Article Text

Abstract
Objective: To evaluate the efficacy of ultrasound guided dry needling and autologous blood injection for the treatment of patellar tendinosis.
Design: Prospective cohort study.
Setting: Hospital/clinic based.
Patients: 47 knees in 44 patients (40 men, 7 women, mean age 34.5 years, age range 17 to 54 years) with refractory tendinosis underwent sonographic examination of the patellar tendon following referral with a clinical diagnosis of patellar tendinosis (mean symptom duration 12.9 months).
Interventions: Ultrasound guided dry needling and injection of autologous blood into the site of patellar tendinosis was performed on two occasions four weeks apart.
Main outcome measures: Pre- and post-procedure Victorian Institute of Sport Assessment scores (VISA) were collected to assess patient response to treatment. Follow up ultrasound examination was done in 21 patients (22 knees).
Results: Therapeutic intervention led to a significant improvement in VISA score: mean pre-procedure score = 39.8 (range 8 to 72) v mean post procedure score = 74.3 (range 29 to 100), p<0.001; mean follow up 14.8 months (range 6 to 22 months). Patients were able to return to their sporting interests. Follow up sonographic assessment showed a reduction in overall tendon thickness and in the size of the area of tendinosis (hypoechoic/anechoic areas within the proximal patellar tendon). A reduction was identified in interstitial tears within the tendon substance. Neovascularity did not reduce significantly or even increased.
Conclusions: Dry needling and autologous blood injection under ultrasound guidance shows promise as a treatment for patients with patellar tendinosis.
- VISA, Victorian Institute of Sport assessment score
- patellar tendinosis
- dry needling
- autologous blood injection
Statistics from Altmetric.com
Patellar tendinosis or jumper’s knee refers to a clinical syndrome characterised by anterior knee pain and tenderness at the inferior pole of the patella. It is recognised that this represents a phenomenon of myxoid degeneration and tearing of collagen fibres rather than being secondary to inflammation.1–3 This condition often causes morbidity in sport and may be refractory to treatment. Various techniques have been adopted for the treatment of patellar tendinosis, including physiotherapy,4 sclerosant injection,5 steroid injection,6 extracorporeal shock wave therapy,7 and surgical decompression with resection of the affected tendon and open stimulation techniques.7–9
Autologous blood injection has been evaluated as a treatment for lateral epicondylitis in humans,10,11 and in vitro studies have been carried out in rabbit patellar tendons.12
Our aim in the current study was to assess the efficacy of ultrasound guided dry needling and injection of autologous blood into the patellar tendon as a treatment for proximal patellar tendinosis. Following treatment, the patient adopts a standardised physiotherapy protocol to aid rehabilitation before re-starting full sporting activity.
METHODS
Patients
Forty seven knees in 44 consecutive patients were included in the study, which involved sonographic assessment of the patellar tendon and autologous blood injection. Informed consent of the patients and institutional review board approval were obtained before recruitment. There were 40 men and seven women (mean age 34.5 years, range 17 to 54 years) with 22 left and 25 right knees treated. The mean duration of symptoms was 12.9 months (range 1 to 48 months). Forty patients described sport as a precipitating factor. These included football (17), running (11), tennis (4), rugby (3), boxing (1), triathlon (1), dancing (1), golf (1), and martial arts (1).
Only patients with proximal patellar tendinosis were included in the study. Three patients were excluded as ultrasound showed the presence of multiple focal areas of calcification within the proximal tendon. It was felt that this might be an adverse factor in tendon healing. Two patients who had undergone previous surgery for anterior cruciate ligament reconstruction were also excluded. Pre-procedure Victorian Institute of Sport Assessment scores (VISA)13 were obtained in all patients to allow quantification of the symptoms and follow up assessment of the efficacy of treatment.
Sonographic technique
Sonography of the patellar tendon was carried out with the patient lying supine on an examination couch. The patient was positioned with the knee partially flexed by placing a pillow behind it. During sonography the patellar tendon was therefore under a degree of tension and the wavy configuration that is evident with the knee in full extension was abolished. Patients underwent diagnostic examination and therapeutic intervention at several institutions where the senior author practices. Ultrasound machines from two manufacturers were used: Siemens (Acuson) Sequoia (Siemens Medical Solutions, Mountain View, California, USA) with a 15L8W transducer and a Toshiba 5500.
Sonographic image interpretation
The patellar tendon was examined in both the transverse and longitudinal planes to confirm the imaging findings. The diagnosis of patellar tendinosis was based on the presence of four characteristic sonographic features. These included tendon size, focal alteration in tendon echotexture, interstitial clefts or tears (fibrillar disruption), and neovascularity (fig 1).

Longitudinal image of the proximal patellar tendon. Colour Doppler shows marked neovascularity in the hypoechoic segment of the proximal patellar tendon.
All patients included in the study had a hypoechoic tendon with loss of the normal fibrillar architecture in the affected tendon segment. A focal increase in proximal patellar tendon thickness was also universally apparent. Discreet interstitial tears were present in 31 patients (66%), with no intrasubstance tear identified in the remainder. Neovascularity was present in 39 patients (83%) (23 mild, 13 moderate, and three severe).
Procedure
Three millilitres of autologous blood were obtained from the antecubital fossa. Under aseptic technique and sonographic guidance, 3 ml of 0.5% bupivicaine was infiltrated along the superficial and deep aspects of the patellar tendon at the site of tendinosis. Once the local anaesthetic had been given sufficient time to act, the needle tip was positioned centrally within the site of tendinosis (fig 2). Following this the tendon was “dry needled”, passing the needle repeatedly through the abnormal tendon substance for a one minute period. The local anaesthetic syringe was then removed from the needle and the autologous blood filled syringe was attached, followed by slow injection of the blood. If areas of interstitial tears were evident on sonography, these were targeted for injection of the blood. Filling of these clefts can be directly visualised as fluid permeating between the abnormal hypoechoic clefts.

Longitudinal image of the proximal patellar tendon. The needle (arrow) has been inserted into the hypoechoic area before dry needling and autologous blood injection.
Follow up and physiotherapy protocol
Following the initial treatment, patients were advised to cease the sporting activities that precipitated their symptoms but to continue their activities of daily living. If they had been undergoing physiotherapy before autologous blood injection this was postponed until the treatment course was completed. A second injection was then scheduled at an interval of four weeks following the initial injection. At this time, a repeat sonographic assessment was undertaken, followed by dry needling and autologous blood injection using the same technique as at the initial visit. After the second injection, the patients were referred for a standardised physiotherapy programme specifically designed for the study. At the outset of treatment all patients are advised that the treatment consists of both injection and physiotherapy, and they should expect a three month healing period before they resume their previous levels of sporting activity.
All patients were asked to complete post-procedure VISA scores to allow assessment of the efficacy of the treatment. Twenty one patients (24 knees) were invited back for a repeat ultrasound examination to assess the changes in the patellar tendon following treatment.
Statistical analysis
Comparison was made between the pre- and post-procedure VISA score. Normality of the difference between the pre- and post-procedural VISA scores was assessed using the Kolmogorov–Smirnov test. The data did not show evidence of non-normality and were analysed using the paired sample t test. All statistical analysis was carried out using SPSS for Windows, version 14.0 (Chicago, Illinois, USA) and probability (p) values <0.05 were considered significant.
RESULTS
Clinical outcome
The mean (SD) pre-procedural VISA score was 39.8 (16.3), range 8 to 72. It increased significantly to 74.3 (17.5), range 29 to 100, on post-procedure follow up (t = 13.770, df = 43, p<0.001). The mean follow up period was 14.8 months, range 6 to 22. There were three treatment failures among the initial 47 patients. These patients failed to achieve symptomatic improvement. At follow up all three had undergone surgical decompression and so a follow up VISA score could not be recorded. One of these patients had two autologous blood injections but did not follow the physiotherapy protocol and returned immediately to sporting activity. The further two cases underwent routine injection and physiotherapy as per protocol.
Ultrasound outcome
Follow up ultrasound examination was undertaken using the same technique, knee position, and machine as in the pre-treatment examination. The ultrasound features that were used to diagnose patellar tendinosis were reassessed for interval change. These included overall tendon thickness, focal alteration in tendon echotexture, interstitial clefts or tears (fibrillar disruption), and neovascularity.
In all, 21 patients (24 knees) returned for ultrasound follow up examination. In 22 cases, a reduction in proximal tendon thickness was observed, with no difference in the remaining two cases. Furthermore, the size of the focal alteration in tendon echotexture reduced in 22 cases (fig 3), with one case remaining unchanged and one case showing an increase in length of the abnormally hypoechoic segment. In only a single case, however, was the tendon appearance classed as completely normal—that is, a return to the normal fibrillar pattern of the proximal patellar tendon. Two patients had tiny foci of calcification at the previous site of tendinosis (2 mm). Residual interstitial fissures/tears were identified in three cases but had resolved in 14. Neovascularity remained in 23 cases. The degree of neovascularity remained unchanged in nine cases, had lessened in five, and was more florid in nine.

{kind=link}
{kind=link}
{kind=link}
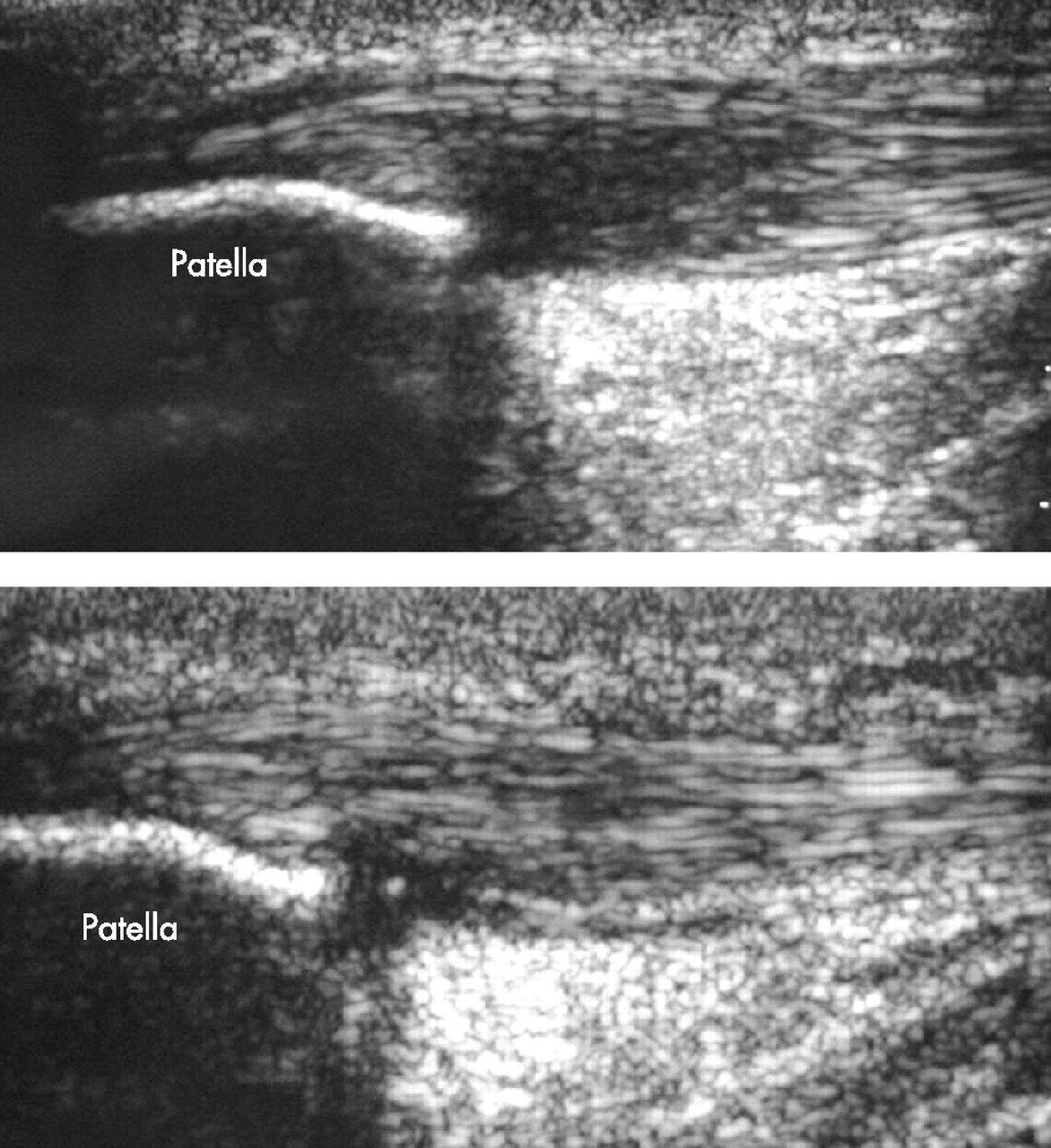
Longitudinal image of the proximal patellar tendon pre-treatment and 6 months post-treatment in the same patient. The post-treatment image shows near complete resolution of the hypoechoic segment in the proximal patellar tendon. There has been return of the normal echogenic fibrillar pattern in the tendon. There is a tiny residual hypoechoic segment at the insertion.
DISCUSSION
Patellar tendinosis or jumper’s knee is an extremely common knee disorder with an estimated incidence of between 13% and 20% in athletic populations.14–16 Various possible intrinsic aetiologies for this condition have been proposed in athletes, including abnormal patellar tracking,17 limb length discrepancy,14 and reduced flexibility of the quadriceps and hamstring muscle groups.18 While patellar tendinosis is often diagnosed clinically, magnetic resonance imaging and ultrasound are now well established.6,19–22 The sonographic features of tendinosis are well described in both the patellar tendon and elsewhere.10,20,23,24 We used four sonographic features for diagnosis and ultrasound follow up. These included tendon size, focal alteration in tendon echotexture, interstitial clefts or tears (fibrillar disruption), and neovascularity. The degree of neovascularity identified in patients with patellar tendinosis is affected by the position of the knee during sonographic assessment. In the extended position, neovascularity appears more florid and when tension is applied on the tendon in flexion, some of the neovascularity is abolished. For the purposes of the study and to ensure continuity, the knee was examined in a consistent position, resting on a pillow. This enabled an assessment to be made on follow up sonography of the degree of neovascularity. When the patient returned at four weeks for the second injection, we often observed that the hypoechoic focus in the proximal patellar tendon had become more echogenic. We postulate that this accumulation of echogenic material relates to the formation of immature scar tissue/granulation tissue, though we have no pathological evidence of this. Furthermore, there were changes in the neovascularity following the autologous blood injection. We anticipated that a decrease in tendon neovascularity would be observed; however, this only occurred in nine patients. An equal number of patients showed an increase in vascularity, which we cannot explain. This occurred despite resolution in symptoms and a return to sporting activity.
We assessed the clinical outcome of patients using VISA. This assesses symptomatology, simple function, and the ability to undertake sporting activity, scored out of 100. It has been validated as a clinical method for assessing the severity of a patient’s symptoms in patellar tendinosis and has been shown to be a reliable and reproducible index.13 We were able to demonstrated a significant in improvement in symptoms using our technique.
The injection of autologous blood into tendons has been evaluated in studies assessing the in vitro12 and in vivo10,11 effects on tendons. Taylor and co-workers assessed the effects of autologous blood injection on the strength of rabbit patellar tendons and found a significant increase in injected tendon strength when compared with the contralateral normal side.12 Connell and co-workers reported clinical and sonographic improvement in patients treated with autologous blood injections for lateral epicondylitis.10 In our study, the patellar tendon underwent barbotage or “dry needling” before autologous blood injection in all cases included in the study. This technique involves the repeated lancing of the area of abnormal tendon. It is done to stimulate an inflammatory response within the tendon. There is focal disruption of the collagen fibres within the area of tendinosis, so the process of dry needling is done to incite internal haemorrhage. It is then hypothesised that the inflammatory response induces the formation of granulation tissue which strengthens the tendon.11 Although our study design does not allow comment on the mechanism of action of this technique, several workers have postulated possible biological mechanisms that may contribute. Anitua and co-workers investigated the effects of platelet-rich clots on human tendon cells in culture. They found that autologous preparations rich in growth factors induce cell proliferation and promote synthesis of angiogenic factors during the healing process.25 Furthermore, it has been hypothesized that basic fibroblast growth factor and transforming growth factor β may act as humoral mediators in the induction of the healing cascade.26
We believe that it is essential that this procedure should be done under ultrasound guidance. Fredberg and co-workers found that the clinical suspicion of tendonitis could be confirmed by ultrasound evaluation in only one third of cases.6 Ultrasound therefore allows confirmation of the diagnosis and provides an imaging baseline under which the response can be assessed. It allows the area of tendon abnormality to be located precisely and interstitial tears to be identified and targeted for blood injection. Frequently, the abnormality can be quite focal and the injectate can be seen permeating the clefts within the tendon substance. In addition, physiotherapy plays a vital role in the ongoing treatment of patients following a period of rest and the series of injections. We used a standardised protocol based on the findings of Purdam et al.27 Loading of the patellar tendon was achieved by decline eccentric dips, with incrementally increasing load over three to six months, until the subject had returned to sport. All subjects also received quadriceps, hamstring, and calf stretches. The programme was home based, with regular physiotherapy clinic visits to guide the subject’s progression.
What is already known on this topic
-
Patellar tendinosis is a common problem causing morbidity in sport. It is often refractory to treatment. Autologous blood injection has been reported as showing promise in the treatment of this condition at other sites, for example in medial and lateral epicondylitis.
What this study adds
-
This study reports the technique of dry needling and autologous blood injection under sonographic guidance as a therapeutic option for patellar tendinosis.
-
Therapeutic intervention led to a significant improvement in VISA score as a measure of clinical outcome.
There are various limitations to our study. We are, in essence, evaluating two therapies simultaneously. Autologous blood injection and dry needling is combined with physiotherapy as part of our treatment protocol. We therefore do not know the relative importance of the autologous blood injection and the dry needling in the therapeutic outcome of the group studied. Previous workers have identified good results with painful eccentric quadriceps training, with significant improvement in clinical outcome.4 However, most of our patients had undergone a course of physiotherapy, and the tendinosis had proved refractory to this initial treatment. Second, although the VISA score provides an objective measure of clinical outcome in patients treated with this technique, we do not have any other objective measurement of tendon healing. The ultrasound findings are descriptive and rather subjective. It would be difficult to justify biopsy of the tendon to provide histological evidence of tendon healing. With this in mind, ultrasound was chosen as the method to monitor the “healing response” and to observe the sonographic appearances of tendons treated by this new technique. Further research is required with a randomised controlled trial of autologous blood injection/physiotherapy versus physiotherapy alone.
CONCLUSIONS
Dry needling and injection of autologous blood for patellar tendinosis shows promise as an alternative treatment for this chronic condition. It is important to carry out this technique under sonographic guidance so that the abnormal tendon can be targeted precisely for dry needling and injection of blood. The patient subsequently undergoes a course of physiotherapy following initial treatment before resuming sporting activity.
REFERENCES
COMMENTARY
Recalcitrant patella tendinopathy has traditionally been a difficult condition to treat successfully. An understanding of the importance of eccentric loading has certainly helped, and the availability of other modalities such as extracorporeal shock wave therapy gives clinicians more options, but this condition has always been frustrating to treat. Surgery has offered reasonable symptomatic relief, but in athletic endeavours that can be measured (such as high jump), a permanent decrease in performance can be observed. Autologous blood injection offers us an alternative treatment modality, and this study adds to the anecdotal evidence that it can be very effective in the treatment of patella tendinopathy.
Footnotes
-
Published Online First 26 March 2007