Article Text

Abstract
Achilles tendinopathy affects athletes, recreational exercisers and even inactive people. The pathology is not inflammatory; it is a failed healing response. The source of pain in tendinopathy could be related to the neurovascular ingrowth seen in the tendon’s response to injury. The treatment of Achilles tendinopathy is primarily conservative with an array of effective treatment options now available to the primary care practitioner. If conservative treatment is not successful, then surgery relieves pain in the majority of cases. Directing a patient through the algorithm presented here will maximise positive treatment outcomes.
- CSI, corticosteroid injection
- NSAID, non-steroidal anti-inflammatory drug
Statistics from Altmetric.com
Pain in the Achilles tendon is relatively common in recreational exercisers and individuals active in sports.1 Achilles tendon pain has also been reported in inactive individuals.2 It is seen most commonly in the mid-portion of the tendon, but also occurs at the bone–tendon junction.
Overuse is considered to induce the condition,3 but the aetiology and pathogenesis have not been scientifically clarified. A study on chronic Achilles tendinopathy (342 tendons) showed that physical activity was not correlated with the extent of histopathology, suggesting that physical activity could be more important in provoking the symptoms than being the root cause of pathology.4 The lack of association between activity, pain and structural abnormality has also been reported in other tendons, and pathological changes are seen on imaging in physically active asymptomatic individuals.5
Pathological change in the tendon can manifest clinically as tendon swelling or nodules. It is also clearly visible with standard soft-tissue imaging techniques. This review focuses on treatment of Achilles mid-tendon pain; management of rupture, insertional pathology and peritendinopathy are outside the scope of this article.
TENDON HISTOPATHOLOGY
The four cornerstones of tendon histopathology are (1) cellular activation and increase in cell numbers, (2) increase in ground substance, (3) collagen disarray and (4) neovascularisation. It is not considered to be a primarily inflammatory condition. Histological evaluation of Achilles tendon biopsies, intratendinous microdialysis6,7 and contemporary molecular biology techniques (cDNA-arrays, real-time quantitative PCR) of appropriately prepared biopsy tissue8 all failed to show evidence of prostaglandin-mediated inflammation.
There are, however, signs of neurogenic inflammation.9 The presence of neuropeptides such as substance P and calcitonin gene-related peptide indicate that there still might be an inflammation in the tendon.10 Peripheral local noxious stimulation makes peptidergic group IV fibres release peptides from their terminals, starting various pathophysiological processes contributing to neurogenic inflammation.
WHERE DOES THE PAIN COME FROM?
It is well known that the chronic painful Achilles and patellar tendons are difficult to treat, and the pain mechanisms associated with these conditions are not understood. Methods such as the above-mentioned microdialysis, cDNA-arrays and PCR, as well as ultrasonography combined with colour Doppler, provide novel and potentially important information about the chronic painful Achilles tendon versus normal Achilles tendon.
Glutamate, a well known neurotransmitter and very potent modulator of pain in the central nervous system, is found in high levels in painful tendons but not in normal tendons.11 In conjunction with the findings of a local neurovascular ingrowth12 and promising results of pilot studies with sclerosing injections, there is now some evidence that the neural pathways associated with tendinopathy could be associated with the neovascularisation. Biopsies taken from an area with tendinosis with neovascularisation showed nerve structures in close relationship with the vessels;12 studies have shown substance P nerves in the vascular wall and calcitonin gene-related peptide nerves close to the vascular wall.12,13 Also, the neurokinin-1 receptor, which is known to have a high affinity for substance P, has been found in the vascular wall.14 The findings suggest, for the first time, an explanation for the pain associated with tendinosis. As interference with this neurovascular ingrowth via sclerotherapy (see below) appears to decrease pain, further research appears well justified.
DIAGNOSIS
A correct clinical diagnosis can often be established solely by clinical examination, especially if the tendon exhibits focal or generalised swelling. If a clinical diagnosis is not clear, ultrasonography or MRI may reveal the pathology within the tendon.15 Although abnormalities detected by imaging are likely to be associated with pain, it is possible that these morphological abnormalities are painless and that pain may be arising from another source. Clinical acumen is important to correlate clinical and imaging examinations.
The first priority of clinical examination is to exclude acute rupture, and the calf squeeze test has excellent validity.16 After demonstrating that the tendon is intact, the examination should aim to provoke tendon pain during tendon-loading activity. In most patients, simple single-leg heel raises will be sufficient to cause pain. In more active individuals, however, it may be necessary to ask the patient to hop on the spot, or hop forward, to further load the tendon and reproduce pain. Repetition of the loading test may be necessary in some athletes to fully evaluate the tendon.
It is important to exclude other diagnoses such as posterior ankle impingement, os trigonum syndrome, tenosynovitis or dislocation of the peroneal or other plantar flexor tendons, an accessory soleus muscle, irritation or neuroma of the sural nerve and systemic inflammatory disease. These diagnoses cause pain in and also around the Achilles tendon; true tendon pain is nearly always confined to the tendon itself.
IMAGING
Imaging abnormalities in the tendon include hypoechoic areas seen on ultrasound and areas with increased signal intensity seen on MRI. These areas correspond with areas of altered collagen fibre structure and increased interfibrillar ground substance (proteoglycans and hydrophilic glycosaminoglycans).17,18 Signal intensity on MRI has been associated with the clinical outcome.19 However, the pathology is also found in tendons that appear normal on imaging.20
Colour and power Doppler have recently added a new dimension to standard ultrasound tendon imaging. This imaging demonstrates blood flow in tissues. In the Achilles tendon, blood flow is not detectable in normal tendons but colour Doppler often reveals blood flow in pathological tendons.21 Such blood flow has been linked to greater pain scores, poorer function and longer symptoms in the Achilles tendon,22 compared with control participants who have no visible flow. The association, however, is not absolute.23
The long-term clinical importance of blood vessels in pathological tendons is not clear. Two longitudinal studies have shown that the addition of colour Doppler at baseline examination did not improve the diagnostic performance of ultrasound19 or indicate a poorer outcome.24
Clinically, imaging should not be the sole guide for clinical decisions; variation in symptoms such as morning stiffness and load pain should direct treatment modification. Studies in many tendons have indicated that clinical outcomes are independent of imaging and change in imaging.19,25,26
TREATMENT
Many treatments are offered to patients with painful tendons, but the scientific evidence for most of the conservative and surgical treatments remains sparse. Treatments that have some evidential basis and have been investigated with randomised controlled trials include eccentric exercise, glyceryl trinitrate patches, electrotherapy (microcurrent and microwave), sclerosing injections and non-steroidal anti-inflammatory drugs (NSAIDs). Of these, NSAIDs showed little or no effect on outcome, and further discussion of medication has not been included in this review.27,28 There are no randomised or prospective studies that compare different conservative and surgical treatment regimens.
Conservative treatment is recommended as the initial strategy by most authors.29,30 This strategy includes identification and correction of possible aetiological factors, and a symptom-related approach. Generally, the initial treatment consists of a multifactorial approach that may include a combination of rest (complete or modified activity), medication (NSAIDs, corticosteroids), orthotic treatment (heel lift, change of shoes, corrections of malalignments), stretching and strength training.
If conservative treatment fails, surgical treatment is instituted. It has been a general opinion that in about 25% of patients with chronic painful conditions located in the Achilles tendon, non-surgical treatment is not successful and surgical treatment is needed.31 For the Achilles tendon, frequency of surgery has been shown to increase with patient’s age, duration of symptoms and occurrence of tendinopathic changes.31,32
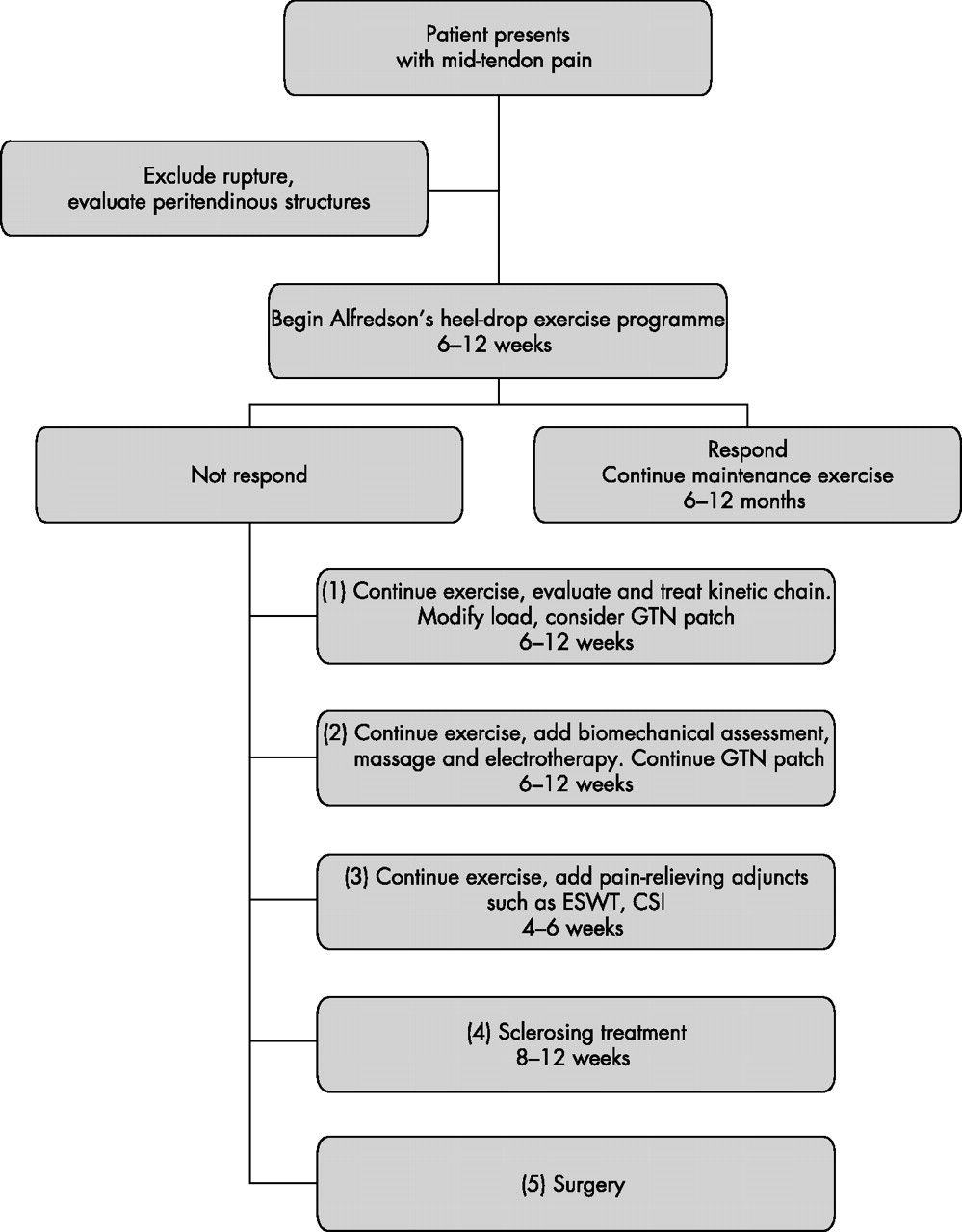
A treatment algorithm has been constructed to place these treatment options in a clinical reasoning order (fig 1). This order is appropriate for most individuals with Achilles tendon pain, but may need to vary in special cases such as the elite athlete, the person with acute tendon pain unable to fully bear weight or the older individual who may be unable to complete an exercise-based programme. The doctor must interpret individual needs and modify the algorithm for each clinical presentation.
{kind=link}
Algorithm for treating Achilles tendinopathy. Timeframes are recommended and should be modified as appropriate for individual presentations. CSI, corticosteroid injection; ESWT, extracorporeal shock wave therapy; GTN, topical glyceryl trinitrate.
NON-OPERATIVE TREATMENT METHODS
Eccentric musculotendinous training
Curwin,33 and Curwin and Stanish34 in 1984, stressed the importance of eccentric training as a part of the rehabilitation of tendon injuries. They demonstrated the success of a simple 6-week programme of progressive tendon load.34 Alfredson et al adapted this programme and scientifically evaluated an eccentric calf muscle training programme for painful mid-portion Achilles tendinopathy.2,35
Alfredson’s model of eccentric training involves no concentric loading and emphasises the need for patients to complete the exercise protocol despite pain in the tendon. If patients experience no tendon pain doing this programme, the load should be increased until the exercises provoke pain. Good short-term and long-term clinical results have been reported.35–37 This 12-week programme is effective when the other conventional treatments (rest, NSAIDs, change of shoes, orthoses, physical therapy and ordinary training programmes) have failed and is successful in approximately 90% of those with mid-tendon pain and pathology. Insertional Achilles tendon pain is not as responsive, and good clinical results are achieved in approximately 30% of tendons.38
A follow-up study (mean 3.8 years later) of patients treated with eccentric training indicated the majority of the patients were satisfied and back to previous tendon-loading activity level. Interestingly, the tendon thickness had decreased significantly, and ultrasonographically the tendon structure looked more normal.39 The same 12-week programme resulted in a decrease in tendon volume assessed with MRI, as well as a decrease in tendon signal intensity by 23%.40
Other exercise regimes that incorporate an eccentric component are also effective,41 but have not been as rigorously evaluated as the Alfredson programme. A concentric calf-muscle training programme (calf raises) did not prove as effective as the eccentric (heel-drop) training programme.42 In the eccentric group, 82% of patients were satisfied and back to previous activity level at the completion of treatment compared with those doing concentric exercise (36% satisfied patients).
Why does eccentric exercise reduce pain in tendinopathy?
Although there are several possible explanations for the effectiveness of eccentric exercise, none have been fully investigated. Eccentric exercise alters tendon pathology in both the short term and the long term. In the short term, a single bout of exercise increases tendon volume and signal intensity on MRI.43 A programme of eccentric exercise affects type I collagen production and, in the absence of ongoing insult, may increase the tendon volume over the longer term.44 As such, an eccentric exercise programme may increase tensile strength in the tendon over time. The effect of repetitive stretching, with a “lengthening” of the muscle–tendon unit, may also have an impact on capacity of the musculotendinous unit to effectively absorb load.
Another possible mechanism of action relates to mechanical insult of the pain-producing nerves. A unique feature of Alfredson’s eccentric training programme is that the patient is encouraged to undertake painful heel-drop exercises. As the nerve structures found in painful human tendons lie in close proximity to the tendon vessels, and as these vessels disappear with muscle contraction and stretch, the good clinical effects demonstrated with eccentric training could be due to alteration of the neovascularisation and accompanying nerves. The number of repetitions (180 repetitions/day) may damage the vessels and accompanying nerves as they traverse the soft tissue outside the tendon into the dense tendinosis tissue. The finding that patients satisfied with the result of the eccentric training regimen had no neovascularisation remaining, and all patients with a poor clinical result continued to have neovascularisation,39 is consistent with this hypothesis. However, that observation could also be the result of other upstream stimuli that influence both pain and neovascular obliteration, so we are not in a position to draw causal conclusions from an observational study.
Topical glyceryl trinitrate
This substance has been investigated in randomised controlled trials in the Achilles, elbow and supraspinatus tendons as an adjunct to an eccentric exercise programme. The topical glyceryl trinitrate was applied to the tendon as a patch that was renewed each day for 6 months. The treatment was compared with a placebo patch, and pain and function were measured over 6 months. In the Achilles tendon, activity pain in the treatment group was reduced at 12 and 24 weeks compared with placebo, and it also improved outcomes at 6 months.45 This study also supports the use of an eccentric exercise programme, as 49% of the placebo group reported excellent outcomes.
Extracorporeal shock wave therapy
Although extracorporeal shock wave therapy has been trialled in several tendons and fascial structures, there have been no randomised controlled trials in the Achilles tendon.46 In other structures, extracorporeal shock wave therapy decreases pain compared with a placebo,47 and may be beneficial in relieving pain, while rehabilitation of the musculotendinous structures continues.
Corticosteroid injection
In other tendons, corticosteroid injection (CSI) appears to have short-term pain-relieving effects but no effect or detrimental effects in the longer term.48 The short-term effect of CSI has been shown in the Achilles tendon with improvement in walking pain and reduction in tendon diameter as measured by ultrasonography.49 Intratendinous injection is contraindicated because of the catabolic effects,50 although a recent study of CSI into intratendinous vessels in six tendons has shown promising results.51 Peritendinous injection has fewer effects on the tendon and could be a worthwhile adjunct to a considered management programme.50 CSI may be most beneficial when used to relieve pain while continuing to undertake exercise programmes.
Electrophysical agents
The role of electrophysical agents in the treatment of tendinopathy remains poorly investigated in humans. Therapeutic ultrasound increases protein synthesis in tendons,52 but there is an oversupply of poor-quality protein in tendons suffering from overuse, so it may not improve clinical outcome to further increase protein production.
A recent randomised trial compared the outcome after hyperthermia with low-frequency microwave to traditional ultrasound.53 Significantly better outcomes were recorded by the hyperthermia group after treatment and 1 month later. Microcurrent applied for 2 weeks has been shown to decrease pain at 12 months when compared with conventional treatment.54
Other treatments
A night splint has been shown to be an effective intervention for Achilles tendinopathy.37 A greater reduction in pain was seen when the night splint was combined with a 12-week eccentric exercise programme. In both cases, when used alone and in conjunction with the eccentric exercise, a night splint reduced pain for 12 months.37
Biomechanical evaluation of the foot and leg is a clinically important part of Achilles tendon management. Although there is little empirical evidence to support the association between foot posture and Achilles tendinopathy,55 modification of foot posture in some patients can reduce pain and increase the capacity to load the tendon.56
Similarly, massage of the calf complex can assist rehabilitation, as can tendon mobilisation.57 Frictions have been shown to increase protein output of tendon cells;58 however, similar to the effect seen with ultrasonography, greater amounts of collagen and ground substance may not alter pain or pathology in a positive manner.
Sclerosing injections
The role of the neovascularisation in tendon pain has been further examined in a pilot study where a vascular sclerosant (Polidocanol—an aliphatic non-ionised nitrogen-free substance with a sclerosing and anaesthetic effect) was injected in the area with neovascularisation anterior to the tendon. Short-term (6 months) evaluation of this treatment showed that 8 of 10 tendons were pain free after a mean of two treatments.59 The tendons that were pain free had no neovascularisation either on the outside or the inside, but in the two non-successfully treated patients, vessels remained. A 2-year follow-up (our unpublished data) of these patients showed that the same eight patients remained pain free with no vessels in the tendon. Ultrasonographically, tendon thickness had decreased and the structure looked more normal. As vessel number has been shown to correlate with tendon thickness,23 treatment that decreases vessel number is also likely to affect tendon thickness.
In a double-blind, randomised controlled study comparing the effects of injections of a sclerosing and a non-sclerosing substance (lidocaine + epinephrine), the sclerosing substance was clearly more effective.60
The rehabilitation after sclerosing injection treatment includes a period of rest (1–3 days), then gradually increased tendon-loading activity, but no maximum loading (jumping, fast runs, heavy strength training) during the first 2 weeks. After 2 weeks, maximal tendon loading is allowed. After treating 400 Achilles tendons, we have had two complications that may be related to treatment. One patient who was treated in the Achilles tendon insertion sustained a total rupture in the proximal part of the tendon at the end of an 800 m track race 8 weeks after the treatment. Another patient who was treated in the mid-portion sustained a partial rupture in an area where he previously had four intratendinous CSIs. There have been no other complications. This research suggests a clinical role for sclerosing therapy in those who fail to respond to eccentric exercise.
SURGICAL TREATMENT
Surgical treatment for tendons that fail to respond to conservative treatment can involve several procedures, all of which are designed to irritate the tendon and initiate a chemically mediated healing response. These procedures range from more simple procedures such as percutaneous tenotomy61 to open procedures and removal of tendon pathology.
Percutaneous tenotomy resulted in 75% of patients reporting good or excellent results after 18 months. Open surgery for Achilles tendinopathy has shown that the outcomes are better for those tendons without a focal lesion compared with those with a focal area of tendinopathy.62 At 7 months after surgery, 67% had returned to physical activity, 88% from the no-lesion group and 50% from the group with a focal lesion.
What is already known about this topic
-
There are many conservative and surgical treatment options for Achilles tendinopathy
-
When and how to progress with treatment for recalcitrant Achilles tendinopathy can be a difficult clinical decision
What this study adds
-
A review of treatment options for Achilles tendinopathy
-
Suggested timeframes and sequential treatment strategies for resistant Achilles tendinopathy
Achilles tendon surgery requires extensive post-surgical rehabilitation and the results after surgery may only be as good as the strength and functional capacity that is regained. Adequate attention to rehabilitation is likely to improve outcomes for those who are surgically treated.
CONCLUSION
Achilles tendinopathy is a condition that can be effectively treated by the primary care practitioner. There are many simple and easily applied conservative treatment options that can relieve most tendon pain. Most of those who fail to respond to conservative care will find relief from surgical treatment.
REFERENCES
Footnotes
-
Published Online First 20 February 2007
-
Competing interests: None declared.