapist (KG). The examination included palpation of the patellar tendon, in particular its attachment to the inferior pole of the patella. Tests that aimed to reproduce the pain of patellar tendinosis included: one leg body weighted squats and drop jumps (plyometric jump) on each leg from 20 cm and/or 43 cm. Clinical tests to exclude differential diagnoses were also performed.
The following diagnostic criteria for jumper’s knee were used: history (>4 weeks) of exercise/volleyball associated pain at the patellar tendon insertion into the inferior pole of the patella,1 tenderness to palpation,1,32 and pain during provocative tests of the knee extensors.5,33,34
Sonography
A single experienced musculoskeletal radiologist, who was blinded to the volleyball player’s clinical history, performed all US and PD examinations. A high resolution linear array 8 MHz ultrasound transducer (Sequoia 512, Acuson, Mountain View, CA) was used for all examinations.
Grey scale US
US was performed using longitudinal and transverse grey scale scans of the left and right patellar tendons with the patient lying supine and the knees in extension. The thickness of the tendon was measured and structural changes (hypoechoic areas) evident in both the longitudinal and the transverse scans were recorded.
PD examination
PD sonography was used to study blood flow in the patellar tendon. As only high flows can be registered, the technique does not allow for registration of the normal circulation in the tendon because of the relatively low flow rate.
To our knowledge, there is no method to quantify blood flow in the tendon. Therefore, we used a semi-quantitative scale as follows: 0, no flow; 1, flow outside the tendon; 2, one or two vessels inside the tendon; and 3, multiple vessels inside the tendon.
For analysis, only those tendons with vessels inside the tendon were considered to have neovascularisation.
Statistical methods
The results are presented as means (SD) and were analysed with Excel 2000 (Microsoft, Redmond, WA, USA).
RESULTS
Subject characteristics
All 60 volleyball players, 29 males (48%) and 31 females (52%), studying at The Swedish National Centre of high school volleyball participated in the study. Of these 60 players (120 tendons), one player had previously been treated with steroid injections and had later been surgically treated bilaterally for jumper’s knee (patellar tendinosis) and one player had previously been treated with steroid injections in one tendon. The surgical treatment and the treatment with steroid injections were carried 9 months before the study started. These two players were included in the study. Descriptive data on the subjects are presented in table 1. All results are presented as numbers of tendons (not number of individuals).
Volleyball players (n = 60) basic data at baseline
At baseline
A clinical diagnosis of jumper’s knee was made in 17 patellar tendons (10 male and seven female), 14 of which also had structural changes on US. In 13 (10 male and three female) of these 14 tendons, PD sonography showed neovascularisation within the area of structural changes on US (figs 1 and 2; tables 2 and 3). A total of 70 tendons (32 male and 38 female) were clinically normal, had normal US, and had no neovascularisation on PD sonography. However, 24 clinically normal tendons (nine male and 15 female) had abnormal US but had no neovascularisation on PD sonography, while nine clinically normal tendons (seven male and two female) had abnormal US and neovascularisation on PD sonography. Three tendons (three female) positive for a clinical diagnosis of jumper’s knee had a normal US and no neovascularisation on PD sonography.
Jumper’s knee in volleyball players (n = 60) at baseline and at 7 month follow up
Jumper’s knee symptoms and sonographic findings at baseline and at 7 month follow up
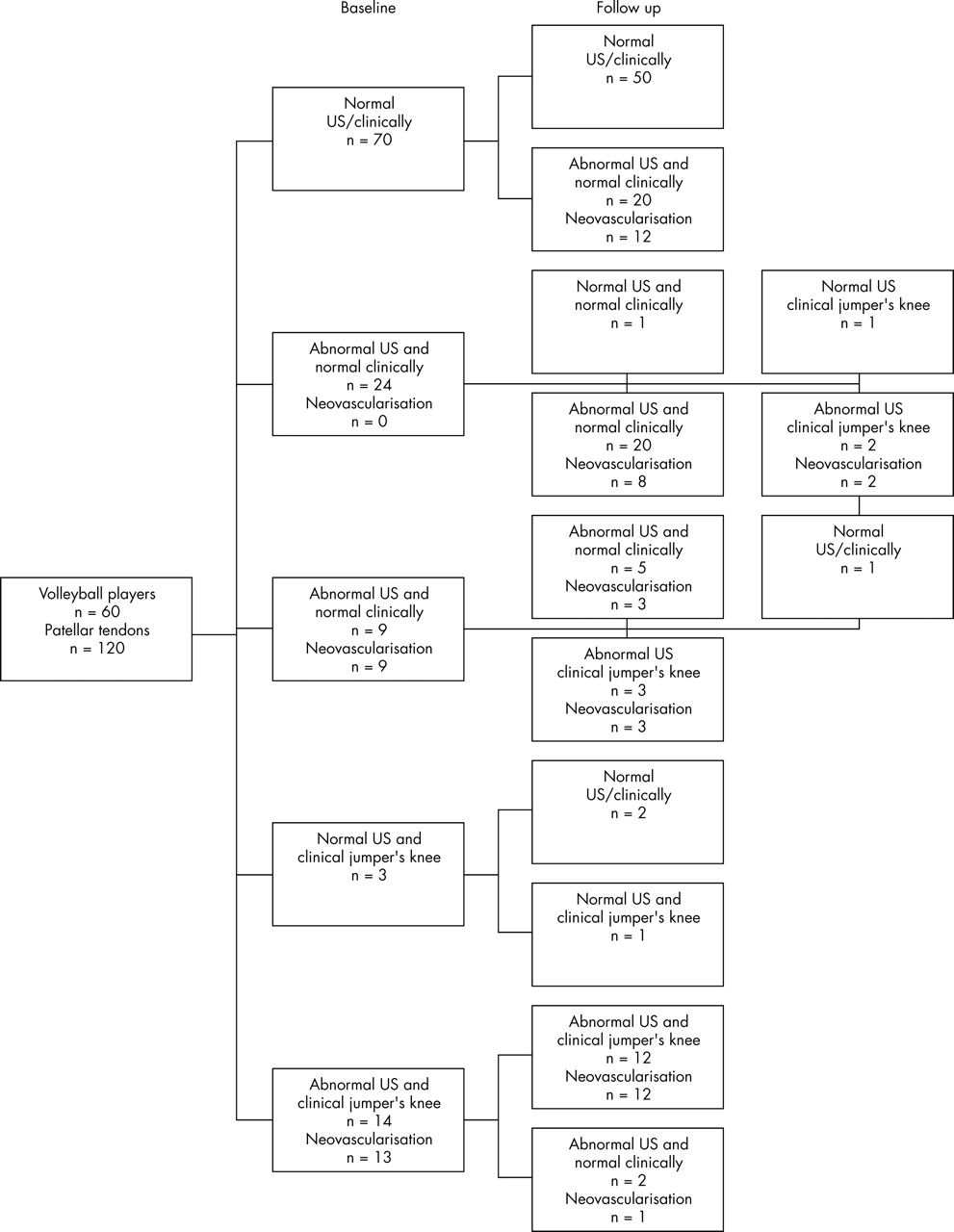
Flow chart summarising the longitudinal outcomes.

{kind=link}
{kind=link}
Longitudinal scan of the patellar tendon. The hypoechic region and neovascularisation is seen in the marked area. PD signals indicate flow inside the tendon and its immediate surroundings.
At 7 month follow up
A clinical diagnosis of jumper’s knee was made in 19 tendons (13 male and six female). In 17 (13 male and four female) of these there were also structural tendon changes on US and neovascularisation on PD sonography (fig 1; tables 2 and 3).
During the 7 month period of observation, three (two male and one female) of the nine asymptomatic tendons with structural changes and neovascularisation at inclusion developed clinical symptoms of jumper’s knee, and had abnormal US and neovascularisation on PD sonography. Of the remaining six tendons in this category at inclusion, three tendons (three male) did not change in any respect, in two tendons (two male) the neovascularisation disappeared on PD sonography, and in one tendon (one female) the US normalised (that is, vessels also disappeared).
Two of 24 clinically normal tendons (one male and one female) which had abnormal US but no neovascularisation on PD sonography at inclusion, developed clinical jumper’s knee, together with abnormal US and neovascularisation on PD sonography.
A total of 20 pain free and ultrasonographically normal tendons developed structural tendon changes on US, and 12 of these (nine male and three female) also developed neovascularisation on PD sonography.
At inclusion, three tendons (three female) were diagnosed clinically as having jumper’s knee but had normal US and no neovascularisation on PD sonography. At follow up, two of these were now clinically normal and still had normal US and no neovascularisation on PD sonography. The other was still diagnosed as jumper’s knee, but had normal US and no neovascularisation on PD sonography.
DISCUSSION
This longitudinal study provides novel cross sectional and longitudinal data regarding structural changes on US, neovessels seen on PD sonography, and clinical correlation in jumper’s knee.
Prevalence and structural abnormality on US
Jumper’s knee is a common problem among senior volleyball players.9 This investigation shows that jumper’s knee is already relatively common (14%) among high level volleyball players at a relatively young age. This is higher than the 7% Cook et al reported in a group of male and female basketball players (14–18 years of age),2 but lower than the 36% reported by Lian et al in a group of 47 male senior professional volleyball players.27
The absence of an association between structural tendon changes and symptoms of jumper’s knee has previously been reported.19,26,27 In our study, we found grey scale structural tendon changes at baseline, but no pain, in 33/120 tendons (28%). Neovessels as seen on PD sonography, however, had a 59% correct association with pain (13 painful of 22 with neovessels). At follow up, there were structural tendon changes, but no pain, in 47/120 tendons (39%). Cook et al found structural changes, but no pain, in 56/268 (21%) patellar tendons in a similar group of junior basketball players.2
The results are comparable with those in a group of asymptomatic male elite soccer players, where structural changes were present in 18/98 tendons (18%) at baseline and in 15/98 tendons (15%) at follow up.35 In 3/18 tendons with persistent structural tendon changes, symptoms characterised as jumper’s knee had developed.35
Association between neovessels and tendon pain
The possible relationship between chronic tendon pain and neovascularisation has recently been highlighted in the Achilles tendon. In patients with chronic painful mid-portion Achilles tendinosis30,31 and chronic insertional Achilles tendon pain,36 we demonstrated an association between the occurrence of neovascularisation and pain during tendon loading activity. Also, Terslev et al28 reported an association between neovessels and pain in a small sample of elite male basketball players with jumper’s knee. In the present study, the majority of patients, especially the males, who had a clinical diagnosis of jumper’s knee also had structural tendon changes and neovascularisation. These findings indicate a possible relationship between the combination of structural tendon changes plus neovascularisation, and pain during patellar tendon loading activity. It is noteworthy that at inclusion there were nine clinically normal tendons that had structural tendon changes plus neovascularisation, but no pain. Interestingly, during the 7 months of observation, three out of these nine tendons developed clinical jumper’s knee. This is a high proportion (33%), possibly indicating that it could be worth screening this at risk population. Furthermore, in 12 out of the 70 tendons that were normal at inclusion, structural tendon changes and neovascularisation developed during the follow up period. This was not associated with pain at that time, but further longitudinal follow up is warranted.
In the present study, it was interesting to notice that during the 7 month period of high intensity training and volleyball playing, structural tendon changes and neovascularisation developed in 12 tendons. Almost all of these tendons belonged to individuals in the second and third grades (11/12) where there is more specific and heavier weight training, and a higher intensity and frequency of volleyball training compared to first grade. Altogether, most of the tendons with structural tendon changes belonged to individuals in grades two and three. This is in accordance with the findings reported by Cook et al in a similar group of junior basketball players.2 Structural tendon changes have previously been suggested to increase the risk of developing symptoms of jumper’s knee in junior basketball players.37
What is already known on this topic
Jumper’s knee (chronic patellar tendinosis) is a troublesome condition mainly seen in athletes engaged in explosive jumping sports, such as volleyball, and is likely associated with overloading of the knee extensor mechanism.
The correlation between the occurrence of neovessels and pain is moderate in this study but better than that found using grey scale US alone in the cross sectional analysis. However, this is a prospective study, and perhaps neovessels are early signs of a deterioration of the condition, in later stages resulting in pain during tendon loading activity. Further studies should examine whether vascular effects (ingrowth, dilatation) precede neural changes (ingrowth, stimulation) in this condition. Further follow up studies will clarify the fate of these tendons.
In summary, a clinical diagnosis of jumper’s knee in junior elite volleyball players is associated with neovascularisation in the area with structural tendon changes, and neovascularisation together with structural tendon changes in asymptomatic volleyball players may indicate a risk for developing jumper’s knee. Further prospective studies over a longer period of time can possibly clarify the dynamic patterns between the development of clinical symptoms and structural and vasculoneural tendon changes.
What this study adds
Neovascularisation was a common finding in adolescent elite junior volleyball players with a clinical diagnosis of jumper’s knee combined with structural tendon changes at ultrasonography. The occurrence of neovessels might possibly indicate a deterioration of the condition.
REFERENCES
Commentary
This clinical paper deals with the most intriguing matter of overuse related tendon changes in athletes. This study may in particular facilitate the search for the missing link between structural changes and symptoms.1,2 The association of neovascularisation and symptoms (or increased risk for symptoms) supports earlier mentioned hypotheses of neural ingrowth accompanying neovessels and possibly causing pain in tendinopathy.3 The idea, suggested by the authors, that neovascularisation reflects a deterioration of the condition was also mentioned in connection with Achilles tendinopathy.4 However, whether the vascular ingrowth precedes the neural ingrowth in tendinopathy is thus far not substantiated and warrants further studies on this subject. Moreover, a notable observation is the existence of clinical tendinopathy without ultrasonographic changes or neovascularisation. This type of patients would not fit in the suggested pattern of symptoms and vasculoneural tendon changes. Nevertheless, much credit must be given to this very interesting clinical study that undeniably will prompt further research on tendinopathy.
Footnotes
-
Competing interests: none declared.