Article Text

Abstract
Background: “Tennis elbow” is a difficult condition to treat. Ultrasonography (US) and colour Doppler (CD) guided injections with polidocanol targeting the area with increased blood flow in the extensor origin have shown promising clinical results.
Objective: To evaluate and compare effects of US and CD guided intratendinous injections with sclerosing polidocanol and a local anaesthetic (lidocaine + epinephrine), in patients with tennis elbow.
Design: Prospective, randomised, controlled, double-blind, crossover study.
Setting: Sports Medicine Unit, Umeå University.
Patients: 32 patients (36 elbows), age range 27 to 66 years, with a long duration of elbow pain diagnosed as tennis elbow, were included in the study. All patients were followed up 3 and 12 months after treatment. Two patients were excluded due to other interventions during the study.
Interventions: One US and CD guided injection with the sclerosing agent polidocanol (group 1) or the local anaesthetic lidocaine plus epinephrine (group 2). At the 3 month follow-up, additional injections with polidocanol were offered to both groups (crossover for group 2).
Main outcome measures: Satisfaction with treatment (Yes/No), elbow pain during activity (visual analogue scale), and maximum voluntary grip strength.
Results: There were no significant (p<0.05) differences in the outcome between group 1 and group 2. In both groups, there was a significantly lower VAS at the 3-month and 12-month follow-ups, and grip strength was significantly higher at the 12-month follow-up.
Conclusions: US and CD guided intratendinous injections gave pain relief in patients with tennis elbow. Polidocanol and lidocaine plus epinephrine injections gave similar results.
Statistics from Altmetric.com
Tennis elbow, chronic pain of extensor origin, is known to be troublesome to treat. The aetiology and pathogenesis are unknown, as is the origin of pain. The general opinion is that the condition is due to overuse, and that the extensor carpi radialis brevis muscle (ECRB) plays a central role.1 – 3 Furthermore, there is no traditional inflammation.2 ,4 The histological findings vary, and include microrupture, granulation tissue and degenerative changes.2 ,3 ,5 ,6 Consequently, the term “lateral elbow tendinopathy or tendinosis” is used instead of “lateral epicondylitis”.
Numerous methods have been used to try to treat the condition, including physiotherapy, various types of injections, non-steroidal anti-inflammatory drugs (NSAIDS), various types of surgical treatments, orthotic devices and rest, but there is no “gold standard” for treatment.7 – 14 The target for most methods is the common extensor origin. Various substances have been used for injection treatment, including corticosteroids, platelet-rich plasma and autologous blood.9 ,11 ,13
Previous studies using ultrasound (US) and colour Doppler (CD) have shown increased blood flow in the extensor origin, and a possible relationship between increased blood flow and pain has been suggested.15
Recent studies on other tendons with chronic painful tendinosis, such as in the Achilles tendon and in the patellar tendon, have shown changes in vessels and nerves in the area.16 ,17 Ljung et al have shown an innervation pattern in the extensor origin,18 and in a recent pilot study, US and CD guided injections targeting the area with increased blood flow showed promising clinical results.19
The aim of this study was to evaluate the effects of US and CD guided injections with a sclerosing agent (polidocanol) and local anaesthetic (lidocaine plus epinephrine) in patients with tennis elbow. The hypothesis was that the sclerosing polidocanol, but not the non-sclerosing lidocaine plus epinephrine, would affect pain in the extensor origin and grip strength.
METHODS
The investigation was approved by the ethics committee of the Medical Faculty, University of Umeå. Informed consent was obtained from the patients after the study was explained both orally and in writing to them.
Participants
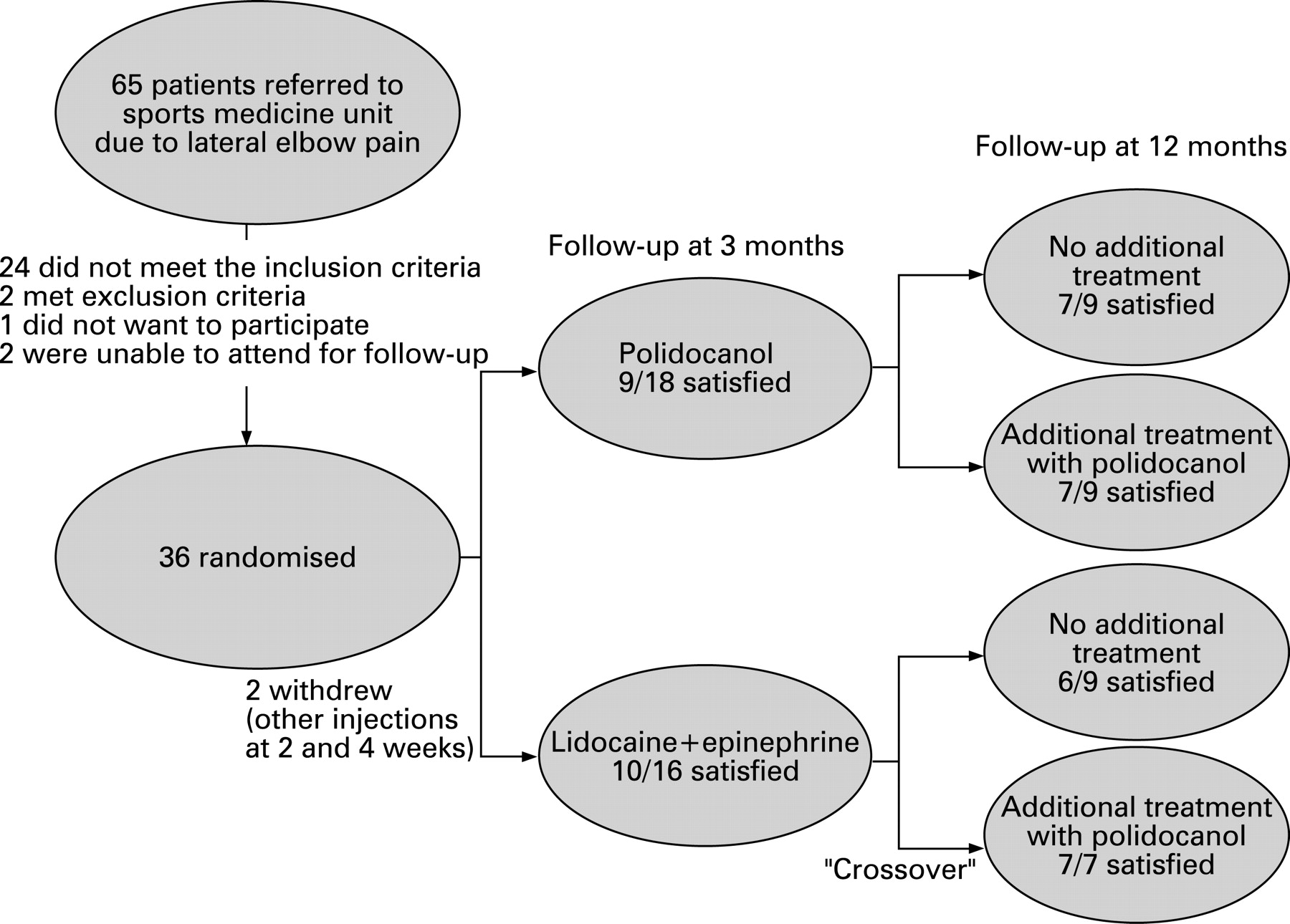
In total, 65 patients with lateral elbow pain were referred to the Sports Medicine Unit in Umeå between November 2005 and May 2006. Of these, 24 (37%) patients did not have the clinical diagnosis of tennis elbow, and were excluded. Thus, 32 patients (16 men, 16 women, mean age 46 years, range 27 to 66), with a long duration (mean 21 months, range 3 to 96) of pain diagnosed as tennis elbow (a total of 36 elbows), were eligible for the study.
All patients, except one who was retired, had pain symptoms during their work. Ten patients were on sick leave due to pain in the elbow. In 21 elbows, there was tennis elbow on the dominant side. Previous treatment included NSAIDs (n = 27), cortisone injections (n = 24), stretching (n = 22), eccentric training (n = 22), orthotic devices (n = 21), acupuncture (n = 13), ultrasound (n = 9), injection with botulinum toxin (n = 5) and surgery (tendon lengthening) (n = 2). Demographic data for each group are shown in table 1.
Inclusion criteria were pain on palpation of the extensor origin on the lateral epicondyle, pain elicited from the lateral epicondyle by forced extension of the wrist, symptoms for more than 3 months, and no interventions for the condition during the previous 3 months.
Exclusion criteria were arthritis, synovitis of the proximal radioulnar joint, entrapment of the radial nerve, generalised pain syndrome, radiculopathy from the cervical spine, and any other diseases (medial epicondylagia, impaired sensibility, paralysis) that would affect the outcome measurements. Two patients had the correct diagnosis but were excluded on the basis of these criteria. One had a generalised pain syndrome, and the other had had intracerebral haemorrhage with impaired sensibility.
Three more patients were offered participation in the study but rejected; one did not want any injections and the other two did nt live in the area and could not attend for follow-up.
Two further patients were excluded after the first follow-up: one had received an injection of botulinum toxin 2 weeks after inclusion in our study, and the other had received an injection of corticosteroids for pain in the flexor origin at the medial epicondyle of the elbow 4 weeks after inclusion.
Study design, randomisation and blinding
The study design is shown in fig 1. All the patients and the radiologist were blinded to the substance that was injected. The patients selected a sealed envelope from a box with 36 opaque envelopes, allocating them to one of the two treatments. The envelope was opened by an assistant in a separate room, where the substance was prepared for injection. The equipment was the same for all treatments, and there were no visible differences in colour or density between the two different substances. Immediately after the 3-month evaluation, the code was broken.
Sonography
All tendons were examined with high-resolution grey-scale US and with CD (Acuson Sequoia 512; 8–13 MHz frequency). The examinations were carried out with the patient in a sitting position, with the arm resting on a table, having 70–80° of elbow flexion and a pronated wrist. CD was used to locate increased blood flow. All participants had structural changes and increased blood flow in the area with tendon changes (fig 2).

{kind=link}
{kind=link}
Initial intervention
Two different substances were used for the injection treatment: polidocanol (10 mg/ml) (group 1) or lidocaine hydrochloride (10 mg/ml) plus epinephrine (5 μg/ml) (group 2). Polidocanol has a sclerosing effect by acting directly on the intimae layer in the vascular wall or indirectly by compressive effects on vessels through tissue expansion, and also has a local anaesthetic effect. Lidocaine hydrochloride has a local anaesthetic effect, and was combined with epinephrine to provide a vasoconstrictive effect.
The patients were given one injection of the appropriate substance. Participants sat in the same position as for the US/CD examination. Before treatment, the skin was washed with a solution of chlorhexidine and alcohol. The injections were performed with a 0.7×50 mm needle connected to a 2-ml syringe. The injections were performed dynamically, with the aid of real-time grey-scale US and CD guidance, injecting close to the target vessels inside the extensor origin. When the tip of the needle was positioned in the area with increased blood flow, a small volume of 0.5 ml of polidocanol or lidocaine plus epinephrine was injected (fig 2). Both substances had an immediate effect on the blood flow (no flow detected using CD), and all patients had temporary pain relief after injection. After treatment, there were no restrictions for patients’ activity level.
The same experienced radiologist (LÖ) performed all US and CD examinations and interventions.
Follow-up
The patients were followed up 3 months after injection. Patients in both groups were offered another injection with the sclerosing substance polidocanol (the study protocol included a crossover for group 2) if pain still existed. Patients given another injection were followed up every sixth week until 3 months after the last injection. Follow-up was carried out for all patients 12 months after the first injection.
Outcome measures
Primary outcome measures were (1) satisfaction with treatment (Yes/No) and (2) elbow pain during grip activities in daily life, including work situations. Using a 100-mm VAS for pain, 0, no pain; 100, severe pain). The secondary outcome measure was maximum voluntary grip strength, evaluated by using a hydraulic hand dynamometer (FEI Irvington, New York, USA). During the dynamometer test, the arm was held in the horizontal plane, with the elbow straight and the wrist in neutral position. Maximum grip strength was measured three times, and the highest value was used for statistical analysis.
Statistical analysis
Based on data from our pilot study (polidocanol injected in the extensor origin) in which 11/13 patients reported satisfaction, and the assumption that local anaesthesia would have a similar effect to placebo, it was calculated that 14 patients were needed in each group.19 The SPSS package (version 14.0, SPSS Inc, Chicago, Illinois, USA) was used for all statistical calculations. Differences between groups concerning continuous data were calculated using the Mann–Whitney U test. When data was categorical, the Fisher exact test was used. Differences over time within the groups were calculated using the Wilcoxon signed ranks test. Significance was set at p<0.05 for all groups.
RESULTS
Baseline data (age, duration of symptoms, sex, work, affected side, sick leave) did not differ between the two groups. At the 3-month follow-up, the patients who were not fully satisfied were offered additional injections with polidocanol (crossover for group 2). In group 1, nine patients had additional treatment (1–3 injections), and in group 2, seven patients had additional treatment with polidocanol (1–2 injections).
Follow-up at 3 months
At the 3-month follow-up, there were no significant differences in satisfaction with treatment (p = 0.51), pain during grip activity (p = 0.49) and grip strength (p = 0.86) between the patients in group 1 and the patients in group 2. Satisfaction with the treatment was reported by 9/18 (50%) patients in group 1 and 10/16 (62%) patients in group 2. The patients in both groups had a significantly lower VAS (pain during grip activity) after treatment than they had had before treatment (p = 0.026). Outcome for each group is shown in table 2.
Follow-up at 12 months
At the 12 month follow-up, there were no significant differences in satisfaction with the treatment (p = 1.0), pain during grip activity (p = 0.66) and grip strength (p = 0.11) between the two groups. Satisfaction with the treatment was reported by 14/18 (78%) patients in group 1 and 13/16 (81%) patients in group 2. The patients in both groups had a significantly lower VAS (p<0.000) and a significantly higher grip strength (p<0.000) after treatment than they before treatment. Outcome for each group is shown in table 2.
Adverse effects
There were no adverse effects in either group.
DISCUSSION
The main finding in our study was that there were no differences in the clinical results between US and CD guided intratendinous injections of the sclerosing substance polidocanol and the local anaesthetic lidocaine + epinephrine in patients with chronic painful tennis elbow. About half of the patients in both groups (50% and 62%, respectively) were satisfied with the results of the treatment at the 3-month follow-up. Additional injections in both groups (crossover design used for group 2), improved the clinical results to around 80% of patients satisfied. Of the non-satisfied patients, two were later treated surgically.
As there were no adverse effects in the groups, we consider the treatments safe. Three participants in group 2 noted increased elbow pain and stiffness during the first week after injection with lidocaine + epinephrine.
Tennis elbow is not always easy to diagnose. About one-third of the patients referred to our unit did not meet the diagnostic criteria for tennis elbow. We believe we have used the appropriate methods to diagnose, and that our group of patients is representative of patients with severe tennis elbow. The group of patients included had a long duration of elbow pain, and had tried multiple treatments with disappointing results.
We elected to use VAS and patient satisfaction as the primary outcome measures. VAS is known to be a reliable instrument for scoring differences in pain over time. Nevertheless, it has its restrictions, as the scoring needs to be related to the same level of activity each time. Less pain often leads to an increased activity level, which sometimes induce more pain. At the 12-month follow-up, four patients were still on sick leave (10 patients at the start), and we believe this might explain why the mean VAS was still quite high at the end of the study. Using the VAS in combination with satisfaction with treatment, the results seem easier to evaluate.
As the secondary outcome measure, we used grip strength, which is considered the best objective outcome measure.20
The study design (crossover for group 2), made it impossible to investigate if multiple lidocaine + epinephrine injections would also improve the clinical results. This might be considered as a weakness of the study; however, our hypothesis when designing the study was that the local anaesthetic lidocaine plus epinephrine would have nothing but a temporary pain-relieving effect.
US and CD guided intratendinous injection technique has also been used by Connell et al. They have shown promising results using a dry-needle technique together with injection of autologous blood, with good clinical short-term results in 32/36 patients after a mean of 2 injections.9
Blind (not guided by US or CD) local injections have been used for treatment for many years. Corticosteroid injections are commonly used, with varying results.13 Mishra and Pavelko injected buffered platelet-rich plasma, using a “peppering” technique, and reported good clinical short-time results in 15 patients (81% improvement in VAS after 6 months). The injections were was preceded by an injection of local anaesthetic + epinephrine, and approximately 0.5 mL was injected into the area of maximum tenderness.11
With the results of the aforementioned studies in mind, it is tempting to believe that the intratendinous injection in itself, not the substance injected, is of significant importance for the clinical result. US and CD guided injections reliably deposit the substance in the area with tendon changes, whereas the positioning of blinded injections seems more unreliable. Theoretically, the increased intra tendinous pressure caused by injecting a volume into the tendon might be responsible for the pain relieving effects.
In conclusion, we found that one US and CD guided intratendinous injection of the sclerosing substance polidocanol or the local anaesthetic lidocaine plus epinephrine gave pain relief in 50–62% of patients with tennis elbow. Additional injections with polidocanol in patients who were not fully satisfied improved the clinical results.
What is already known on this topic
Pain in patients with tennis elbow is elicited from the extensor origin at the lateral epicondyle.
Ultrasonography examination of the extensor origin in patients with tennis elbow shows structural changes.
Colour Doppler examination of the extensor origin in patients with tennis elbow shows increased blood flow.
What is already known on this topic
Ultrasonography and colour Doppler guided injections targeting the region with blood flow in the extensor origin at the lateral epicondyle gives pain relief in patients with tennis elbow.
Good clinical results were seen after both polidocanol and lidocaine plus epinephrine injections.
Acknowledgments
The Swedish Research Council for Sports funded the study.
REFERENCES
Footnotes
Competing interests: None.